Lymphadenopathy detailed
Reading File
Finding Sources
Finding Sources
Searching PubMed
lymphadenopathy diagnosis management
Searching Images
lymphadenopathy lymph node anatomy regions
Reading File
Reading File
Reading File
Reading File
Reading File
Finding Sources
Reading File
Finding Sources
Loading Image
Loading Image
Loading Image
I now have comprehensive material to write a detailed, well-structured answer. Here it is:
Lymphadenopathy — Detailed Overview
1. Definition & Normal Node Parameters
Lymphadenopathy refers to enlargement of one or more lymph nodes beyond accepted normal dimensions. Lymph nodes are bean-shaped secondary lymphoid organs distributed along lymphatic vessels; they typically measure <1 cm in diameter and function to filter lymph and mount immune responses to antigens.
What is "normal"?
- Soft, flat submandibular nodes <1 cm — often palpable in healthy children and young adults
- Inguinal nodes up to 2 cm — may be normal in adults
- Any supraclavicular or scalene node enlargement is always abnormal
— Harrison's Principles of Internal Medicine 22E, p. 520
2. Pathophysiology of Node Enlargement
Lymph nodes consist of B and T lymphocytes, macrophages, and dendritic cells. Enlargement occurs via three principal mechanisms:
| Mechanism | Example |
|---|---|
| Reactive hyperplasia — proliferation of lymphoid elements in response to antigen | Viral URTIs, infectious mononucleosis |
| Neoplastic infiltration — replacement by malignant cells | Lymphoma, metastatic carcinoma |
| Infiltrative/storage — deposition of abnormal material | Gaucher's disease, amyloidosis |
Afferent lymphatics drain into the subcapsular sinus; efferent lymph exits at the hilum. The hilus is the anatomical point where blood vessels enter/leave. — Goldman-Cecil Medicine, p. 1771
3. Classification
By Distribution
| Type | Definition | Common Associations |
|---|---|---|
| Localized / Regional | Single anatomic area | Infection of draining region, metastatic cancer |
| Generalized | ≥3 non-contiguous node regions | EBV, CMV, HIV, SLE, leukemia, lymphoma |
By Duration
- Acute (<2 weeks)
- Subacute (2–6 weeks)
- Chronic (>6 weeks)
4. Etiology — Comprehensive Classification (Harrison's Table 70-1)
1. Infectious Diseases
Viral: EBV (infectious mononucleosis), CMV, HIV, viral hepatitis, herpes simplex, HHV-6, VZV, rubella, measles, adenovirus, herpesvirus-8
Bacterial: Streptococci, staphylococci, Bartonella henselae (cat-scratch disease), brucellosis, tularemia, plague, chancroid, tuberculosis, atypical mycobacteria, syphilis (primary & secondary), diphtheria, leprosy
Fungal: Histoplasmosis, coccidioidomycosis, paracoccidioidomycosis
Chlamydial: Lymphogranuloma venereum, trachoma
Parasitic: Toxoplasmosis, leishmaniasis, trypanosomiasis, filariasis
Rickettsial: Scrub typhus, rickettsialpox, Q fever
2. Immunologic / Autoimmune Diseases
- Rheumatoid arthritis, juvenile RA
- Mixed connective tissue disease
- Systemic lupus erythematosus (SLE)
- Dermatomyositis, Sjögren's syndrome
- Serum sickness
- Drug hypersensitivity: diphenylhydantoin, hydralazine, allopurinol, primidone, gold, carbamazepine
- Angioimmunoblastic lymphadenopathy
- Primary biliary cirrhosis, graft-vs-host disease
- Silicone-associated lymphadenopathy
- IgG4-related disease
- Immune reconstitution inflammatory syndrome (IRIS)
3. Malignant Diseases
- Hematologic: Hodgkin's disease, non-Hodgkin's lymphomas, acute/chronic lymphocytic leukemia, hairy cell leukemia, malignant histiocytosis, amyloidosis
