Refeeding syndrome complete guide for emergency physician
Reading File
Finding Sources
Searching PubMed
"refeeding syndrome" AND management
Searching the Web
refeeding syndrome emergency medicine management 2024 2025 guidelines
Reading File
Reading File
Reading File
Reading Web Page
https://emcrit.org/ibcc/refeeding
Reading File
Reading File
Finding Sources
Reading Article
PMID: 40090863
Loading Image
Reading File
Finding Sources
I now have enough data from multiple authoritative sources to build a comprehensive guide. Let me compile it:
Refeeding Syndrome: Complete Guide for the Emergency Physician
1. Definition
Refeeding syndrome (RFS) is a potentially fatal metabolic disorder caused by the reintroduction of nutrition - oral, enteral, or parenteral - to patients who have been significantly malnourished or starved. It is characterized by severe fluid and electrolyte derangements, typically occurring within 72 hours of nutrition reintroduction.
The syndrome was first described after World War II, when severely malnourished Japanese prisoners were refed and developed sudden electrolyte crises and death. - Yamada's Textbook of Gastroenterology, 7th ed.
2. Pathophysiology
The core mechanism involves a critical metabolic shift from fat-based to carbohydrate-based fuel metabolism after refeeding.
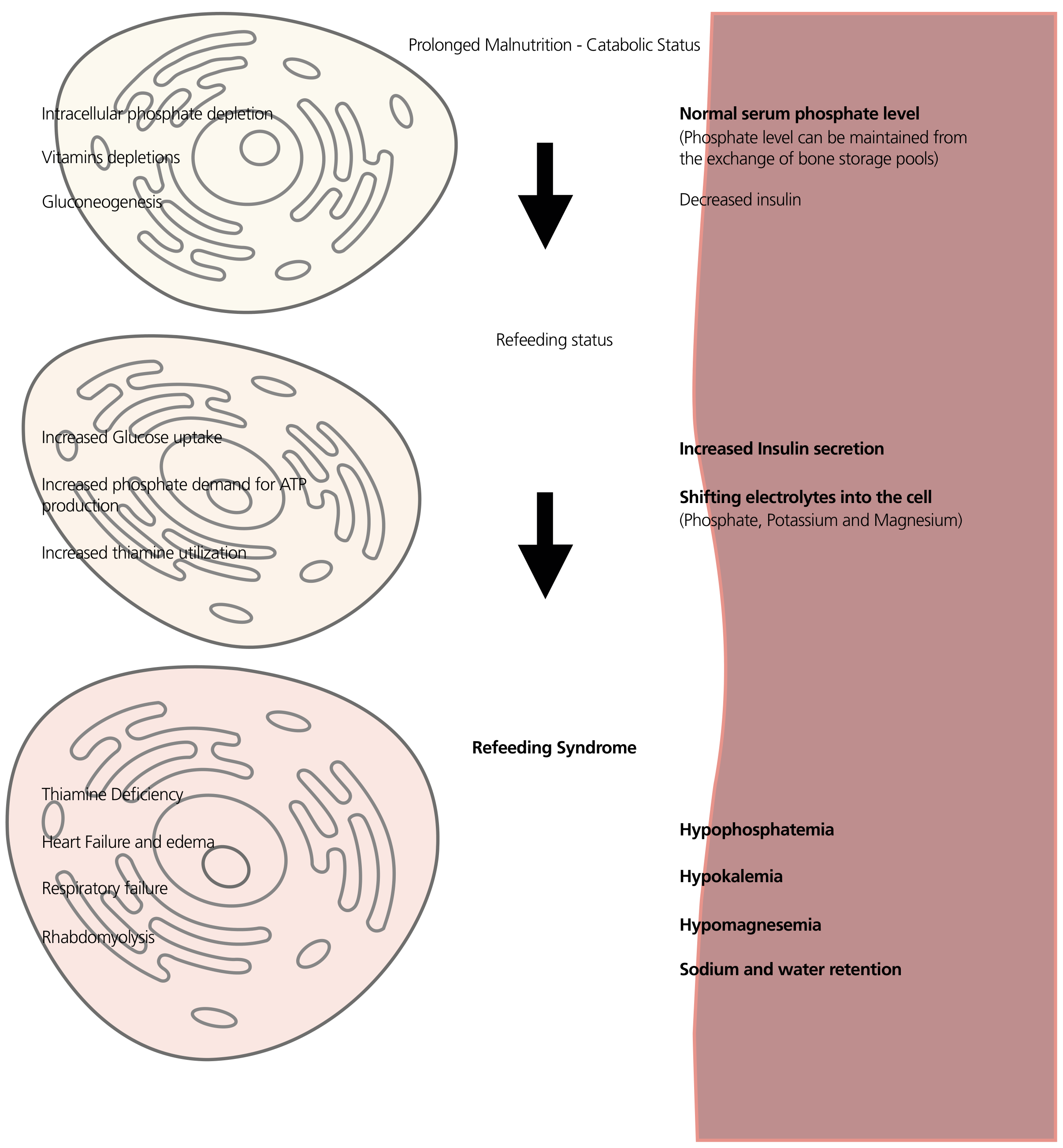
During starvation:
- Fatty acids and amino acids become the primary fuel sources
- Insulin levels fall
- Intracellular minerals (phosphate, potassium, magnesium) are progressively depleted
- Serum electrolyte levels can appear deceptively normal because bone stores maintain serum levels
On refeeding (the trigger):
- Carbohydrate load stimulates insulin secretion
- Insulin activates Na/K-ATPase - driving potassium (and phosphate, magnesium) into cells
- Phosphate is consumed intracellularly to synthesize ATP via glycolysis
- Thiamine (vitamin B1) is consumed as a cofactor for pyruvate dehydrogenase; without it, pyruvate cannot enter the Krebs cycle
- Sodium and water are retained, causing volume expansion
Result: Rapid and severe drops in serum phosphate (hallmark), potassium, and magnesium - all occurring against a background of total body depletion of these electrolytes. - Schwartz's Principles of Surgery, 11th ed.; Yamada's GI, 7th ed.
