Discuss the indications, operative steps and complications of laparoscopic TEP repair for inguinal herni
laparoscopic TEP repair inguinal hernia indications operative steps complications
Laparoscopic TEP (Totally Extraperitoneal) Repair for Inguinal Hernia
Overview
I. INDICATIONS
Absolute / Clear Indications (Grade A - IEHS/EHS guidelines)
- Bilateral inguinal hernias - TEP allows repair of both sides through the same access without additional incisions, making it the preferred approach
- Recurrent inguinal hernia after prior open anterior repair (Lichtenstein, Shouldice, etc.) - the TEP approach accesses a virgin preperitoneal plane, avoiding dissection through scarred anterior tissue. The IEHS guidelines give a Grade A recommendation that TEP and TAPP are preferred alternatives to Lichtenstein for recurrent hernias after open anterior repair
- Unilateral primary inguinal hernia - TEP is a valid and preferred alternative to open mesh repair when the surgeon has adequate experience
- Symptomatic hernias requiring repair (direct, indirect, femoral) - any type of groin hernia can be addressed
Additional Preferred Indications
- Bilateral repair at time of another laparoscopic procedure (e.g., laparoscopic prostatectomy) - concurrent repair can be considered when there is no gross contamination
- Young active patients - faster return to work and daily activity
- Patients where chronic post-operative inguinal pain (CPIP) is a concern - laparoscopic repair results in the lowest risk of CPIP compared to open techniques
- Femoral hernias - excellent exposure of the femoral canal is a natural advantage of the preperitoneal approach
Contraindications to TEP (open repair preferred)
- General anesthesia contraindicated - laparoscopic repair requires general anesthesia; patients who cannot tolerate it should have open repair under local/regional anesthesia
- Prior pelvic/lower midline surgery - previous surgery in the space of Retzius, prostatectomy, or pelvic radiation may scar the preperitoneal space, making safe dissection hazardous (TAPP may still be feasible; open is preferred if both are unsafe)
- Multiple prior abdominal surgeries affecting the preperitoneal space
- Uncorrected coagulopathy
- Incarcerated/strangulated hernia with suspected bowel non-viability - requires open approach for bowel inspection
- Large inguinoscrotal hernias (relative) - highly complex, risk of conversion is significant
- Prior extraperitoneal/preperitoneal repair (failed TEP/TAPP) - subsequent repair should use an open anterior approach through a virgin plane
II. OPERATIVE STEPS
Patient Preparation and Positioning
- General anesthesia is mandatory (intra-abdominal CO₂ insufflation is not tolerated awake)
- Patient placed supine in Trendelenburg position (10-15 degrees) to allow bowel to fall away from the pelvis
- Arms tucked to the sides
- Bladder decompressed with urethral catheter (optional but reduces bladder injury risk)
- Surgeon stands contralateral to the hernia side; assistant stands opposite
- Video screens placed at the foot of the bed
Trocar Placement
| Trocar | Size | Position |
|---|---|---|
| Camera port (T1) | 10-12 mm | Infraumbilical midline, just below umbilicus |
| Working port (T2) | 5 mm | Midline, midway between umbilicus and pubis |
| Working port (T3) | 5 mm | Midline, just above pubic symphysis |
Step-by-Step Technique
- A 1.5-2 cm infraumbilical midline incision is made down to the anterior rectus sheath
- The anterior rectus sheath is incised, and the rectus abdominis muscle is retracted laterally
- The posterior rectus sheath is identified and the preperitoneal space (space between posterior rectus sheath and peritoneum) is entered bluntly with a finger or a balloon dissector
- The camera port trocar is placed and CO₂ insufflation to 8-12 mmHg creates the working space (some surgeons use a structural balloon trocar/dissecting trocar for initial space creation)
- A dissecting balloon or the 10-mm laparoscope itself is used to develop the preperitoneal space
- Blunt dissection is directed inferiorly toward the pubic symphysis and Cooper's ligament
- The two working trocars (T2 and T3) are inserted under direct vision in the midline
- Identify and dissect the pubis across the midline and Cooper's ligament (Zone 2) - if a large direct hernia is present, dissect to the contralateral Cooper's ligament
- Rule out a direct hernia by removing extraneous fat in Hesselbach's triangle
- Dissect at least 2 cm between Cooper's ligament and the bladder (Space of Retzius) - ensures inferior mesh overlap and avoids bladder distension displacing mesh; be cautious of the corona mortis (anastomosis between inferior epigastric and obturator vessels crossing Cooper's ligament)
- Rule out a femoral hernia by dissecting between Cooper's ligament and the external iliac vein (Zone 3) - femoral canal must be visualized
- Dissect the peritoneal/indirect hernia sac off the spermatic cord/round ligament - cord should lay flat; if the sac is large, it is transected and the distal portion left open to prevent hydrocele
- Identify the vas deferens crossing the external iliac vein in Zone 3 (medial structure)
- Identify the spermatic vessels running laterally in Zone 1 (lateral to the internal ring)
- Identify the psoas muscle posteriorly in Zone 1
- Ensure the peritoneal flap is fully mobilized inferiorly with adequate room for mesh
- Direct hernia sac: The peritoneal pseudosac is reduced by blunt dissection; direct sac does not need formal excision; can be fixed/inverted to Cooper's ligament to prevent seroma/hematoma
- Indirect hernia sac: Grasped and elevated superiorly from the cord, dissected from the cord with gentle traction and counter-traction; if large (inguinoscrotal), transected at the level of the internal ring - distal sac left open
- Femoral hernia sac: Reduced from the femoral canal
- The spermatic cord structures (vas deferens + testicular vessels) are dissected free of the peritoneum
- The peritoneum must be mobilized well inferiorly so that when mesh is deployed, it does not roll up
- The lateral space is developed to expose the psoas, iliac vessels, and lateral wall
- A flat, non-folded mesh of minimum 10 × 15 cm (or larger, up to 12 × 17 cm) is used to completely cover the myopectineal orifice
- The mesh is rolled or folded lengthwise and introduced through the 10-mm trocar
- It is unrolled and positioned to cover:
- The direct space (Hesselbach's triangle)
- The indirect space (internal ring)
- The femoral canal
- At least 2-3 cm overlap on Cooper's ligament inferiorly
- At least 3-4 cm beyond the pubic symphysis medially
- The mesh must lay completely flat without folding or rolling
- Many surgeons perform non-fixation (no tacks), particularly for direct hernias - evidence supports equivalent recurrence rates with lower chronic pain risk
- When fixation is used, tacks/staples are placed medially on Cooper's ligament and the posterior rectus sheath - never below the iliopubic tract laterally (danger zone for nerve injury - lateral femoral cutaneous nerve, femoral branch of genitofemoral nerve)
- Fibrin glue is an alternative with lower chronic pain rates
- For large direct defects, fixation to Cooper's ligament is standard
- CO₂ pressure is reduced slowly to check for peritoneal tears - any significant peritoneal rent should be closed with clips or endoscopic loops to prevent mesh contact with bowel
- The preperitoneal space is desufflated under vision, allowing mesh to be held in place by intraperitoneal pressure
- No peritoneal closure is required (key TEP advantage over TAPP)
- 10-mm port fascial defect is closed with absorbable suture
- Skin closed with subcuticular sutures
III. COMPLICATIONS
A. Intraoperative Complications
| Complication | Notes |
|---|---|
| Peritoneal tear | Most common intraoperative problem; small tears can be managed with clips; large tears may require conversion to TAPP or open; CO₂ leak into peritoneum collapses the working space |
| Vascular injury - inferior epigastric vessels | Most common vascular injury; occurs during trocar insertion or lateral dissection; usually controlled with diathermy or suture ligation |
| Vascular injury - iliac vessels/corona mortis | Potentially life-threatening; corona mortis (aberrant obturator artery from inferior epigastric) is at risk on Cooper's ligament; requires immediate control |
| Bladder injury | Occurs if bladder not decompressed and dissection is too medial in the Space of Retzius; recognized by pneumaturia or visible opening; requires repair |
| Bowel injury | Rare with TEP (advantage over TAPP); can occur with sharp dissection near peritoneal tears |
| Vas deferens injury | Can occur during cord skeletonization - irreversible; leads to infertility in males with bilateral injury |
| Conversion to open | Rate approximately 2-5%; indications: dense adhesions, uncontrolled bleeding, large peritoneal tears |
B. Early Postoperative Complications
| Complication | Incidence | Notes |
|---|---|---|
| Seroma | 4-8% (most common) | More common after large direct hernias; usually self-limiting; avoid aspiration unless symptomatic; resolves over weeks |
| Urinary retention | 3-5% | Due to Trendelenburg position, general anesthesia, pelvic dissection; catheterization usually resolves it |
| Rectus sheath hematoma | ~1.4% | From trocar insertion or injury to inferior epigastric vessels |
| Scrotal hematoma/ecchymosis | More common after large indirect sacs; bruising tracked along spermatic cord | |
| Wound infection | <1% | Lower than open repair; mesh infection is rare |
| Acute testicular pain | Related to handling of cord structures | |
| Trocar site hernia | Rare; umbilical fascial defect should be closed |
C. Late / Long-Term Complications
| Complication | Details |
|---|---|
| Chronic post-operative inguinal pain (CPIP) | Clinically significant CPIP in up to 12% overall; disabling daily pain 0.5-6%; LOWER with laparoscopic vs open repair; mechanism: nerve entrapment (ilioinguinal nerve not at risk in TEP as it is in open), tack fixation injury (lateral femoral cutaneous nerve, genitofemoral nerve), mesh contraction |
| Recurrence | 0.5-3%; causes include inadequate mesh size, mesh migration/folding, missed hernia defect (especially femoral), technical error, failure of fixation in large direct hernias |
| Testicular atrophy/ischemia | Rare (<0.5%); due to injury to testicular vessels during cord skeletonization |
| Mesh-related complications | Mesh infection (<0.1%); mesh migration; mesh shrinkage/contraction causing chronic pain; mesh erosion into adjacent structures (rare) |
| Sexual dysfunction/dysejaculation | Due to sympathetic plexus injury around vas deferens; ejaculatory pain |
| Osteitis pubis | Rare; from periosteal reaction at pubic symphysis fixation point |
| Adhesion/bowel obstruction | Very rare with TEP (significant advantage over TAPP); can occur with large peritoneal rents |
The "Triangle of Doom" and "Triangle of Pain" - Key Danger Zones
- Triangle of Doom: Bounded by the vas deferens medially and the spermatic vessels laterally, with the apex at the internal ring. Contains the external iliac artery and vein - no tacks or staples should ever be placed here
- Triangle of Pain: Lateral to the spermatic vessels, inferior to the iliopubic tract. Contains the femoral nerve, lateral femoral cutaneous nerve (LFCN), and femoral branch of the genitofemoral nerve - tacking in this zone causes chronic neuropathic pain and paresthesia
IV. TEP vs TAPP - Key Differences
| Feature | TEP | TAPP |
|---|---|---|
| Peritoneal entry | No | Yes |
| Bowel injury risk | Lower | Higher |
| Adhesion risk | Very low | Higher |
| Peritoneal closure | Not required | Required |
| Learning curve | Steeper | Less steep |
| Prior pelvic surgery | Difficult | Better access |
| Bilateral hernias | Both can be done | Both can be done |
| Conversion option | Can convert to TAPP | Can convert to open |
| General anesthesia | Required | Required |
V. Advantages of TEP Over Open Repair
- No violation of peritoneal cavity
- Lower chronic post-operative inguinal pain (CPIP)
- Faster return to work and normal activities
- Bilateral repair through same access
- Ideal approach for recurrent hernias after prior open anterior repair
- Better cosmesis (3 small midline incisions)
- Lower wound infection rates
- Lower risk to ilioinguinal nerve (not encountered in TEP)
- Fischer's Mastery of Surgery, 8th Edition, Chapter 223 (Inguinofemoral Hernia Repair), pp. 6090-6107
- Schwartz's Principles of Surgery, 11th Edition, Chapter 37 (Inguinal Hernias), pp. 1639-1645
- International Endohernia Society (IEHS) / HerniaSurge Group Guidelines 2018
- Ferzli et al., Laparoscopic TEP - ALES 2021 - comprehensive technical review
- Zaborowski et al., Perioperative outcomes of TEP repair, ALES - 403-patient series; seroma 4.2%, urinary retention 3.7%, rectus hematoma 1.4%
Recent advances in management of large incisional hernia.