- Metastatic: Carcinomas from breast, lung, GI tract, thyroid, melanoma, genitourinary cancers
4. Lipid Storage Diseases
Gaucher's, Niemann-Pick, Fabry, Tangier disease
5. Endocrine
Hyperthyroidism
6. Other
- Castleman's disease (giant lymph node hyperplasia)
- Sarcoidosis
- Dermatopathic lymphadenitis
- Kikuchi's disease (histiocytic necrotizing lymphadenitis)
- Rosai-Dorfman disease (sinus histiocytosis with massive lymphadenopathy)
- Kawasaki's disease (mucocutaneous lymph node syndrome)
- Histiocytosis X, Familial Mediterranean fever
- Congestive heart failure (passive congestion)
Key epidemiologic point: In primary care, >2/3 of patients with lymphadenopathy have nonspecific or viral causes. <1% have a malignancy. In referred patients, 84% had benign diagnoses; 16% had malignancy (lymphoma or metastatic adenocarcinoma). — Harrison's 22E
5. Clinical Assessment
History
Key points to elicit:
- Symptoms: Sore throat, cough, fever, night sweats, fatigue, weight loss, node pain
- Age: Children/young adults → mostly benign (viral URTIs, mono, toxoplasmosis); after age 50, malignancy incidence rises
- Exposures: Animal contact (cat-scratch disease), sexual history (STIs), travel (endemic mycoses, TB, leishmaniasis)
- Medications: Diphenylhydantoin and others can cause drug-induced lymphadenopathy
- Occupation, tobacco use (ENT exam essential in adults with cervical adenopathy + smoking)
Physical Examination
Node characteristics:
| Feature | Benign/Reactive | Malignant |
|---|---|---|
| Size | <1.0 cm² | >2.25 cm² (1.5×1.5 cm) — suspicious |
| Texture | Soft | Rubbery (lymphoma), hard (metastasis) |
| Tenderness | Usually tender (capsular stretch) | Often nontender |
| Mobility | Mobile | Fixed, matted (metastatic cancer) |
| Borders | Discrete | May be irregular or matted |
Lymphoma nodes tend to be large, discrete, symmetric, rubbery, firm, mobile, nontender. Metastatic nodes are often hard, nontender, fixed. — Harrison's 22E
Splenomegaly + lymphadenopathy → strongly suggests systemic illness: EBV mononucleosis, lymphoma, leukemia, SLE, sarcoidosis, toxoplasmosis, cat-scratch disease.
6. Regional Adenopathy — Anatomical Clues
| Region | Common Benign Causes | Malignant Causes |
|---|---|---|
| Occipital | Scalp infection | Melanoma |
| Preauricular | Conjunctival infections, cat-scratch | — |
| Cervical | URTIs, oral/dental lesions, EBV, viral | Head & neck cancer, breast, lung, thyroid |
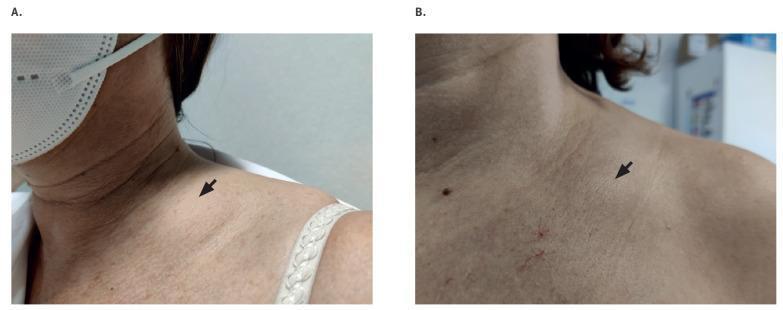
| Supraclavicular (always abnormal) | TB, sarcoidosis, toxoplasmosis | Lymphoma; lung/breast/testis/ovary cancers; Virchow's node (left supraclavicular) = GI primary |
| Axillary | Upper extremity infections/trauma | Melanoma, lymphoma, breast cancer |
| Inguinal | Lower extremity infections/trauma, STIs (LGV, syphilis, herpes, chancroid) | Lymphoma, rectal/genital/lower extremity (melanoma) cancer |
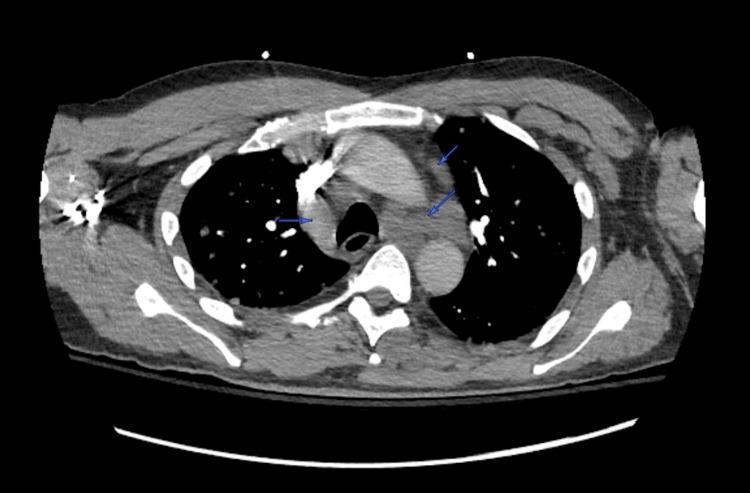
| Mediastinal | Sarcoidosis, histoplasmosis, TB | Lymphoma, lung/esophageal cancer |
| Abdominal/Retroperitoneal | TB | Lymphoma, metastatic disease |
7. Imaging Findings
CT Chest — Mediastinal Lymphadenopathy
CT Abdomen — Retroperitoneal Lymphadenopathy

Clinical Photo — Supraclavicular Lymphadenopathy
Sarcoidosis — Radiographic Pattern (Grainger & Allison)
- Bilateral symmetrical hilar and paratracheal lymphadenopathy in ~70–80% of sarcoidosis patients
- Occasionally asymmetrical; unilateral in only 1–5%
- Nodes can calcify, sometimes in eggshell pattern (shared by silicosis and histoplasmosis)