3. Who is at Risk? (NICE/ASPEN Criteria)
High Risk (ONE criterion sufficient - NICE 2006):
| Criterion | Threshold |
|---|---|
| BMI | < 16 kg/m² |
| Unintentional weight loss | > 15% in last 3-6 months |
| Little or no nutritional intake | > 10 days |
| Pre-existing low electrolytes | Potassium, phosphate, or magnesium LOW before feeding |
Moderate Risk (TWO criteria needed):
| Criterion | Threshold |
|---|---|
| BMI | 16-18.5 kg/m² |
| Unintentional weight loss | > 10% in last 3-6 months |
| Little or no nutritional intake | > 5 days |
| History of: alcohol abuse, insulin use, chemotherapy, antacids, or diuretics |
ASPEN Moderate/Significant Risk Table (Tietz Textbook of Laboratory Medicine, 7th ed.):
| Category | Moderate Risk (2 criteria) | Significant Risk (1 criterion) |
|---|---|---|
| BMI | 16-18.8 kg/m² | < 16 kg/m² |
| Weight loss | 5% in 1 month | 7.5% in 3 months OR >10% in 6 months |
| Caloric intake | < 75% of needs for > 7 days | < 50% of needs for > 5 days |
| Electrolytes | Minimally low or recently low requiring single-dose replacement | Moderately/significantly low or requiring multi-dose replacement |
| Comorbidities | Moderate disease, AIDS, cancer, chronic alcohol, post-bariatric | Severe loss/disease |
Key Clinical Populations to Screen in the ED:
- Anorexia nervosa / eating disorders (highest risk, also have QT prolongation)
- Chronic alcoholism
- Prolonged NPO patients (post-op, ICU)
- Cancer patients on chemotherapy
- Post-bariatric surgery patients
- Patients with prolonged diarrhea or high-output fistulas
- Obese patients with massive recent weight loss
- Prisoners on hunger strike
- Homeless / severely socially deprived individuals
4. Clinical Presentation
Timing: Symptoms typically begin 24-72 hours after refeeding initiation.
Organ System Breakdown:
| System | Manifestation |
|---|---|
| Cardiac | Arrhythmias (VT/VF), heart failure, edema, bradycardia (especially in anorexia) |
| Respiratory | Respiratory muscle weakness, failure to wean from ventilator, respiratory failure |
| Neurological | Confusion, encephalopathy, seizures, Wernicke's encephalopathy (thiamine deficiency), peripheral neuropathy |
| Musculoskeletal | Profound weakness, rhabdomyolysis |
| Hematologic | Hemolytic anemia, leukocyte dysfunction, platelet dysfunction |
| GI | Ileus, constipation |
| Metabolic | Hyperglycemia (from blunted insulin response in some), lactic acidosis |
| Fluid | Sodium and water retention, edema, acute volume overload |
The most severe presentations = cardiac arrhythmia or respiratory arrest. - Bailey & Love's Surgery, 28th ed.; Current Surgical Therapy, 14th ed.
5. Laboratory Abnormalities
Hallmark Finding:
Hypophosphatemia - the sine qua non of RFS. Levels can drop precipitously within hours of feeding. Severe = < 0.5 mmol/L (< 1.5 mg/dL).
Full Electrolyte Picture:
| Electrolyte | Direction | Why |
|---|---|---|
| Phosphate | ↓↓ (hallmark) | Intracellular shift for ATP synthesis |
| Potassium | ↓ | Na/K-ATPase activation by insulin |
| Magnesium | ↓ | Intracellular shift (mechanism incompletely understood); worsens hypokalemia |
| Calcium | ↓ | Linked to hypomagnesemia (impairs PTH release) |
| Glucose | ↑ or ↓ | Hyperglycemia from stress response; hypoglycemia risk if insulin excess |
| Sodium | Variable | Water retention can cause dilutional hyponatremia |
Other labs to order:
- ABG: lactic acidosis, respiratory compromise
- CK: rhabdomyolysis
- ECG: QT prolongation, arrhythmia detection
- Thiamine level (if available, but do not wait for result before dosing)
- LFTs, renal function, glucose
6. Clinical Definitions
ASPEN Definition (2020): RFS is diagnosed when the patient has had adequate nutrition intake (≥ 50% of estimated requirements), AND electrolyte imbalances and clinical symptoms emerge after its commencement. It should NOT be diagnosed from electrolyte changes alone without clinical correlation.