incisional hernia repair advances
recent advances large incisional hernia management 2023 2024 2025 robotic component separation biologic mesh
transversus abdominis release TAR hernia abdominal wall reconstruction
PMID: 37329437
PMID: 39528659
PMID: 40360803
PMID: 38319440
PMID: 38632220
Recent Advances in Management of Large Incisional Hernia
Background
I. DEFINING "LARGE" INCISIONAL HERNIA AND RISK STRATIFICATION
Classification Systems
- Width: Small (<4 cm), Medium (4-10 cm), Large (>10 cm)
- Location: Midline (M1-M5) vs. lateral (L1-L4)
- Recurrent vs. primary
- Contamination class (CDC wound class I-IV)
Loss of Domain
Risk Assessment Tools
- Hernia-specific tools: Ventral Hernia Risk Score (VHRS), Ventral Hernia Working Group (VHWG) Grade
- General tools: American College of Surgeons NSQIP surgical risk calculator
- Key modifiable risk factors before elective repair: BMI >35, active smoking, HbA1c >8, malnutrition
II. PREOPERATIVE OPTIMIZATION - RECENT ADVANCES
1. Botulinum Toxin A (BTA) Injection - Major Recent Advance
- Mean lateral musculature advancement of 4.11 cm with low heterogeneity
- Low rates of SSI, surgical site occurrences, and recurrence post-repair
- BTA alone can "downstage" some hernias, enabling primary fascial closure with retromuscular mesh (Rives-Stoppa) without component separation
- Large hernias with anticipated difficult fascial closure
- Patients who may otherwise need component separation
- Loss of domain cases as preparation for abdominal wall reconstruction
2. Progressive Pneumoperitoneum (PPP)
3. Prehabilitation
- Smoking cessation (minimum 4-8 weeks pre-op)
- Weight loss / bariatric surgery for morbid obesity
- Glycemic optimization (HbA1c <8)
- Nutritional supplementation (albumin, micronutrients)
- Exercise programs to improve cardiopulmonary reserve
III. MESH TECHNOLOGY - RECENT ADVANCES
Classification of Mesh (ICAP 2019)
- Onlay: anterior to anterior rectus sheath
- Inlay: within the defect (bridging - largely abandoned for large hernias)
- Sublay (preferred):
- Retromuscular (posterior to rectus, anterior to posterior rectus sheath)
- Preperitoneal (anterior to peritoneum, posterior to posterior rectus sheath)
- Intraperitoneal (IPOM)
1. Lightweight Macroporous Polypropylene Mesh
2. Biologic Mesh (Bioprosthetics)
- Contaminated fields (CDC class III-IV) - main indication; biologic mesh can be used when synthetic mesh is contraindicated
- Very expensive with no proven superiority over synthetic mesh in clean cases
- Recent AHQC registry data (2024) show absorbable biosynthetic meshes (e.g., Phasix - poly-4-hydroxybutyrate, TIGR matrix) as an emerging middle-ground option for contaminated cases
3. Biosynthetic / Absorbable Synthetic Mesh
4. 3D-Printed / Patient-Specific Mesh
IV. COMPONENT SEPARATION TECHNIQUES - THE CENTRAL ADVANCE
1. Anterior Component Separation (ACS) - External Oblique Release (EOR)
- Originally described by Ramirez et al. in 1990
- External oblique aponeurosis divided 2 cm lateral to the linea semilunaris from rib to inguinal ligament
- Provides 3-10 cm of advancement per side (variable)
- Limitation: Requires large subcutaneous flaps → high wound complication rates (skin necrosis, seroma, SSI)
- Modification - Minimally Invasive ACS (MIS-EOR): Endoscopic or laparoscopic approach preserves perforating blood supply to skin, reducing wound complications (Saulis/Dumanian modification)
2. Posterior Component Separation - Transversus Abdominis Release (TAR) - The Dominant Current Technique
- Advancement of the posterior flap medially (up to 10 cm per side)
- Creation of a large retromuscular space for mesh placement
- Posterior rectus sheath released 2-3 mm medial to linea semilunaris, from subxiphoid to arcuate line
- Retrorectus space dissected laterally to linea semilunaris, protecting neurovascular bundles
- Deep inferior epigastric vessels identified and protected on dorsal rectus surface
- Posterior lamella of internal oblique divided, then transversus abdominis muscle/aponeurosis divided, entering the preperitoneal/pretransversalis space
- Dissection extended past midaxillary line, above costal margin (exposing diaphragm cranially, myopectineal orifices caudally)
- Posterior flaps reapproximated in midline with running suture
- Large uncoated mesh placed in the retromuscular space (trimmed to size)
- Anterior fascial layers closed
- Larger potential mesh overlap (the developed space is larger than with ACS)
- Mesh placed in retromuscular plane (best integration, lowest recurrence)
- No skin flaps required → lower wound complication rate
- Simultaneously addresses subcostal, subxiphoid, and groin hernias
3. Minimally Invasive / Robotic TAR
a) Extended Totally Extraperitoneal (eTEP) Approach
- Combines the retrorectus space development of TEP inguinal hernia repair with abdominal wall hernia repair
- Access is entirely extraperitoneal via small incisions
- Can be combined with TAR (eTEP-TAR or eTEP-RS for Rives-Stoppa)
- Avoids entering the peritoneal cavity entirely
b) Robotic TAR (rTAR)
| Outcome | rTAR | oTAR | p-value |
|---|---|---|---|
| Overall complications | 9% | 24.6% | <0.01 |
| Intraoperative complications | 5.9% | 9.1% | 0.02 |
| SSI | 2.5% | 7.8% | 0.01 |
| Fascial closure | 99% | 94.6% | 0.11 (NS) |
| Operative time | Longer | Shorter | <0.001 |
| Length of stay | -3.9 days shorter | Reference | <0.05 |
- Significantly longer operative time vs. open
- Higher direct costs
- No proven improvement in recurrence rates (Lima et al. 2024)
- Steep learning curve
- ROCSTAR trial ongoing - prospective RCT comparing robotic vs. open for wide abdominal wall hernias
V. MINIMALLY INVASIVE APPROACHES TO LARGE INCISIONAL HERNIA
1. Laparoscopic IPOM-Plus (Defect Closure with Intraperitoneal Mesh)
- IPOM-plus vs. IPOM: significantly lower recurrence (OR 0.51), seroma (OR 0.48), and mesh bulging (OR 0.08)
- Conclusion: Fascial closure with IPOM (IPOM-plus) is now considered the standard for laparoscopic ventral hernia repair when IPOM is chosen
2. Rives-Stoppa Open Retromuscular Repair
3. Enhanced View Totally Extraperitoneal (eTEP) Repair
- eTEP-RS: Rives-Stoppa bilateral retrorectus dissection
- eTEP-TAR: extended to include TAR for larger defects
- Benefits: no adhesiolysis required, no intraperitoneal mesh, no anti-adhesion barrier needed
VI. SYNTHETIC MESH PLANE PREFERENCE IN LARGE HERNIA REPAIR
| Mesh Position | Approach | Recurrence | SSO | Use in Large Defects |
|---|---|---|---|---|
| Bridging (inlay) | Open | Highest (50%+) | High | Only when fascia cannot be closed |
| Onlay | Open | High (10-20%) | High (skin necrosis, seroma) | Limited role |
| Retromuscular (Rives-Stoppa) | Open/Robotic | Low (4-10%) | Moderate | Gold standard for medium-large |
| Retromuscular + TAR | Open/Robotic | Low | Low (with robotic) | Gold standard for large/complex |
| IPOM-plus | Laparoscopic | Low-moderate | Moderate | Medium defects; less ideal for large |
VII. MANAGEMENT OF CONTAMINATED / COMPLEX CASES
Staged Repair
- Stage 1: Remove infected mesh, debride wound, achieve source control; abdominal closure with temporary mesh or negative pressure wound therapy (NPWT/VAC)
- Stage 2: Definitive repair at 6-12 months with biologic or biosynthetic mesh in a clean field
Negative Pressure Wound Therapy (NPWT/VAC)
Damage Control / Bridge Repair
- Reduce contents, treat bowel pathology
- Close fascia primarily if possible, or bridge with absorbable mesh
- Avoid permanent synthetic mesh in contaminated/emergency settings
- Definitive reconstruction planned as elective 2nd procedure
VIII. OUTCOMES MONITORING AND QUALITY METRICS
Patient-Reported Outcomes
- Carolinas Comfort Scale (CCS) - validated hernia-specific quality of life tool
- HerQLes questionnaire - abdominal wall function
- PROMIS scores
Registry-Based Learning
Key Quality Metrics
- Surgical Site Occurrence (SSO) rate
- SSO requiring procedural intervention (SSOPI)
- 30-day readmission
- Hernia recurrence at 1, 3, 5 years
- Patient-reported quality of life
IX. SUMMARY OF KEY RECENT ADVANCES
| Advance | Clinical Impact |
|---|---|
| Botulinum Toxin A preop | Stretches lateral muscles ~4 cm per side; enables fascial closure without or with lesser component separation |
| TAR (Posterior CS) | Lower SSO than anterior CS; enables large retromuscular space for mesh; preferred for large defects |
| Robotic TAR (rTAR) | Minimally invasive posterior CS; lower SSI and complications vs open; longer OR time; similar recurrence |