Practical ED definition: A drop of ≥ 30% in serum phosphate (or absolute level < 0.6 mmol/L) within 72 hours of refeeding, with or without clinical symptoms.
7. Emergency Management
Step 1: Identify at-risk patients BEFORE feeding
In the ED, screen every malnourished patient before initiating IV dextrose, enteral feeds, or TPN. Even a dextrose-containing IV bag can trigger RFS in a severely malnourished patient.
Step 2: Pre-refeeding workup
- Electrolytes (Na, K, Mg, Phos, Ca)
- Blood glucose
- Renal function
- ECG
- Thiamine level (order but don't wait)
Step 3: Thiamine FIRST
Give thiamine 100 mg IV BEFORE any glucose or carbohydrate. This is non-negotiable. Without thiamine, glucose loading causes Wernicke's encephalopathy (and precipitates lactic acidosis via pyruvate dehydrogenase blockade). - Tietz Lab Medicine, 7th ed.
- Standard: thiamine 100 mg IV x1 before feeds, then daily for 5-7 days
- High-risk (severe starvation, alcoholism): continue 100 mg IV daily x 5-7 days
Step 4: Correct pre-existing electrolyte deficits BEFORE or alongside feeding
Restore phosphate, potassium, and magnesium to normal before initiating significant caloric load.
Step 5: Start feeds slowly
| Risk Level | Initial Rate | Goal |
|---|---|---|
| Moderate risk | 10-20 kcal/kg/day | Increase gradually to full requirements over 4-7 days |
| High risk | Maximum 10 kcal/kg/day | Increase to 20 kcal/kg over 48h, then slowly to full needs |
| Highest risk (prolonged starvation, fistula losses) | < 10 kcal/kg/day OR 50% of estimated needs day 1 | Reach full needs over 5-7 days |
For parenteral nutrition: start with only 50% of the dextrose on day 1. - Yamada's GI, 7th ed.
Important 2025 update (AuSPEN Consensus): There is no evidence that patients at risk need to START at a lower-than-standard enteral feed rate for checking tolerance. Goal rates should be reached within 24-72 hours for most routes of nutrition. The key is close monitoring and electrolyte replacement, not necessarily severe caloric restriction for all patients.
Step 6: Electrolyte monitoring and replacement
Monitoring schedule:
- Electrolytes (phosphate, potassium, magnesium, calcium) at baseline, then at 6-12h after initiating feeds
- High-risk: twice-daily electrolytes for first 3 days
- Blood glucose every 4-6 hours initially
Replacement thresholds (approximate - follow local protocol):
| Electrolyte | Mild low | Moderate low | Severe low |
|---|---|---|---|
| Phosphate | 0.6-0.8 mmol/L - oral replacement | 0.4-0.6 mmol/L - IV replacement, slow feeds | < 0.4 mmol/L - aggressive IV, consider stopping feeds briefly |
| Potassium | 3.0-3.5 mEq/L - oral KCl | 2.5-3.0 mEq/L - IV replacement | < 2.5 mEq/L - continuous IV monitoring |
| Magnesium | 0.6-0.7 mmol/L - oral/IV | < 0.6 mmol/L - IV replacement | Refractory hypokalemia = suspect and treat hypoMg first |
Note: Hypomagnesemia will make hypokalemia refractory to replacement. Fix magnesium before potassium.
Step 7: Multivitamin supplementation
Give a multivitamin and trace elements daily for at least the first week of refeeding. B-complex vitamins are particularly important.
8. Established RFS: Treatment
If RFS develops after feeding has been started:
- Reduce or temporarily hold feeds - do not stop feeds entirely unless severe, as abrupt cessation causes hypoglycemia
- Aggressive IV electrolyte repletion - phosphate, potassium, magnesium simultaneously
- Continue thiamine supplementation
- Cautious insulin use - insulin further drives electrolytes into cells; use only for significant hyperglycemia (> 10-12 mmol/L) and with great care
- Manage volume overload - diuretics must be used with extreme caution (worsen potassium/magnesium losses); fluid restriction preferred
- Monitor and treat arrhythmias - ECG monitoring, correct electrolytes aggressively
- Respiratory support if muscle weakness causes ventilatory failure
- Treat rhabdomyolysis - IV fluids, monitor renal function and CK
9. ED-Specific Pitfalls
| Pitfall | Consequence | Fix |
|---|---|---|
| Starting dextrose IV in alcoholic without thiamine | Precipitates Wernicke's encephalopathy | Always give thiamine first |
| Normal electrolytes = no risk | False security - bone stores maintain serum levels until they collapse | Screen history + signs, not just labs |
| Assuming only TPN causes RFS | Even oral feeding, enteral nutrition, or dextrose-containing IV fluids can trigger it | Screen any nutritional input |
| Aggressive insulin for hyperglycemia in malnourished patient | Worsens intracellular electrolyte shift | Use insulin cautiously; fix electrolytes first |
| Correcting hypokalemia without correcting hypomagnesemia | Refractory hypokalemia | Correct Mg first or concurrently |
| Rapid hyponatremia correction in eating disorder patient | Osmotic demyelination syndrome | Correct slowly, < 8-10 mEq/L per 24h |
| QT prolongation in anorexia patients | Fatal ventricular arrhythmias | ECG in all eating disorder admissions; aggressive electrolyte correction |
10. Prognosis and Mortality
A 2021 systematic review and meta-analysis (PMID 33864767) confirmed RFS is associated with significant short- and medium-term all-cause mortality. Patients who develop actual RFS (as opposed to just electrolyte shifts) have substantially worse outcomes. The 2026 systematic review on risk prediction models (PMID 41793849) notes that ICU patients are at highest risk and that current risk models remain inadequately validated.