| eTEP approach | Fully extraperitoneal laparoscopic/robotic repair; avoids adhesiolysis; no anti-adhesion mesh needed |
| IPOM-Plus | Fascial closure during IPOM halves recurrence risk and seroma formation vs IPOM alone |
| Biosynthetic mesh | Slowly absorbable option for contaminated fields; emerging alternative to costly biologic mesh |
| 3D-printed mesh | Investigational; patient-specific geometry; limited evidence |
| NPWT/VAC | Wound management tool reducing SSI in contaminated repairs; mesh salvage protocol |
| ICAP classification | Standardized mesh plane terminology enabling consistent research and communication |
| Prehabilitation programs | Modifiable risk factor optimization reducing wound complications |
- Sabiston Textbook of Surgery, 21st Edition, Chapter 80 (Abdominal Wall Hernias), pp. 1648-1660
- Fischer's Mastery of Surgery, 8th Edition, Chapter 216 (Ventral Incisional Hernia), pp. 5907-5918
- Dias et al. Botulinum toxin for ventral hernia - Hernia 2023 (PMID 37329437) - SR/MA: 4.11 cm average muscle advancement
- Lima et al. Open vs robotic TAR - Surg Endosc 2024 (PMID 39528659) - SR/MA: rTAR lower complications, shorter LOS
- Demetrashvili et al. ACS vs TAR RCT - Updates Surg 2025 (PMID 40360803) - TAR: SSO 19% vs ACS 50%
- Huang et al. IPOM-plus SR/MA - Hernia 2024 (PMID 38319440) - IPOM-plus halves recurrence vs IPOM
- Tryliskyy et al. MIS PCS SR/MA - Hernia 2024 (PMID 38632220) - MIS TAR: SSE 13.4%, SSOPI 5.7%
- HerniaSurge Group International Guidelines, Hernia 2018
Describe the surgical anatomy of the anterior abdominal wall. Briefly discuss its importance in management of ventral hernia repair
surgical anatomy anterior abdominal wall layers muscles fascia nerves blood supply ventral hernia repair importance
Surgical Anatomy of the Anterior Abdominal Wall and Its Importance in Ventral Hernia Repair
I. BOUNDARIES AND SURFACE ANATOMY
- Superiorly: costal margins and xiphoid process
- Laterally: midaxillary lines (right and left)
- Inferiorly: symphysis pubis, pubic tubercles, inguinal ligaments, anterior superior iliac spines (ASIS), and iliac crests
II. EMBRYOLOGY
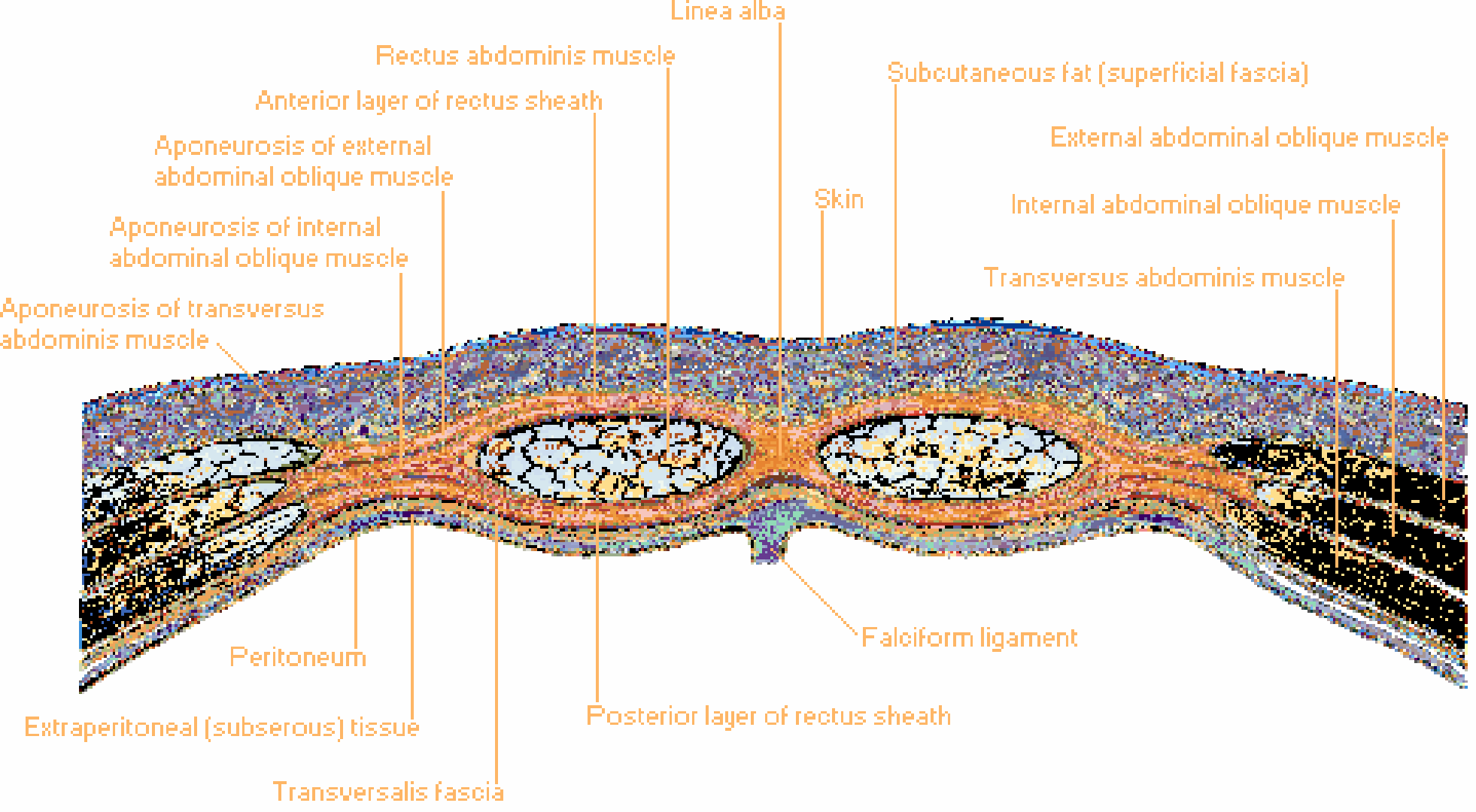
III. LAYERS OF THE ANTERIOR ABDOMINAL WALL (SUPERFICIAL TO DEEP)
| Layer | Notes |
|---|---|
| 1. Skin | Freely mobile over most of the wall |
| 2. Subcutaneous tissue | Variable thickness based on body habitus |
| 3. Superficial fascia (Camper's + Scarpa's) | Superficial fatty layer (Camper's); deep membranous layer (Scarpa's) below umbilicus |
| 4. External oblique muscle/aponeurosis | |
| 5. Internal oblique muscle/aponeurosis | |
| 6. Transversus abdominis muscle/aponeurosis | |
| 7. Transversalis fascia | Thin but important fibrous layer |
| 8. Preperitoneal adipose and areolar tissue | Contains the preperitoneal space |
| 9. Peritoneum | Innermost layer |
Superficial Fascia
- Above the umbilicus: Camper's and Scarpa's fasciae are fused as a single layer
- Below the umbilicus: They separate distinctly:
- Camper's fascia: outer fatty layer, continuous with superficial thigh fascia, extends to the scrotum in males and labia majora in females
- Scarpa's fascia: inner fibrous membranous layer, fuses with the anterior fascia of the flank and back; clinically important as it may limit spread of urinary extravasation
IV. MUSCULOAPONEUROTIC LAYERS
A. Rectus Abdominis (Paired Longitudinal Muscles)
- Origin: Pubic symphysis and crest
- Insertion: Xiphoid process, 5th-7th costal cartilages
- Features: Has 3 tendinous intersections along its length (attached to anterior sheath, not posterior sheath - allowing contents of posterior sheath to move freely)
- Enclosed within the rectus sheath, formed by the aponeuroses of the three lateral muscles
- Separated in the midline by the linea alba
B. Three Flat Lateral Muscles (obliquely oriented relative to each other)
- Origin: Lower 8 ribs (5th to 12th)
- Insertion: Linea alba (medially) and anterior iliac crest (laterally)
- Fiber direction: Inferomedially ("hands in pockets" direction)
- Most superficial of the three lateral muscles
- Lower free edge of its aponeurosis forms the inguinal ligament (Poupart's ligament) stretching from ASIS to pubic tubercle
- Origin: Thoracolumbar fascia, iliac crest, lateral two-thirds of inguinal ligament
- Insertion: Lower costal margin, xiphoid process; aponeurosis contributes to rectus sheath
- Fiber direction: Superomedially (perpendicular/opposite to EO - reinforcing lattice)
- Its bilaminar aponeurosis splits at the linea semilunaris to enclose the rectus above the arcuate line
- Origin: Costal margin, thoracolumbar fascia, iliac crest
- Fiber direction: Transverse/horizontal - the true "corset" muscle
- Insertion: Linea alba, xiphoid, pubic symphysis
- Its aponeurosis contributes to the posterior rectus sheath above the arcuate line
C. Pyramidalis
- Small triangular muscle lying anterior to the lower rectus, between the pubis and linea alba; often absent; tenses the linea alba
V. THE RECTUS SHEATH - Critical for Hernia Surgery
Above the Arcuate Line:
- Anterior sheath: EO aponeurosis + anterior lamella of IO aponeurosis
- Posterior sheath: Posterior lamella of IO aponeurosis + TA aponeurosis
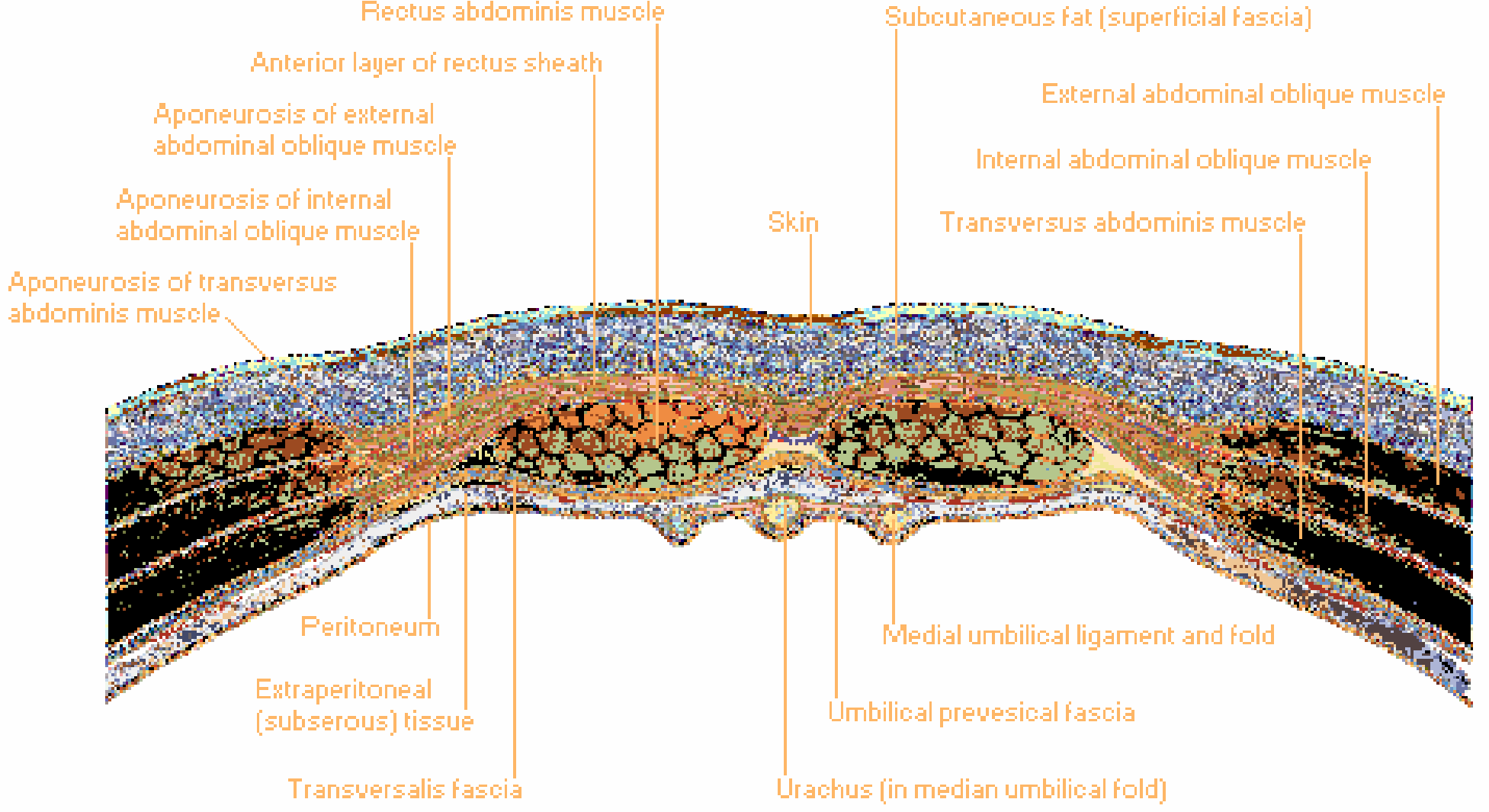
Below the Arcuate Line:
- Anterior sheath: All three aponeuroses (EO + IO + TA) pass anterior to the rectus
- Posterior sheath: ABSENT - only transversalis fascia remains posteriorly
VI. KEY ANATOMICAL LANDMARKS
Linea Alba
- Fibrous raphe formed by the interlacing aponeurotic fibers of all three lateral muscles from both sides fusing at the midline
- Extends from xiphoid process to pubic symphysis
- Width: 10-15 mm above the umbilicus, narrows to ~4 mm at umbilicus and below
- More well-defined and wider above the umbilicus - explaining why epigastric hernias are more common there (wider linea alba = greater chance of fascial defect)
- Progressively widens with age and pregnancy (diastasis recti)
- The principal structure repaired in ventral hernia surgery
Linea Semilunaris
- Curved line on the lateral edge of the rectus abdominis where the aponeuroses of the lateral muscles meet
- The point where neurovascular bundles pierce the posterior sheath to enter the rectus
- Spigelian hernias occur at or along this line
Arcuate Line (Linea Semicircularis / Douglas's Line)
- The free inferior margin of the posterior rectus sheath
- Located approximately midway between the umbilicus and pubis
- Below this line: All aponeuroses are anterior; only transversalis fascia posteriorly
- Critical for planning mesh position: the retrorectus space (Rives-Stoppa plane) extends from the xiphoid to this line in its natural state; TAR releases extend it further
Umbilicus
- A focal point of anatomical convergence where all layers of the abdominal wall fuse, creating a natural weak point
- Contains the obliterated urachus (median umbilical ligament), obliterated umbilical arteries, round ligament of liver (ligamentum teres), and paraumbilical veins
- The umbilicus is the most common site of spontaneous ventral hernia
Internal Surface Landmarks (Peritoneal Folds)
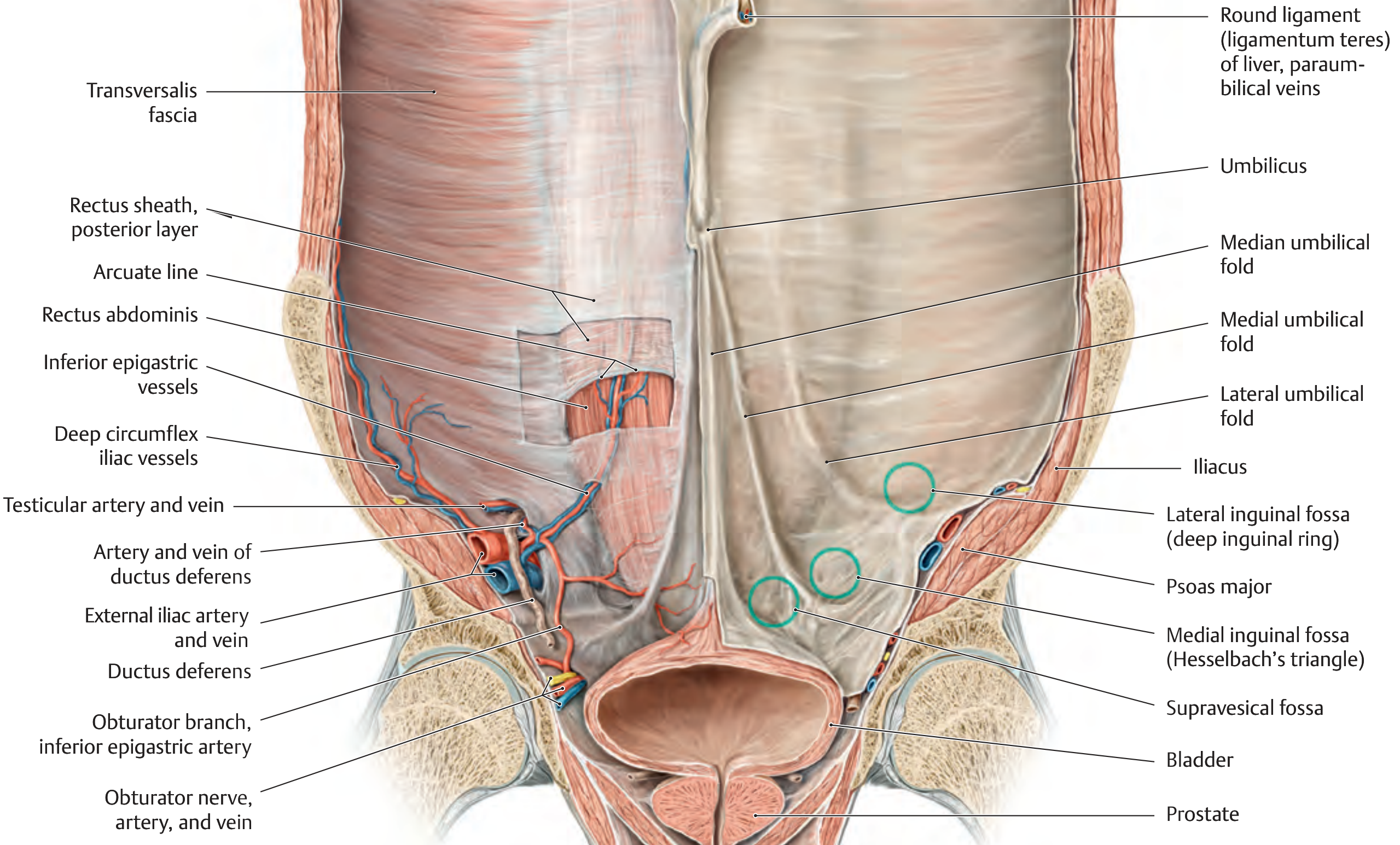
- Median umbilical fold (unpaired): contains the obliterated urachus
- Medial umbilical folds (paired): contain the obliterated umbilical arteries
- Lateral umbilical folds (paired): contain the inferior epigastric vessels - critical landmark separating direct from indirect inguinal hernias
- Supravesical fossa: between median and medial folds
- Medial inguinal fossa (Hesselbach's triangle): between medial and lateral umbilical folds - site of direct inguinal hernia
- Lateral inguinal fossa: lateral to the lateral umbilical fold - site of the deep inguinal ring (indirect inguinal hernia)
VII. TRANSVERSALIS FASCIA
- It forms the posterior boundary of the anterior abdominal wall below the arcuate line
- Contains the preperitoneal space between itself and the peritoneum
- Forms the internal spermatic fascia at the deep inguinal ring
- Its strength and integrity determine the quality of the preperitoneal plane for mesh placement in TEP and eTEP repairs
VIII. SURGICAL POTENTIAL SPACES
| Space / Plane | Location | Clinical Use |
|---|---|---|
| Subcutaneous plane | Between skin and anterior rectus sheath | Onlay mesh placement |
| Premusculofascial (subaponeurotic) plane | Between EO aponeurosis and IO | Minimally invasive anterior CS (EOR) |
| Retrorectus (Rives-Stoppa) space | Between rectus muscle and posterior rectus sheath | Gold standard sublay mesh position |
| TAR space | Between TA muscle and transversalis fascia, posterior to posterior sheath | TAR for large hernias; extends mesh overlap further laterally |
| Preperitoneal space | Between transversalis fascia and peritoneum | TAPP, TEP, eTEP hernia repair |
| Intraperitoneal space | Inside peritoneal cavity | IPOM repair |
IX. BLOOD SUPPLY
Zone I - Dominant Supply (Midline)
- Superior epigastric artery (SEA): terminal branch of the internal mammary artery, enters the rectus sheath posterosuperiorly
- Deep inferior epigastric artery (DIEA): branch of the external iliac artery, enters the rectus sheath posteroinferiorly
- Both lie on the posterior aspect of the rectus muscles and supply the rectus abdominis + skin/subcutaneous tissue through musculocutaneous perforators
- They anastomose within the rectus between the xiphoid and umbilicus
Zone II - Lateral Wall Supply
- Musculophrenic artery (from internal mammary)
- Deep circumflex iliac artery (from external iliac)
- Branches of the lower intercostal arteries (T7-T11) and lumbar arteries
- These vessel arcades run between the transversus abdominis and internal oblique muscles (the TAP plane)
Zone III - Inferior / Superficial Supply
- Superficial epigastric artery (from femoral artery)
- Superficial circumflex iliac artery
X. NERVE SUPPLY
- T7-T12: Lower intercostal nerves
- L1: Iliohypogastric and ilioinguinal nerves
- T7: Epigastrium
- T10: Umbilicus
- L1: Groin/inguinal region
XI. WEAK POINTS / SITES OF HERNIA FORMATION
| Site | Anatomical Basis | Hernia Type |
|---|---|---|
| Umbilicus | Convergence of all layers; obliterated umbilical structures | Umbilical hernia |
| Linea alba | Decussating aponeurotic fibers; wider above umbilicus | Epigastric hernia |
| Surgical incisions | Failed fascial healing; collagen defects | Incisional hernia |
| Deep inguinal ring | Lateral inguinal fossa; weakness in TA fascia | Indirect inguinal hernia |
| Hesselbach's triangle | Medial inguinal fossa; behind posterior inguinal wall | Direct inguinal hernia |
| Femoral ring | Below inguinal ligament, medial to femoral vein | Femoral hernia |
| Linea semilunaris | Junction of aponeuroses at lateral rectus sheath | Spigelian hernia |
| Obturator foramen | Obturator membrane defect | Obturator hernia |
| Lumbar triangles | Superior (Grynfeltt) and inferior (Petit) | Lumbar hernia |
XII. IMPORTANCE OF ANATOMICAL KNOWLEDGE IN VENTRAL HERNIA REPAIR
1. Understanding the Defect
- Knowledge of layers enables accurate classification of hernia location (midline vs. lateral, relation to arcuate line, linea semilunaris)
- Determines which fascial layers are deficient and what remains to close over
- The EHS classification system (M1-M5 midline, L1-L4 lateral) is anatomically based
- Defect dimensions (width, length) determine whether fascial closure is achievable and which approach is needed
2. Choosing the Correct Mesh Plane
- Onlay (anterior to anterior rectus sheath): simplest anatomically but high SSO
- Retrorectus (posterior to rectus, anterior to posterior sheath): ideal plane above arcuate line; widest natural clean space; no contact with bowel; allows excellent integration
- Below arcuate line: No posterior sheath; mesh must be in preperitoneal plane or placed with care to avoid bowel contact
3. Mesh Overlap Planning
4. Component Separation Decisions
- EOR (Anterior CS): Divides EO aponeurosis 2 cm lateral to linea semilunaris; provides 3-10 cm per side; disrupts perforators in subcutaneous flaps → wound complications
- TAR (Posterior CS): Divides posterior lamella of IO and TA; exploits the plane between TA and transversalis fascia; preserves all musculocutaneous perforators; provides up to 10+ cm per side; creates large retromuscular space for mesh
5. Preserving Neurovascular Bundles
6. Understanding the Arcuate Line in Surgical Planning
- The posterior sheath ends at the arcuate line; below this, mesh in the retrorectus space is in direct contact with peritoneum/preperitoneal fat without a fascial barrier
- During lower midline dissection (space of Retzius), anatomical knowledge prevents bladder injury
- The TAR space extends the retrorectus plane caudally past the arcuate line into the pelvis, reaching the myopectineal orifices - enabling simultaneous groin hernia management
7. Minimally Invasive and Robotic Approaches
- eTEP: Extraperitoneal access via the preperitoneal space requires precise understanding of the transversalis fascia plane, the arcuate line, and the retrorectus compartment
- Laparoscopic IPOM: Placing trocars safely requires knowing the inferior epigastric vessel positions (lateral umbilical folds) to avoid injury
- TEP inguinal hernia repair: Relies entirely on knowledge of the preperitoneal space anatomy
8. Preventing Incisional Hernia Formation
- Understanding why incisional hernias develop guides prophylactic measures:
- Midline laparotomy closure: Small bites technique (0.5 cm × 0.5 cm, 4:1 suture:wound ratio) based on the biomechanics of linea alba healing
- Transverse incisions have lower hernia rates than vertical (parallel to abdominal wall force vectors)
- Prophylactic mesh placement in high-risk patients (obese, COPD, previous hernia) at time of laparotomy is now evidence-based
9. Blood Supply Considerations for Wound Healing
- Large skin flaps during open repair disrupt perforating vessels → devascularized skin → necrosis, wound breakdown → SSI, mesh infection
- Choosing minimally invasive approaches (robotic TAR, eTEP) or minimizing skin flap extent preserves Zone III blood supply
10. Diastasis Recti vs. True Hernia
Summary Table: Anatomy and Its Surgical Relevance
| Anatomical Feature | Surgical Relevance in Ventral Hernia Repair |
|---|---|
| Linea alba | Primary structure repaired; wider above umbilicus explains epigastric hernias |
| Arcuate line | Defines extent of retrorectus space; mesh plane changes below it |
| Linea semilunaris | Lateral limit of retrorectus dissection; nerve entry point; Spigelian hernia site |
| Posterior rectus sheath | Creates retrorectus space for ideal mesh placement (Rives-Stoppa) |
| TA muscle plane | Divided in TAR to access preperitoneal space; key to large hernia repair |
| Transversalis fascia | Posterior barrier in preperitoneal space; exploited in TEP/eTEP |
| TAP (TA-IO plane) | Route of neurovascular bundles; plane for TAP block |
| DIEA | Landmark for inferior epigastric vessel preservation; basis for DIEP flap |
| SEA-DIEA anastomosis | Zone I perforators underlie rectus musculocutaneous flaps |
| Peritoneal folds | Identify hernia fossae; guide laparoscopic landmark recognition |
| Scarpa's fascia | May limit urinary extravasation spread; closed separately in lower abdomen wounds |
- Sabiston Textbook of Surgery, 21st Ed., Chapter 80 - Introduction and Anatomy, pp. 1647-1649
- Schwartz's Principles of Surgery, 11th Ed., Chapter 35 - Surgical Anatomy, pp. 1580-1583
- Netter's Atlas of Human Anatomy - Cross sections above and below arcuate line, pp. 404-405
- Thieme Atlas of General Anatomy and Musculoskeletal System - Section 5.8 Anterior Abdominal Wall, p. 233
- IntechOpen: Abdominal Wall Anatomy - Surgical Landmarks in Hernia Repair
Enumerate the factors responsible for incisional hernias
factors responsible for incisional hernia patient surgical technical risk factors 2024
incisional hernia risk factors etiology systematic review
PMID: 38519402
PMID: 36102959
Factors Responsible for Incisional Hernia
I. PATIENT-RELATED (PREOPERATIVE) FACTORS
A. Factors That Impair Wound Healing
- The single most important independent risk factor
- Increased intra-abdominal pressure exerted on the wound throughout healing
- Poor vascular supply to adipose tissue reduces oxygen delivery to wound
- Technically difficult wound closure - aponeuroses harder to approximate under tension
- Increased SSI risk due to poor perfusion and dead space in subcutaneous fat
- BMI >30 approximately doubles, and morbid obesity (BMI >40) quadruples, hernia risk
- Impaired neutrophil function, macrophage activation, and fibroblast proliferation
- Reduced collagen synthesis and cross-linking; reduced tensile strength of healed fascia
- Diminished angiogenesis and neovascularisation in the healing wound
- Increased SSI risk (hyperglycaemia suppresses immune response)
- HbA1c >8% is a recognised pre-operative modifiable risk factor