11. Quick Reference Card for the ED
SCREEN → Any malnourished patient getting feeds/IV dextrose
↓
LABS → BMP + Mg + Phos + ECG before starting
↓
THIAMINE → 100 mg IV BEFORE any glucose (non-negotiable)
↓
FIX LYTES → Correct K, Phos, Mg before or with feeding start
↓
START LOW → 10-20 kcal/kg/day max; 50% of EN rate day 1 for high risk
↓
MONITOR → Electrolytes q6-12h for first 72h; daily thereafter
↓
MULTIVIT → Thiamine + B-complex + trace elements daily x 1 week
↓
ESCALATE → If levels falling: reduce feeds, replace IV aggressively,
cardiac monitor, consider ICU
Sources:
- Bailey and Love's Short Practice of Surgery, 28th ed. - risk criteria, clinical features
- Schwartz's Principles of Surgery, 11th ed. - mechanism, management
- Current Surgical Therapy, 14th ed. - definition, timing, electrolyte pattern
- Yamada's Textbook of Gastroenterology, 7th ed. - pathophysiology diagram, management steps
- Tietz Textbook of Laboratory Medicine, 7th ed. - ASPEN risk stratification table, thiamine dosing
- AuSPEN Consensus 2025 (PMID 40090863) - updated guidance on feeding rates and diagnosis
- RFS mortality meta-analysis 2021 (PMID 33864767) - mortality impact
- EMCrit IBCC - Refeeding Syndrome (Josh Farkas, 2024) - EM-focused clinical framework
Damage control Resuscitation
Reading File
Finding Sources
Searching PubMed
"damage control resuscitation" AND trauma
Searching the Web
damage control resuscitation trauma 2024 2025 guidelines ATLS hemorrhagic shock
Reading File
Reading File
Reading File
Searching PubMed
tranexamic acid trauma hemorrhage mortality
Reading File
Reading File
Reading File
Loading Image
Reading File
Finding Sources
Finding Sources
Reading Article
PMID: 40842057
Reading File
Finding Sources
Finding Sources
I now have comprehensive data from multiple authoritative sources. Let me compile the complete guide:
Damage Control Resuscitation (DCR): Complete Guide for the Emergency Physician
1. Concept and Historical Context
Damage Control Resuscitation (DCR) - also called hemostatic resuscitation - is the modern paradigm for managing hemorrhagic shock in critically injured trauma patients. It replaced the historical approach of aggressive crystalloid-based resuscitation, which was associated with dramatically worse outcomes.
Origins: DCR emerged from military medicine in the 2000s (Iraq/Afghanistan conflicts), where fresh whole blood was used empirically in massively bleeding casualties. The success of military experience drove its translation to civilian trauma.
The core insight: While a patient is still actively bleeding, no aspect of the shock state - blood pressure, end-organ perfusion, temperature, or lactic acidosis - can be corrected by pouring in clear fluids. Volume resuscitation with crystalloids before hemostasis actively worsens coagulopathy, hypothermia, and acidosis. - Bailey and Love's Surgery, 28th ed.
ATLS 11th edition (2025) formalizes DCR as a core principle and introduces the xABCDE sequence - placing control of exsanguinating hemorrhage (x) before airway management, recognizing uncontrolled hemorrhage as the leading cause of preventable trauma death.
2. The Lethal Triad - Understanding What You're Fighting
The three mutually reinforcing killers in hemorrhagic trauma:
HYPOTHERMIA
↓ ↑
(worsens coagulation factor activity,
platelet function; reduces cardiac output)
↗ ↘
COAGULOPATHY ←→ ACIDOSIS
(tissue hypoxia, (dilutional, lactic;
dilution, factor further impairs
consumption) coagulation cascades)
- Hypothermia (core temp < 35°C): impairs coagulation factor activity and platelet function
- Acidosis (pH < 7.2): platelet morphology changes, declining factor activity, decreased thrombin generation
- Coagulopathy: results from tissue injury, dilution from crystalloids, consumption of factors, and hyperfibrinolysis
Large-volume crystalloid resuscitation before hemostasis directly causes all three legs of the lethal triad. DCR is specifically designed to prevent their development. - Mulholland & Greenfield's Surgery, 7th ed.