- Albumin <3.0 g/dL is an independent predictor of wound complications
- Inadequate amino acid availability impairs collagen synthesis
- Impaired immune function increases SSI risk
- Micronutrient deficiencies (zinc, vitamin C) directly impair collagen hydroxylation and cross-linking
- Nicotine causes peripheral vasoconstriction and reduces tissue oxygen tension
- Carbon monoxide displaces oxygen from haemoglobin (carboxyhaemoglobin)
- Reduces collagen synthesis; increases collagenase (MMP) activity
- Impairs chemotaxis and phagocytic function of neutrophils
- Cessation for at least 4-8 weeks pre-operatively substantially reduces risk
- Steroids suppress the inflammatory phase of wound healing (impair macrophage migration, fibroblast proliferation)
- Reduce collagen synthesis and cross-linking
- Cyclosporine, azathioprine, and other immunosuppressants used in transplant patients confer elevated risk
- Chemotherapy (especially within 6 weeks of surgery) impairs wound healing phases
- Reduced oxygen delivery to healing tissues, impairing oxidative reactions required for collagen synthesis
- Reduced skin and fascial tensile strength with ageing
- Impaired wound healing capacity - slower proliferative and remodelling phases
- Reduced synthesis of type I collagen; increased ratio of collagen type III:I (weaker)
- Frequently associated with multiple comorbidities that compound risk
B. Collagen Metabolism Disorders
- Collagen type I:III ratio is reduced in patients who develop hernias (systematic review, PMID 38519402 - Am J Surg 2024)
- Elevated Matrix Metalloproteinases (MMPs) - particularly MMP-2 - found to be upregulated in hernia tissue; MMPs degrade extracellular matrix collagen, weakening fascial strength
- Ehlers-Danlos syndrome, Marfan syndrome: inherent fascial weakness
- Patients with aortic aneurysms have underlying collagen/elastin defects - explaining their very high incisional hernia rates after aneurysm repair
- Prior laparotomies leave scar tissue that is biologically weaker than native fascia
- Abdominal radiation damages fibroblasts and vascularity, producing ischaemic, poorly healing tissue
- Each re-operation in the same field compounds the deficit
C. Factors That Increase Intra-Abdominal Pressure
- Chronic cough raises intra-abdominal pressure repeatedly during the healing period
- Direct mechanical stress disrupts forming fascial repair
- Associated hypoxia impairs wound healing at cellular level
- Repeated Valsalva-like manoeuvres elevate intra-abdominal pressure on the healing wound
- Straining during micturition raises intra-abdominal pressure
- Persistent elevation of intra-abdominal pressure directly stresses wound edges
- The fluid itself may compromise wound healing if infected or by reducing fascial blood flow
- Mechanical pressure from gravid uterus; hormonal changes also affect fascial remodelling
- Wider linea alba relative to body surface area
- Hormonal factors affect collagen composition
- Parity stretches the linea alba
II. OPERATIVE / TECHNICAL (INTRAOPERATIVE) FACTORS
A. Incision-Related Factors
- Midline (median) laparotomy has the highest incisional hernia rate of all incision types
- The midline cuts through the avascular linea alba - no muscle or nerve injury, but poor vascular supply = slow healing
- Lateral (oblique, transverse, grid-iron) incisions divide muscles with better intrinsic blood supply and heal with lower hernia rates
- Paramedian and transverse incisions have significantly lower hernia rates than midline
- Laparoscopic port sites are much less prone (1.5-1.8%) than open incisions
- Longer incisions have higher hernia rates than shorter incisions
- Longer wounds have greater wound tension and more area for fascial separation
- Upper midline hernias are more common than lower midline - the linea alba is wider above the umbilicus
- Below the arcuate line: no posterior rectus sheath - only transversalis fascia posteriorly, creating a structurally weaker zone
B. Suture Technique Errors - The Most Controllable Factor
- When suture bites incorporate fat and muscle alongside fascia, these non-fascial tissues become ischaemic and necrotic under suture tension
- This creates suture slack as the tissues compress and cut through, separating fascial edges (Fischer's Mastery of Surgery)
- The subsequent fascial gap forms the incisional hernia
- Prevention: The small bite technique (Israelsson) - 5 mm fascial bites, 5 mm apart, incorporating only aponeurotic tissue with a suture:wound length ratio ≥4:1 - is the current evidence-based standard (STITCH trial)
- A ratio <4:1 places excessive tension at each bite, causing ischaemia and failure
- Evidence shows intentionally achieving SL:WL >4 significantly reduces postoperative SSI, wound dehiscence, and incisional hernia
- Rapidly absorbable sutures (e.g., plain catgut, Vicryl) lose tensile strength before the fascia achieves adequate healing strength (~8 weeks)
- Fascial strength only reaches ~50% of its original strength by 2 months; full healing takes >1 year
- Braided/multifilament sutures: cause more tissue drag, harbour bacteria (increased SSI), and may cut through fascia more readily than monofilament
- Best practice: Slowly absorbable monofilament suture (e.g., PDS, Monocryl, Maxon) using a 2-0/0 gauge with a 30-40 mm needle
- Rapidly absorbable sutures should never be used for fascial closure
- Forcibly approximating ischaemic wound edges under tension causes tissue necrosis, suture cutting through, and eventual dehiscence
- Closure under undue tension impairs local blood supply to fascial edges
- Separate peritoneal closure adds no structural benefit and can cause adhesions
- Mass closure of all layers (including muscle) creates a mixture of tissue types under the suture - incorporating poorly healing tissues alongside strong fascia
C. Operative Setting and Duration
- Emergency laparotomy (vs. elective) is a strong independent predictor of incisional hernia
- No preoperative optimisation possible
- Often contaminated fields → higher SSI risk
- Frequently involves bowel-related procedures (contamination, stomas)
- Physiologically stressed patient with impaired healing
- Higher bacterial load → increased SSI risk → higher hernia rate
- Mesh placement is restricted, limiting repair options if hernia develops
- Longer operations associate with greater tissue oedema, blood loss, and drying
- Increased SSI risk with longer operations
- Tissue hypoperfusion and haematoma formation impair healing
- Haematoma is a nidus for wound infection
- Abdominal wound dehiscence (burst abdomen) almost inevitably leads to an incisional hernia if managed conservatively or re-closed under suboptimal conditions
- Port sites ≥10 mm that are not closed at fascial level have significantly higher hernia risk
- Trocar-site hernias are most common at the umbilicus (where all layers converge)
- Enlargement of port sites for specimen extraction greatly increases risk
D. Type of Operation
- Aortic aneurysm repair: very high hernia rates (up to 30-40%) due to underlying collagen disease
- Colorectal surgery / stoma formation and reversal: wound contamination; stoma site hernias
- Liver/pancreas surgery: prolonged ileus raises intra-abdominal pressure; nutritional depletion
- Renal transplantation (PMID 37715026): immunosuppression + surgical wound at iliac fossa
- Obesity surgery: wound complications in obese patients
III. POSTOPERATIVE FACTORS
- SSI is an independent predictor of early incisional hernia formation (<6 months postoperatively) (Fischer's Mastery of Surgery)
- Bacterial enzymes and inflammatory proteases (MMPs, collagenases) degrade newly forming collagen at the wound
- The wound gap from infected/separated wound tissue becomes a hernia
- Wound class, patient immune status, suture material (monofilament vs. braided), and operative technique all influence SSI risk
- Partial or complete fascial disruption postoperatively - if the burst abdomen is managed with re-closure or conservative treatment, incisional hernia is the rule
- Large seromas in the dead space above closed fascia create pressure on healing wound
- Seroma infection → SSI → hernia
- Wound haematoma → infection → impaired healing → hernia
- Prolonged ileus raises intra-abdominal pressure during the critical early wound-healing period, stressing the fresh repair
- Acute episodic raises in intra-abdominal pressure can disrupt early wound closure
- Particularly in COPD, chest infections, and smokers
- Repeated spikes in intra-abdominal pressure
IV. SUMMARY TABLE
| Category | Factor | Mechanism |
|---|---|---|
| Patient | Obesity | ↑ IAP, poor tissue perfusion, technical difficulty |
| Patient | Diabetes | Impaired collagen synthesis, ↑ SSI risk |
| Patient | Smoking | Vasoconstriction, ↑ MMPs, ↓ collagen synthesis |
| Patient | Malnutrition | Inadequate collagen substrate |
| Patient | Steroids/immunosuppression | Impairs all phases of wound healing |
| Patient | Collagen disorders | Reduced type I:III ratio; elevated MMP-2 |
| Patient | COPD/chronic cough | Repeatedly elevated IAP |
| Patient | Advanced age | Reduced collagen quality and healing capacity |
| Patient | Previous surgery/radiation | Scarred, poorly vascularised tissue |
| Operative | Midline incision | Poor blood supply; widest zone of linea alba |
| Operative | Large bite suture | Ischaemia of incorporated fat/muscle → suture slack → fascial gap |
| Operative | Low SL:WL ratio (<4:1) | Excessive suture tension → necrosis |
| Operative | Rapidly absorbable suture | Loses strength before fascial healing is adequate |
| Operative | Emergency surgery | No optimisation; contamination; high IAP |
| Operative | Contaminated wound | SSI risk; mesh avoidance |
| Operative | Prolonged operation | Oedema, blood loss, SSI |
| Postoperative | SSI | Protease degradation of forming collagen |
| Postoperative | Wound dehiscence | Direct fascial defect |
| Postoperative | Seroma/haematoma | Infection risk; dead space |
| Postoperative | Ileus/distension | Elevated IAP on fresh closure |
V. KEY PREVENTIVE IMPLICATIONS
- Suture technique: Small bites (5 × 5 mm), monofilament slowly-absorbable suture, SL:WL ratio ≥4:1 (STITCH trial)
- SSI prevention: Skin preparation, prophylactic antibiotics, antibiotic-coated sutures, NPWT in contaminated wounds
- Preoperative optimisation: Smoking cessation, glycaemic control (HbA1c <8), nutritional support, weight reduction
- Incision choice: Transverse/oblique incisions where feasible; minimal port-site enlargement laparoscopically; fascial closure of all ≥10 mm laparoscopic ports
- Prophylactic mesh augmentation (PMA): For very high-risk patients (AAA repair, BMI >35, COPD) - increasing evidence supports prophylactic retromuscular or onlay mesh at time of elective midline laparotomy
- Fischer's Mastery of Surgery, 8th Ed., Chapter 213 (Abdominal Wall Closure), pp. 5841-5852; Chapter 216 (Ventral Hernia), pp. 5897-5898
- Sabiston Textbook of Surgery, 21st Ed., Chapter 80 - Introduction and Anatomy, p. 1647-1648
- Schwartz's Principles of Surgery, 11th Ed., Chapter 35 - Surgical Anatomy and Wound Complications
- Amro et al. Genetic and biologic risk factors - Am J Surg 2024 (PMID 38519402) - reduced type I:III collagen ratio and elevated MMP-2 in hernia formation
- Tansawet et al. Prediction models SR/MA - World J Surg 2022 (PMID 36102959) - BMI, smoking, emergency operation, SSI consistently in multiple predictive models (pooled C-stat 0.81)
Discuss the methods used for abdominal wall repair
methods abdominal wall repair ventral hernia open laparoscopic robotic mesh techniques 2024 2025
ventral hernia repair laparoscopic open retromuscular mesh comparison outcomes
Methods Used for Abdominal Wall Repair
- Primary (suture) repair
- Mesh-based repair (open and minimally invasive)
- Component separation techniques
- Minimally invasive and robotic approaches
- Biological and biosynthetic mesh strategies for contaminated fields
- Prophylactic mesh augmentation
I. MESH PLANES - THE FOUNDATION OF MODERN REPAIR
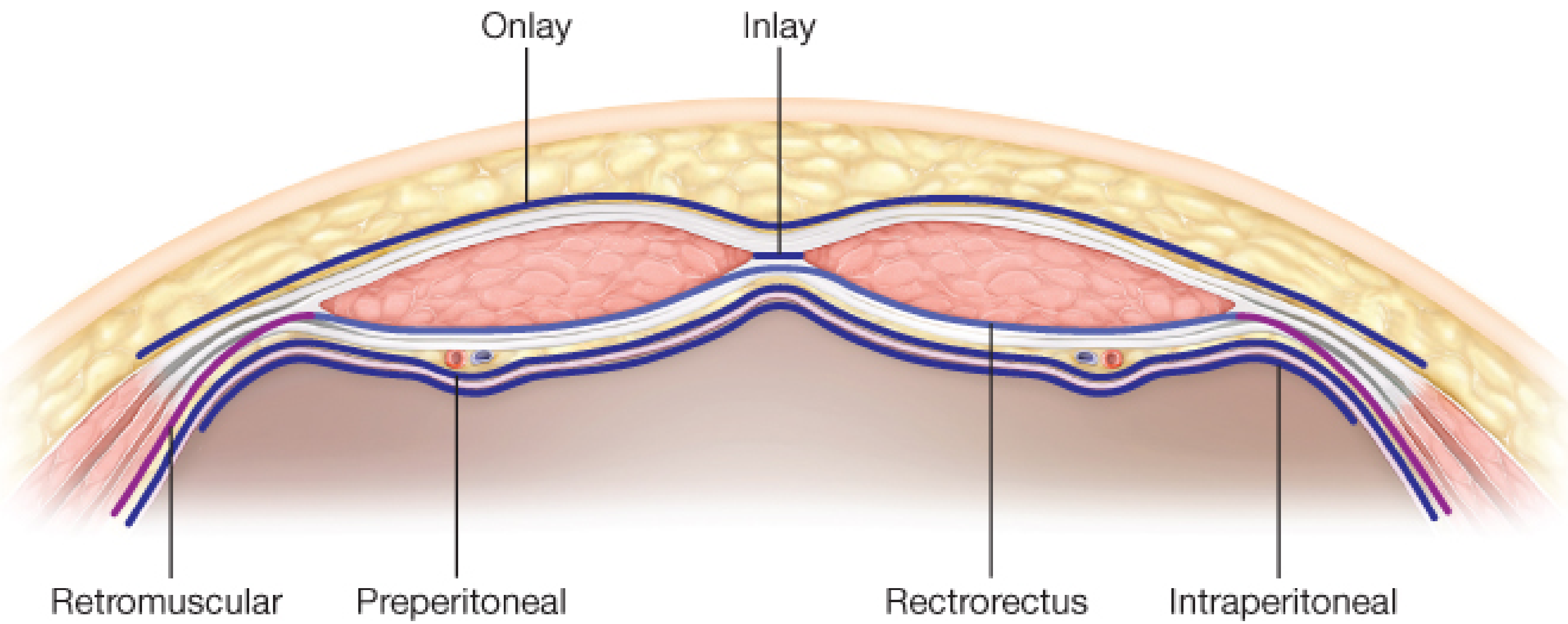
| ICAP Plane | Location | Synonyms |
|---|---|---|
| Onlay | Anterior to anterior rectus sheath | Supraaponeurotic |
| Inlay | Within defect as bridge | Bridging, interposition |
| Sublay - Retrorectus | Posterior to rectus, anterior to posterior sheath | Rives-Stoppa plane |
| Sublay - Retromuscular | Posterior to TA muscle, anterior to transversalis fascia | TAR space |
| Sublay - Preperitoneal | Between transversalis fascia and peritoneum | Preperitoneal |
| Intraperitoneal | Inside the peritoneal cavity | IPOM |
II. PRIMARY (SUTURE) REPAIR
A. Indications
- Small defects (<2 cm in most primary hernias; <4 cm in umbilical hernias per EHS guidelines)
- Contaminated or emergency settings where mesh is inadvisable
- Healthy fascia with tension-free approximation possible
B. Historical Techniques
- Described for umbilical hernias
- Fascial edges overlapped horizontally in an imbrication technique - two layers of interrupted sutures create fascial redundancy (one layer overlapping the other like "pants over vest")
- High recurrence rates for hernias >2 cm; largely historical
- The inverted hernia sac itself was used to create posterior redundancy; anterior rectus sheath relaxing incisions reduce tension
- Largely abandoned
- Used historically with reportedly good results; abandoned due to technical difficulty, wire fatigue, and complications (sinus formation)
C. Modern Primary Repair - The Small Bite Technique (Evidence-Based)
- Used for small hernias (<2 cm) and fascial closure at time of laparotomy
- STITCH trial principle: 5 mm fascial bites × 5 mm spacing, incorporating only the aponeurotic layer - no fat or muscle
- Suture:wound length (SL:WL) ratio ≥ 4:1
- Slowly absorbable monofilament suture (PDS 2-0, Monocryl) using 30-40 mm needle
- The running suture technique is preferred for even tension distribution
III. OPEN MESH-BASED REPAIR
A. Onlay Repair
- Skin flaps developed between skin/subcutaneous fat and anterior rectus sheath, extending laterally to the linea semilunaris
- Hernia sac reduced; fascia closed with running slowly absorbable suture
- Mesh secured with non-absorbable interrupted circumferential sutures to the fascia (not subcutaneous tissue)
- Drains placed on top of mesh; skin closed over
- Technically straightforward
- No entry into peritoneal cavity
- No intra-abdominal adhesions
- Large subcutaneous skin flaps required → high seroma rates, skin necrosis, wound breakdown
- Mesh in subcutaneous position vulnerable to SSI
- Higher recurrence rates than retromuscular/sublay position
B. Retrorectus (Rives-Stoppa-Wantz) Repair - The Current Open Gold Standard
- Midline incision; hernia sac entered, adhesiolysis performed to free anterior abdominal wall
- Posterior rectus sheath incised 2-3 mm lateral to its medial insertion on the linea alba (on both sides)
- Retrorectus space developed bilaterally by blunt and sharp dissection up to the linea semilunaris
- Neurovascular bundles (T7-L1) piercing the posterior sheath at the linea semilunaris are identified and protected
- Deep inferior epigastric vessels on the dorsal rectus protected
- Bilateral retrorectus spaces joined superiorly by dividing posterior sheath just lateral to linea alba cephalad (connecting the spaces through the preperitoneal fat below the xiphoid)
- Inferiorly, below the arcuate line, the spaces naturally communicate; Space of Retzius accessed down to pubic tubercle and Cooper's ligaments - allowing simultaneous groin hernia treatment
- Posterior sheath closed with 2-0 resorbable suture (creating a new "posterior wall")
- Large uncoated synthetic mesh (minimum 10-15 cm width) placed flat in the retrorectus space with at least 5 cm overlap beyond defect margins in all directions
- Mesh fixation optional (intra-abdominal pressure holds mesh); sutures or fibrin glue used if desired
- Anterior fascia closed over the mesh with small-bite technique
- Natural avascular space - no skin flaps
- Mesh completely extraperitoneal - no anti-adhesion coating required
- Large mesh overlap achievable
- Intra-abdominal pressure holds mesh in place
- Low SSI and recurrence rates (4-10%)
- Can address simultaneous groin hernias via Space of Retzius
C. Inlay (Bridging) Repair
IV. COMPONENT SEPARATION TECHNIQUES
A. Anterior Component Separation (ACS) - External Oblique Release (EOR)
- Subcutaneous skin flaps elevated between skin/fat and anterior rectus sheath, extending to the linea semilunaris
- External oblique aponeurosis incised 2 cm lateral to the linea semilunaris along the entire length (from costal margin to inguinal ligament)
- EO muscle fibres divided in continuity
- Plane between EO and IO developed
- Posterior rectus sheath incised and opened along the linea alba edge - this provides additional medial mobility