3. Four Pillars of DCR
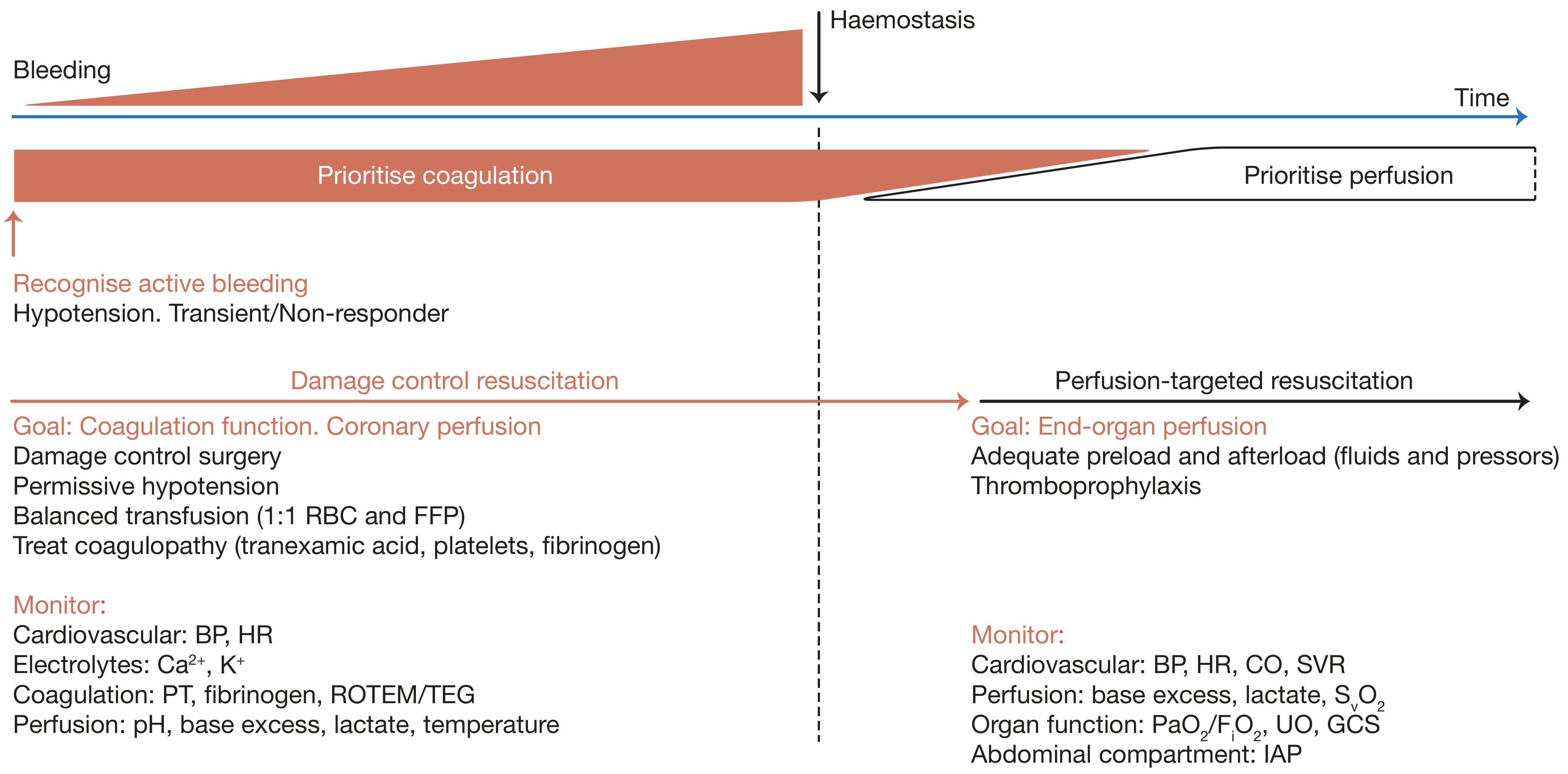
DCR applies only while the patient is actively bleeding. Once haemostasis is achieved, the strategy shifts to perfusion-targeted resuscitation. - Bailey and Love's Surgery, 28th ed.
Pillar 1: Rapid Hemorrhage Control (Stop the Bleeding First)
This is the overriding priority at every moment.
| Location | Intervention |
|---|---|
| External extremity | Tourniquet (high and tight, 2-3 inches above wound) |
| Junctional (groin, axilla, neck) | Wound packing with hemostatic gauze + direct pressure |
| Pelvis | Pelvic binder |
| Intracavitary (chest/abdomen) | Immediate OR / damage control surgery |
| Non-compressible torso hemorrhage | REBOA (Resuscitative Endovascular Balloon Occlusion of the Aorta) - at select centers |
In the abdomen (Damage Control Surgery): Pack, control bleeding, limit contamination, leave abdomen open, bring to ICU. Definitive repair is deferred. Standard criteria: major abdominal vascular injury + any two of: coagulopathy, acidosis, hypothermia.