- Bilateral release allows medialisation of 3-10 cm per side (variable)
- Perforator-sparing ACS: Periumbilical perforators (within 3 cm radius of umbilicus) are identified and preserved to maintain skin blood supply
- Mini-incision / Semilunar approach: Multiple small incisions along the semilunar line rather than large skin flaps
- Endoscopic/laparoscopic ACS: Balloon dissector tunnels in subcutaneous space; EO divided under laparoscopic vision - preserves skin perforators
B. Posterior Component Separation - Transversus Abdominis Release (TAR)
- Retrorectus space developed on both sides as per Rives-Stoppa
- Posterior rectus sheath released 2-3 mm from linea alba insertion, from subxiphoid to arcuate line
- At the linea semilunaris: posterior lamella of internal oblique divided first, then transversus abdominis muscle and/or aponeurosis divided - entering the space superficial to transversalis fascia and peritoneum
- Release carried from subxiphoid, curving medial to costal margin, staying medial to neurovascular bundles
- Extended past the arcuate line, disconnecting posterior rectus sheath from lateral attachments
- Transversalis fascia and peritoneum dissected from underside of TA muscle - past midaxillary line, above costal margin (exposing diaphragm cranially, myopectineal orifices caudally)
- Posterior flap advancement: up to 10+ cm medially per side
- Posterior flaps reapproximated in midline with running suture
- Large uncoated mesh (typically 25-35 cm × 15-20 cm) placed in the retromuscular space
- Anterior fascial layers closed with small-bite technique
- No skin flaps required → preserves all musculocutaneous perforators → lower wound complication rates
- Larger potential mesh overlap (wide retromuscular space extending past midaxillary line)
- Mesh in retromuscular position (best integration, lowest recurrence)
- Simultaneously addresses subcostal, subxiphoid, and groin hernias
- Can be performed minimally invasively (laparoscopic/robotic)
V. LAPAROSCOPIC APPROACHES
A. Laparoscopic IPOM (Intraperitoneal Onlay Mesh)
- 3-5 trocars placed away from hernia
- Adhesiolysis, hernia sac reduction
- Composite mesh (synthetic + anti-adhesion barrier layer facing viscera) introduced and positioned to overlap defect by ≥3-5 cm in all directions
- Mesh fixated with transfascial sutures and/or tacks (no-go zones: triangle of doom, triangle of pain)
- Defect NOT closed
- IPOM-plus vs. IPOM: recurrence OR 0.51 (p<0.01), seroma OR 0.48 (p<0.01), mesh bulging OR 0.08 (p<0.01)
- IPOM-plus is now the standard when IPOM is chosen
- Mesh contacts bowel even with anti-adhesion coating → adhesion formation, fistula, SBO risk
- Tack fixation risks chronic pain (nerve injury)
- Less ideal for large defects (limited to medium defects)
- International guidelines now recommend preperitoneal/retromuscular placement over IPOM where possible
B. Laparoscopic TAPP (Transabdominal Preperitoneal)
- Peritoneal cavity entered → peritoneum incised above defect
- Preperitoneal dissection performed; hernia sac reduced
- Mesh placed in preperitoneal space
- Peritoneum closed over mesh (suture or tacks)
- Advantage: familiar intraperitoneal view; bilateral hernias easily identified
- Limitation: must close peritoneum; adhesiolysis if prior surgery
C. Laparoscopic/Robotic eTEP (Enhanced-View Totally Extraperitoneal)
- Initial access lateral to the rectus sheath; preperitoneal balloon dissection
- Bilateral retrorectus spaces developed and connected
- Mesh placed retrorectus
- eTEP extended to include posterior component separation
- For larger defects requiring TAR via minimally invasive approach
- No intraperitoneal entry - no adhesiolysis needed, no anti-adhesion mesh
- Reduced post-operative ileus
- Excellent ergonomics with robotic platform
VI. ROBOTIC REPAIR - The Dominant Current Advance
Robotic TARM (Transabdominal Retromuscular)
- Transabdominal access; peritoneum dissected off posterior rectus sheath
- Bilateral retrorectus spaces developed robotically
- Mesh placed retromuscular; peritoneum closed
Robotic eTEP / eTEP-TAR
- Fully extraperitoneal retrorectus repair with or without TAR
- TAR performed robotically under magnified 3D vision with articulated instruments
Robotic TAR (rTAR)
| Outcome | rTAR | Open TAR | p |
|---|---|---|---|
| Overall complications | 9% | 24.6% | <0.01 |
| SSI | 2.5% | 7.8% | 0.01 |
| Length of stay | -3.9 days shorter | Reference | <0.05 |
| Operative time | Longer | Shorter | <0.001 |
| Fascial closure rate | 99% | 94.6% | NS |
VII. MESH TYPES IN ABDOMINAL WALL REPAIR
A. Permanent Synthetic Mesh
- Polypropylene (PP): Most widely used; macroporous (>1 mm); good tissue ingrowth; used in clean fields; available in lightweight, standard, heavyweight variants
- Polyester: Softer, more pliable; used for large retromuscular repairs
- PTFE/ePTFE (Gore-Tex): Non-porous; used intraperitoneally (minimal adhesions) but poor tissue ingrowth
- Composite mesh (PP + anti-adhesion coating - titanium oxide, PVDF, collagen, cellulose): Used for IPOM; anti-adhesion layer faces bowel
B. Biologic Mesh
- Derived from human or animal extracellular matrix (human acellular dermis - AlloDerm; porcine dermis - Strattice; bovine pericardium)
- Allows tissue remodelling and ingrowth; resists infection better than synthetic
- Indication: Contaminated fields (CDC class III-IV), infected wounds, immunocompromised patients
- Very expensive; recent evidence questions superiority over biosynthetic mesh
- ACS 2025 data: Time to recurrence - synthetic mesh 132 months; long-acting resorbable 166 months; biologic mesh 80 months
C. Biosynthetic / Slowly Absorbable Mesh
- Poly-4-hydroxybutyrate (Phasix), TIGR matrix, BioA
- Resorbs over 12-24 months; allows native tissue remodelling
- Middle ground between synthetic and biologic - used in contaminated cases at lower cost than biologic mesh
VIII. REPAIR IN CONTAMINATED FIELDS
- Primary suture only (if small defect, good tissue)
- Biologic mesh - in the retromuscular or onlay position
- Biosynthetic mesh (Phasix, TIGR) - increasingly preferred for cost-effectiveness
- Staged repair:
- Stage 1: Remove infected mesh/debride; temporary abdominal closure with biological mesh, absorbable mesh, or NPWT
- Stage 2: Definitive repair at 6-12 months in a clean field
IX. SUMMARY OF METHODS BY DEFECT SIZE
| Defect Size | Preferred Method |
|---|---|
| <2 cm (small) | Primary suture (small-bite technique) ± mesh in high-risk patients |
| 2-4 cm (small-medium) | Mesh repair: retrorectus (Rives-Stoppa) or laparoscopic IPOM-plus |
| 4-10 cm (medium) | Open retrorectus (Rives-Stoppa) or laparoscopic/robotic eTEP-RS |
| >10 cm (large) | TAR (open or robotic) + retromuscular mesh; consider BTA preoperatively |
| Loss of domain | Preoperative optimisation (BTA ± PPP); TAR + large mesh; staged approach |
| Contaminated field | Biologic or biosynthetic mesh; staged repair |
| Emergency/strangulated | Primary repair or absorbable bridging mesh; definitive staged repair |
X. OUTCOMES COMPARISON
| Method | Recurrence | SSO/SSI | Advantages | Disadvantages |
|---|---|---|---|---|
| Primary suture | 10-50% (size-dependent) | Low | No mesh | High recurrence for >2 cm |
| Onlay mesh | 10-20% | High (skin flaps) | Simple, no peritoneal entry | Wound complications, subcutaneous mesh |
| Retrorectus (Rives-Stoppa) | 4-10% | Moderate | Gold standard; best integration | Open only; limited to ~8-10 cm defects |
| Open ACS + mesh | 5-15% | High (wound complications) | Large defects | 50% SSO with skin flaps |
| Open TAR + mesh | 5-12% | Moderate (lower than ACS) | Best for large defects | Complex; long OR time |
| Laparoscopic IPOM-plus | 5-15% | Low | MIS; fast recovery | Mesh inside peritoneum; tack pain |
| Robotic eTEP/TAR | 4-10% | Low (SSI 2.5%) | MIS + retromuscular; shorter LOS | Very expensive; longer OR time |
- Sabiston Textbook of Surgery, 21st Ed., Chapter 80 (Ventral Hernia), pp. 1650-1658
- Fischer's Mastery of Surgery, 8th Ed., Chapter 216 (Ventral Incisional Hernia), pp. 5907-5926
- ICAP Classification, Hernia 2019
- Lima et al. Open vs robotic TAR - Surg Endosc 2024 (PMID 39528659)
- Huang et al. IPOM-plus SR/MA - Hernia 2024 (PMID 38319440)
- Demetrashvili et al. ACS vs TAR RCT - Updates Surg 2025 (PMID 40360803)
- ACS Press Release, June 2025 - Long-acting resorbable mesh: longest time to recurrence (166 months) vs synthetic (132 months) vs biologic (80 months)
Biological meshes.
biologic mesh hernia repair outcomes contaminated
biological mesh hernia repair types properties indications outcomes 2024 2025
PMID: 35044431
PMID: 39666204
PMID: 36623959
PMID: 40473948
Biological Meshes in Abdominal Wall Surgery
I. DEFINITION AND CONCEPT
- Act as a scaffold for host tissue ingrowth and vascularisation
- Undergo remodelling - gradual replacement by the patient's own organised collagen and connective tissue
- Resist infection better than synthetic mesh in contaminated fields
- Be biocompatible with minimal foreign body response
II. SOURCES AND CLASSIFICATION
A. By Tissue of Origin
| Source | Tissue | Commercial Examples |
|---|---|---|
| Human (Allograft) | Acellular dermal matrix | AlloDerm (Lifecell), AlloMax, FlexHD |
| Porcine (Xenograft) | Dermis | Strattice (Lifecell), Permacol (Medtronic), CollaMend |
| Porcine (Xenograft) | Small intestinal submucosa (SIS) | Surgisis (Cook Biotech) |
| Porcine (Xenograft) | Urinary bladder matrix | MatriStem |
| Bovine (Xenograft) | Pericardium | Tutomesh, Veritas |
| Bovine (Xenograft) | Dermis | SurgiMend, PeriGuard |
| Fetal bovine | Dermis | SurgiMend PRS |
B. By Cross-Linking Status - A Critical Processing Variable
| Property | Non-Cross-Linked | Cross-Linked |
|---|---|---|
| Tissue remodelling | More extensive; faster incorporation | Less remodelling; slower degradation |
| Strength | Less initial mechanical strength | Greater initial strength |
| Degradation | Faster; risk of premature failure | Slower; more durable long term |
| Host cell infiltration | Better | Reduced |
| Infection resistance | Better (pores allow macrophage access) | Reduced (barrier to immune cells) |
| Examples | AlloDerm, AlloMax, Surgisis, SurgiMend | Permacol (glutaraldehyde cross-linked), CollaMend |
C. By Sterilisation Method
- Gamma irradiation: Most common; can affect collagen structure
- Ethylene oxide gas: Used for some products
- Non-sterilised / aseptic processing: Some allografts rely on aseptic technique rather than terminal sterilisation (e.g., AlloDerm in some configurations)
III. COMPOSITION AND STRUCTURE
- Type I and III collagen - primary structural proteins; ratio is important (type I is stronger)
- Elastin - provides elasticity and compliance
- Fibronectin and laminin - cell adhesion molecules promoting fibroblast attachment and migration
- Proteoglycans - regulate water content and cellular behaviour
- Growth factors (some products) - TGF-β, FGF, VEGF - promote vascularisation and remodelling
- Basement membrane components - critical for endothelial cell attachment and neovascularisation
IV. MECHANISM OF INCORPORATION
- Inflammatory phase (Days 1-7): Neutrophils and macrophages infiltrate; early debridement of necrotic material; Type M1 macrophage response
- Vascularisation (Days 3-14): Endothelial cell infiltration; neovascularisation of the scaffold; critical for graft survival
- Fibroblast infiltration (Days 7-21): Fibroblasts migrate along the collagen scaffold; begin synthesising new collagen
- Remodelling (Weeks to months): Host collagen replaces the original scaffold; scaffold gradually degraded and replaced by organised native tissue; ideally results in functional neo-fascia
V. INDICATIONS FOR BIOLOGICAL MESH
Primary Indication: Contaminated Fields
- Repair of hernia with concurrent bowel resection - enterotomy, stoma takedown, or bowel resection simultaneously
- Infected mesh explantation - removal of previously placed infected synthetic mesh with immediate repair
- Enteroatmospheric fistula - after open abdomen with bowel exposed; closure with biological mesh
- Strangulated hernia with bowel resection - contaminated field from necrotic bowel
- Active or recent wound infection at hernia site
- Open abdomen / damage control laparotomy - as temporary or definitive coverage
Secondary Indications (Selected Cases)
- High-risk patients with multiple risk factors where synthetic mesh infection would be catastrophic (transplant patients on heavy immunosuppression)
- Parastomal hernia repair where proximity to stoma makes infection likely
- Hiatal hernia reinforcement - level I RCT (Oelschlager) showed reduced recurrence (9% vs. 24%) with biologic mesh for paraesophageal hernia reinforcement; though follow-up studies reported significant mesh complications (erosion, stricture)
- Pelvic floor reconstruction in contaminated settings
Previously Claimed Indications Now Questioned
- Primary ventral hernia in clean fields - not recommended (high recurrence, no advantage over synthetic)
- Routine use in clean-contaminated (CDC Class II) wounds - increasingly replaced by synthetic or biosynthetic mesh
VI. SPECIFIC PRODUCTS AND THEIR PROPERTIES
A. AlloDerm (LifeCell) - Human Acellular Dermal Matrix
- Source: Human cadaveric dermis
- Cross-linking: Non-cross-linked
- Processing: Proprietary MatrACELL process; retains basement membrane
- Format: Available as single-layer and multi-layer (AlloDerm RTU - ready to use; and AlloDerm MegaSheet for large repairs)
- Properties: Excellent cell infiltration; good vascularisation; early remodelling
- Weakness: Softer initially; risk of laxity; expensive (~$20,000+ per repair)
- Evidence: Widely used but high recurrence rates in large contaminated hernias; no longer superior to synthetic in RCTs
B. Strattice (LifeCell) - Porcine Acellular Dermal Matrix
- Source: Porcine dermis
- Cross-linking: Non-cross-linked (unlike Permacol)
- Properties: Thicker and stiffer than AlloDerm; good mechanical strength; better suited for large defects
- Use: Complex abdominal wall reconstruction in contaminated fields; prophylactic reinforcement
C. Permacol (Medtronic) - Porcine Acellular Dermal Matrix
- Source: Porcine dermis
- Cross-linking: Glutaraldehyde cross-linked - the key distinguishing feature
- Properties: Very stiff and durable; slow degradation; reduced cellular infiltration; behaves more like a permanent prosthesis
- Concern: Cross-linking reduces macrophage access → poorer infection resistance than non-cross-linked products; risk of forming persistent foreign body if not incorporated
D. SurgiMend (Integra) - Fetal/Neonatal Bovine Dermal Matrix
- Source: Fetal bovine dermis
- Cross-linking: Non-cross-linked
- Advantage: Fetal tissue has higher type III:I collagen ratio (more elastic); potentially better remodelling in dynamic areas (chest wall, hiatus)
E. Surgisis / COOK BioDesign (Cook Biotech) - Porcine SIS
- Source: Porcine small intestinal submucosa (SIS)
- Cross-linking: Non-cross-linked; multi-layered (8-layer product available)
- Properties: Thinner; excellent growth factor content; promotes neovascularisation; good for small defects; may not provide enough strength for large hernia repair
F. CollaMend (BD/Bard) - Porcine Acellular Dermal Matrix
- Cross-linked; similar to Permacol
VII. BIOSYNTHETIC MESH - THE EMERGING ALTERNATIVE
| Product | Material | Degradation time | Use |
|---|---|---|---|
| Phasix (BD) | Poly-4-hydroxybutyrate (P4HB) | 12-18 months | Contaminated fields; high-risk |
| GORE BIO-A | Polyglycolide-trimethylene carbonate | ~6 months | Contaminated repair |
| Vicryl mesh (Ethicon) | Polyglactin 910 | 2-3 months (rapidly absorbed) | Temporary bridge only |
| TIGR matrix | Lactide + glycolide + trimethylene carbonate | 3 years | Long-lasting resorbable reinforcement |
VIII. THE CURRENT EVIDENCE CRISIS FOR BIOLOGICAL MESH
Landmark RCT - JAMA Surgery 2022 (PMID 35044431)
| Outcome | Synthetic Mesh | Biologic Mesh | p-value |
|---|---|---|---|
| 2-year hernia recurrence | 5.6% | 20.5% | <0.001 |
| Surgical site occurrence (SSI/wound complication) | Similar | Similar | 0.58 (NS) |
| Median prosthetic cost | $105 | $21,539 | <0.001 |
| Median 30-day hospital direct cost | $17,289 | $44,936 | <0.001 |
SR/MA - Surgery 2023 (PMID 36623959)
- Biologic mesh: significantly more hernia recurrence (OR 2.75, 95% CI 1.76-4.31, p<0.00001)
- Biologic mesh: significantly more SSI (OR 1.53, 95% CI 1.02-2.29, p=0.04)
- Conclusion: "Current evidence supports macroporous, uncoated synthetic mesh as the implant of choice for elective open ventral hernia repair, and its use should be considered even in contaminated cases."
Meta-Analysis - Hernia 2024 (PMID 39666204)
- Synthetic mesh: significantly lower recurrence than biologic (p<0.0001) in RCT subgroup
- No difference in SSI rates (between groups overall)
- Synthetic mesh: shorter length of stay
- Conclusion: Synthetic mesh is safe and effective in contaminated fields; biosynthetic meshes need further cost-effectiveness investigation
Meta-Analysis - Surg Endosc 2025 (PMID 40473948)
- Biologic mesh: higher SSI risk vs. synthetic (p=0.03)
- Biologic mesh: higher recurrence (p<0.0001)
- No benefit for biologic in reoperation, mesh removal, seroma, or haematoma
- Conclusion: No evidence of superiority for biological meshes over synthetic in contaminated environments
ACS 2025 Comparative Longevity Data
- Time to recurrence: Long-acting resorbable (166.4 months) > Synthetic (132.1 months) > Biologic (80 months)
- Biologic mesh had the shortest projected time to recurrence of all three categories
IX. COMPLICATIONS OF BIOLOGICAL MESH
| Complication | Notes |
|---|---|
| High recurrence rate | 20-40% at 2-5 years in contaminated cases; driven by insufficient remodelling and mesh degradation before adequate host tissue formation |
| Seroma | Common; fluid accumulation around degrading scaffold |
| Mesh laxity / bulge | As the mesh degrades before complete replacement by host tissue; leads to functional failure without frank recurrence |
| Infection | Surprisingly not reliably lower than synthetic in recent RCTs; cross-linked meshes may be particularly susceptible |
| Mesh removal | When infected or failed; removal is simpler than synthetic mesh explantation |
| Fistula formation | Particularly hiatal repair; mesh erosion into oesophagus or stomach reported |
| Encapsulation (cross-linked) | Cross-linked mesh may not fully incorporate → persistent foreign body disc |
| High cost | $20,000-$50,000 per case vs. <$200 for synthetic; unsustainable if outcomes are not superior |
X. PRACTICAL DECISION-MAKING: WHEN TO USE BIOLOGICAL MESH
| Situation | Current Recommendation |
|---|---|
| Clean field (CDC Class I), elective repair | Synthetic mesh; no role for biologic |
| Clean-contaminated (CDC Class II), elective | Synthetic mesh preferred (retromuscular); biologic no longer first choice |
| Contaminated (CDC Class III) | Synthetic mesh or biosynthetic; biologic only if patient-specific factors strongly favour it |
| Dirty/infected (CDC Class IV) | Biosynthetic (Phasix) or primary repair as staged approach; OR biologic if concurrent infection requires mesh and patient cannot tolerate staged repair |
| Infected mesh explantation | Staged approach preferred; if single-stage needed, retromuscular synthetic or biologic acceptable |
| Transplant/heavy immunosuppression | Biologic remains an option; evidence limited |
| Hiatal hernia reinforcement | Biologic has level I evidence (Oelschlager RCT) for reducing recurrence; but long-term erosion risk limits enthusiasm |
XI. SUMMARY
- Higher recurrence rates with biologic vs. synthetic mesh
- No significant advantage in SSI, mesh removal, or reoperation rates
- Dramatically higher costs (100-200x more expensive)
- Biosynthetic meshes (Phasix, BIO-A) emerging as cost-effective middle ground
- Sabiston Textbook of Surgery, 21st Ed., Chapter 80, pp. 1066-1068 (Mesh Classification)
- Rosen et al. Biologic vs Synthetic RCT - JAMA Surg 2022 (PMID 35044431): Synthetic superior to biologic; 5.6% vs 20.5% recurrence; $105 vs $21,539 prosthetic cost
- Mazzola Poli de Figueiredo et al. SR/MA RCTs - Surgery 2023 (PMID 36623959): Biologic OR 2.75 more recurrence; OR 1.53 more SSI
- Frountzas et al. MA contaminated fields - Hernia 2024 (PMID 39666204): Synthetic lower recurrence and LOS in contaminated fields
- Carvalho et al. MA CDC II-IV - Surg Endosc 2025 (PMID 40473948): No evidence of superiority for biologic mesh in contaminated environments
- SAGES Wiki: Biologic Mesh - clinical overview