Pillar 2: Permissive Hypotension
The concept: Deliberately accept a lower-than-normal blood pressure until surgical hemostasis is achieved. Aggressive fluid resuscitation raises blood pressure, which can "pop the clot" and worsen hemorrhage.
| Parameter | Target |
|---|---|
| Systolic BP (penetrating trauma) | 80-90 mmHg |
| MAP (general) | ~50-65 mmHg |
| Duration | Only until definitive hemorrhage control |
Critical exceptions - do NOT use permissive hypotension in:
- Traumatic brain injury (TBI) - cerebral perfusion pressure must be maintained; MAP > 80 mmHg
- Elderly patients - more likely to have cardiac and carotid disease; hypotension causes catastrophic ischemia
- Blunt trauma (relative caution vs. penetrating)
- Spinal cord injury
Mulholland & Greenfield's Surgery, 7th ed.
Pillar 3: Hemostatic Resuscitation (Blood Products, Not Crystalloids)
Minimize crystalloids. Crystalloids dilute clotting factors and cause dilutional coagulopathy, hypothermia, and abdominal compartment syndrome.
Use blood products early, in balanced ratios.
The 1:1:1 Ratio (PROPPR Trial)
- FFP : Platelets : pRBCs = 1:1:1
- This approximates whole blood's coagulation function
- The landmark PROPPR RCT (Holcomb et al., JAMA 2015) showed 1:1:1 vs 1:1:2 reduced 24-hour and 30-day mortality and increased rates of hemostasis
- More recent evidence confirms improved survival with 1:1 plasma:pRBC ratios, especially when given in the first 6-12 hours
Whole Blood (WB)
- If available: low-titer cold-stored whole blood is superior to component therapy (provides all elements in physiologic ratios)
- Used routinely in military settings; increasingly available in civilian trauma centers
- The gold standard when available; component therapy is a substitute
Cryoprecipitate
- Rich in fibrinogen, Factor VIII, vWF, Factor XIII
- Used as adjunct when hyperfibrinolysis depletes fibrinogen
- Also acts as low-volume colloid
- Fibrinogen target: > 1.5-2.0 g/L
Calcium Replacement
- Massive transfusion causes citrate chelation of calcium - profound hypocalcemia worsens cardiac function and coagulation
- Give calcium chloride 1g IV after every 4 units of blood products, or as guided by iCa++
- Target ionized calcium > 1.1 mmol/L
The Role of Hypertonic Saline
- Draws water into vascular space with small volume (especially 7.5% or 5% NaCl)
- Potential immune-modulating effects reducing resuscitation injury
- Theoretical advantages in TBI (reduces cerebral edema)
- A multicenter RCT was halted early due to no survival difference; small subset without transfusion requirement had higher mortality with HTS
- Current use: limited; considered as a one-time bolus in select patients, particularly TBI
Pillar 4: Treating Existing Coagulopathy
Tranexamic Acid (TXA) - The Most Important Drug in DCR
Mechanism: Antifibrinolytic - blocks plasminogen binding to fibrin, preventing clot breakdown. Trauma causes acute hyperfibrinolysis in 20-30% of patients.
Dosing:
- 1g IV over 10 minutes within 3 hours of injury, followed by 1g IV over 8 hours (CRASH-2 protocol)
- Alternative (NAEMSP/ACEP/ACS-COT 2025): 2g IV push (single dose, prehospital friendly)
- Must be given within 3 hours of injury - after 3 hours, TXA is ineffective and may increase mortality
Evidence:
- CRASH-2 trial (20,000+ patients): relative reduction in all-cause mortality and hemorrhage death
- 2024 meta-analysis (PMID 37999653): TXA reduces mortality in traumatic hemorrhage in emergency settings
- 2025 EAST PMG (PMID 40956301): strong evidence supporting TXA in injured patients at risk of hemorrhage
- 2025 Joint Position Statement - NAEMSP/ACEP/ACS-COT (PMID 40842057): recommends prehospital TXA for hemorrhagic shock, either 1g + 1g or 2g dose, within 3 hours
TXA in the ED: Give immediately at triage in any patient with hemorrhagic shock - do not wait for labs. Time to administration matters more than precise timing.
Prothrombin Complex Concentrate (PCC) and rFVIIa
- 4-factor PCC (25-50 units/kg): rapid reversal of anticoagulant-associated coagulopathy; cost-effective second-line agent in MTP
- rFVIIa: activates Factor Xa at injury site via tissue factor on platelets; early studies promising but larger RCTs did not confirm mortality benefit; role now limited to refractory coagulopathy
- FFP (preferred first line over PCC in most civilian protocols)
4. Massive Transfusion Protocol (MTP)
An MTP is a predefined, activated protocol that brings blood products rapidly to the bedside in pre-packaged cooler packs (typically in 1:1:1 ratios). Implementing an MTP is now required by the American College of Surgeons for all verified trauma centers.
Predicting the Need for MTP - Scoring Tools
| Score | Variables | Threshold for MTP Activation |
|---|---|---|
| ABC Score (Assessment of Blood Consumption) | HR > 120, SBP ≤ 90, penetrating mechanism, FAST positive | ≥ 2 points = activate |
| TASH Score | Hgb, SBP, HR, FAST, fracture, lactate, sex | ≥ 16 = high probability |
| Clinical gestalt | Transient or non-responder to initial resuscitation | Activate early, don't wait |
Key principle: Activate MTP early and based on mechanism + hemodynamics. Do not wait for lab results. De-escalate once hemostasis achieved and labs guide further therapy.
5. Viscoelastic Testing: TEG and ROTEM
Conventional coagulation tests (PT, aPTT, INR) are unreliable in trauma - they are performed at physiologic pH and temperature, failing to account for the effects of hypothermia and acidosis on in-vivo coagulation. They also cannot detect hyperfibrinolysis.
Thromboelastography (TEG) and Rotational Thromboelastometry (ROTEM) are point-of-care viscoelastic tests that:
- Provide a dynamic real-time view of clot formation, strength, and lysis
- Detect coagulation factor deficiencies, platelet dysfunction, and fibrinolysis
- Give results in 5-15 minutes
- Guide targeted resuscitation - reduce unnecessary blood product use and direct specific factor replacement
- Are more accurate than conventional labs in predicting massive transfusion requirements
Mulholland & Greenfield's Surgery, 7th ed.; Morgan & Mikhail's Clinical Anesthesiology, 7th ed.
| TEG Parameter | Deficit | Product to Give |
|---|---|---|
| Prolonged R-time | Factor deficiency | FFP |
| Prolonged K-time / Low alpha angle | Fibrinogen deficit | Cryoprecipitate |
| Low MA (max amplitude) | Platelet dysfunction | Platelets |
| Elevated LY30 / Clot lysis | Fibrinolysis | TXA |
| Hypercoagulable pattern | Clot present, bleeding controlled | Adjust ratios down |
When TEG/ROTEM is available: transition from empiric 1:1:1 to goal-directed component therapy once bleeding is controlled.
6. Endpoints of Resuscitation
Vital sign normalization is not sufficient. Up to 82% of severely injured patients with normalized vital signs have ongoing occult ischemia. - Mulholland & Greenfield's Surgery, 7th ed.
| Endpoint | Target | Notes |
|---|---|---|
| Lactate | < 2 mmol/L (trending down) | Best marker of oxygen debt clearance |
| Base deficit | > -6 mEq/L | Severity correlates with mortality |
| pH | > 7.35 | |
| Temperature | > 36°C | Active warming throughout |
| Ionized calcium | > 1.1 mmol/L | Replace aggressively |
| Fibrinogen | > 1.5-2.0 g/L | |
| Urine output | > 0.5 mL/kg/hr | Only after hemorrhage controlled |
| Mixed venous O2 (SvO2) | > 65% | Even with normal vitals - detects ongoing shock |
| Platelet count | > 50,000/µL (> 100,000 if TBI) | |
| INR | < 1.5 |
7. Managing the Lethal Triad Specifically
Hypothermia (core temp < 35°C)
- Remove all wet clothing immediately
- Warm all IV fluids (blood products through fluid warmer - mandatory for high-volume transfusion)
- Warm IV fluids and blood products: target > 37°C infusion temperature
- External warming blankets (Bair Hugger)
- Warm humidified oxygen
- Warm the resuscitation bay
- Rewarming via warmed peritoneal lavage or CRRT in extreme cases
Acidosis
- Treat the cause (hemorrhage control + restore perfusion)
- Bicarbonate not recommended as primary therapy - does not correct underlying tissue hypoxia and can worsen cellular acidosis
- Correct with restoration of perfusion (lactate clearance is the guide)
Coagulopathy
- TXA early
- Balanced blood products (1:1:1)
- Calcium replacement
- Cryoprecipitate if fibrinogen low
- Warm products to prevent worsening hypothermia-driven coagulopathy
- TEG/ROTEM guided therapy once available
8. ED-Specific Workflow
SCENE / PREHOSPITAL
├─ Tourniquet / wound pack / pelvic binder
├─ TXA 1g IV (or 2g) if shock + < 3h from injury
└─ Minimum fluids (no crystalloid boluses)
↓
TRAUMA BAY ARRIVAL (xABCDE - ATLS 11)
x → Control exsanguinating hemorrhage FIRST
A → Airway
B → Breathing
C → Circulation (not "give 2L NS" - activate MTP)
D → Disability (GCS, pupils)
E → Exposure + environment (cut off all clothes, warm)
↓
SIMULTANEOUS ACTIONS (first 5 minutes)
• Activate MTP if: transient/non-responder, SBP < 90,
HR > 120, penetrating, FAST+
• TXA if not given prehospital (< 3h window!)
• Start 1:1:1 blood products - NO crystalloid boluses
• Warm ALL blood products via fluid warmer
• FAST exam + portable CXR + pelvic XR
• Calcium chloride 1g IV
• Permissive hypotension: target SBP 80-90
(unless TBI → maintain MAP > 80)
↓
HEMORRHAGE CONTROL
• FAST positive → OR (damage control laparotomy)
• Pelvic fracture → IR (angioembolization) or pelvic packing
• Chest hemorrhage → thoracostomy / thoracotomy
• REBOA (Zone I or III) if available and indicated
↓
MONITOR & TITRATE
• ABG: pH, lactate, base deficit, Ca++, Hgb
• TEG/ROTEM → transition to goal-directed therapy
• Temperature: active warming
• De-escalate MTP when hemostasis confirmed
↓
POST-HEMOSTASIS: Switch to Perfusion-Targeted Resuscitation
• Now target MAP > 65 (or > 80 if TBI)
• Adequate preload and afterload
• Thromboprophylaxis (24-48h post injury)
• Abdominal compartment pressure monitoring
9. Special Populations and Exceptions
| Population | Modification |
|---|---|
| TBI | NO permissive hypotension; MAP > 80 mmHg; target normocapnia; avoid hyponatremia |
| Elderly | Higher baseline BP; "normal" SBP 100-120 may be relatively hypotensive; lower threshold for MTP |
| Anticoagulated patients | 4-factor PCC to reverse anticoagulation rapidly; reversal agent if DOAC-related |
| Pediatrics | TXA: if used, within 3h of injury; weight-based blood product dosing; no standardized MTP threshold |
| Pregnancy | Higher baseline blood volume; fetal monitoring; uterine displacement; 1:1:1 applies |
| Penetrating cardiac | ED thoracotomy if signs of life lost within 15 min in penetrating; 1:1:1 + aortic cross-clamp |
10. Abdominal Compartment Syndrome (ACS) - The Complication of Over-Resuscitation
Paradoxically, DCR also helps PREVENT ACS - which was common with aggressive crystalloid resuscitation.
- Definition: Sustained intra-abdominal pressure (IAP) > 20 mmHg + new organ dysfunction
- Intra-abdominal hypertension: IAP ≥ 12 mmHg
- Measure via: Foley catheter - transduced bladder pressure
- Manifestations: Oliguria, hypoxia (elevated diaphragm), cardiac failure, ileus
- Treatment: Decompressive laparotomy with temporary abdominal closure (wound VAC)
The incidence of ACS is falling with adoption of DCR - confirming crystalloids as the iatrogenic driver. - Mulholland & Greenfield's Surgery, 7th ed.
11. Key Evidence Base
| Trial / Guideline | Finding |
|---|---|
| CRASH-2 (2010) | TXA ≤ 3h reduces mortality in hemorrhagic trauma; after 3h, increases mortality |
| PROPPR Trial (Holcomb, JAMA 2015) | 1:1:1 vs 1:1:2 FFP:PLT:pRBC - improved 24h and 30d mortality; better hemostasis |
| PAMPer Trial (2018) | Prehospital FFP reduced 30-day mortality vs standard care |
| EAST PMG 2025 (PMID 40956301) | Strong evidence for TXA in injured patients at hemorrhagic risk |
| NAEMSP/ACEP/ACS-COT 2025 (PMID 40842057) | Prehospital TXA reduces mortality; 1g+1g or 2g dose within 3h |
| TEG/ROTEM meta-analysis (PMID 33769424) | Viscoelastic testing guides DCR more precisely than standard labs |
| AAST/ACS Protocol 2024 | Evidence-based DCR protocol: hemorrhage control + hypotensive resuscitation + hemostatic products + adjuncts |
12. Common Pitfalls
| Pitfall | Consequence | Fix |
|---|---|---|
| "2L NS first" reflex | Dilutional coagulopathy, worsens lethal triad | Activate MTP, give blood products instead |
| Delaying TXA while waiting for labs | Missed 3-hour window = no benefit or harm | Give TXA at triage if mechanism + hemodynamic instability |
| Permissive hypotension in TBI | Cerebral herniation, secondary injury | Target MAP > 80 in confirmed or suspected TBI |
| Treating acidosis with bicarbonate | Worsens cellular acidosis, no outcome benefit | Fix perfusion (stop bleeding, restore blood) |
| Giving saline for hypocalcemia | Hyperchloremic acidosis | Use calcium chloride |
| Rewarming too slowly | Coagulopathy persists despite products | Warm fluids, warm room, external warmers from the start |
| Over-resuscitating post-hemostasis | Abdominal compartment syndrome, pulmonary edema | Transition to guided, restrictive resuscitation after hemostasis |
| Continuing 1:1:1 after bleeding controlled | Unnecessary blood product exposure | Switch to TEG/ROTEM-guided therapy |
Sources:
- Mulholland & Greenfield's Surgery, 7th ed. - lethal triad, DCR components, TEG/ROTEM, endpoints
- Bailey and Love's Short Practice of Surgery, 28th ed. - four DCR pillars, DCR diagram
- Sabiston Textbook of Surgery, Biological Basis (latest ed.) - DCR components, origins
- Morgan & Mikhail's Clinical Anesthesiology, 7th ed. - DCS/DCR anesthesia perspective, TEG use
- Rockwood & Green's Fractures in Adults, 10th ed. (2025) - DCR in orthopaedic trauma
- AAST/ACS DCR Clinical Protocol 2024 - evidence-based DCR recommendations
- NAEMSP/ACEP/ACS-COT TXA Position Statement 2025 (PMID 40842057) - prehospital TXA guidance
- EAST PMG TXA 2025 (PMID 40956301) - systematic review + practice guideline
- TEG/ROTEM Systematic Review (PMID 33769424) - viscoelastic testing in DCR
- ATLS 11th edition (2025) - xABCDE, DCR formalized
This is a shared conversation. Sign in to Orris to start your own chat.