- Nodal enlargement maximal on first radiograph; usually resolves within 6–12 months
- "Icing sugar" calcification pattern characteristic
8. Diagnostic Workup
Laboratory Tests
Guided by clinical suspicion; initial panel typically includes:
- CBC with differential — atypical lymphocytes (EBV/CMV), leukocytosis (bacterial), blasts (leukemia), cytopenias (lymphoma/leukemia)
- ESR, CRP, LDH
- Monospot / EBV serology, CMV IgM
- Throat culture (if pharyngitis present)
- HIV testing (generalized adenopathy)
- PPD/IGRA (TB exposure risk)
- ANA, RF (if autoimmune suspected)
- Serum protein electrophoresis
- Chest X-ray — mediastinal adenopathy, pulmonary infiltrates
Imaging
- Ultrasound: First line for superficial nodes — identifies necrosis, guides biopsy; nodes with central necrosis warrant immediate surgical attention
- CT chest/abdomen/pelvis: Staging, detecting non-palpable adenopathy; CT identifies nodes in mediastinum, retroperitoneum, and iliac chains
- PET-CT: Preferred for lymphoma staging and treatment response
- MRI: Useful for delineating lymphatic channels (e.g., cystic hygroma, pelvic nodes)
9. Indications for Lymph Node Biopsy
Size thresholds:
- Nodes ≤1.0 cm² (1×1 cm) → almost always benign; observe with exclusion of mono/toxoplasmosis
- >2 cm diameter in younger patients (9–25 y) → predictor of malignant or granulomatous disease
- >2.25 cm² (1.5×1.5 cm) → best cutoff to distinguish malignant/granulomatous from benign
Other indications for biopsy:
- Supraclavicular location (always abnormal)
- Fixed, nontender, progressively enlarging node
- Constitutional symptoms: night sweats, unexplained weight loss, fever (B symptoms)
- Mediastinal adenopathy on imaging
- Failure to resolve after 4–6 weeks of observation (or antibiotic therapy when appropriate)
- Splenomegaly without obvious cause
Biopsy type:
- Excisional biopsy preferred for lymphoma (fresh specimen, not formalin — enables flow cytometry, immunophenotyping, cytogenetics)
- Core needle biopsy — acceptable for some solid malignancies
- Fine-needle aspiration (FNA) — useful for rapid cytology but insufficient for lymphoma diagnosis
10. Specific Conditions — Key Features
Infectious Mononucleosis (EBV)
- Generalized lymphadenopathy + pharyngitis + fever + splenomegaly
- Atypical lymphocytes on smear; positive monospot; EBV IgM
- Posterior cervical > anterior cervical involvement
Tuberculosis / Atypical Mycobacteria
- Cervical nodes most common (scrofula)
- Nontuberculous mycobacteria: fluctuant nodes, violaceous overlying skin, positive AFB cultures, tuberculin skin test positive; surgical excision often required (most NTM resistant to standard chemotherapy)
Cat-Scratch Disease (Bartonella henselae)
- Painful regional adenopathy, self-limited
- Cat exposure history (not always present)
- Diagnosis: indirect immunofluorescence antibody (moderate specificity) or PCR of biopsy
- Usually resolves without treatment
Lymphoma
- Hodgkin's: rubbery, discrete, symmetric nodes; mediastinal involvement common; Reed-Sternberg cells on biopsy
- Non-Hodgkin's: more variable distribution; systemic symptoms less predictable; excisional biopsy + flow cytometry required
Metastatic Cancer
- Hard, nontender, fixed nodes
- Location guides primary: neck (head/neck, thyroid); axilla (breast, melanoma); supraclavicular (lung, GI, testis, ovary); inguinal (genitourinary, melanoma, rectal)
- Virchow's node (left supraclavicular): Troisier's sign → GI primary (gastric cancer most classic)
Sarcoidosis
- Bilateral hilar lymphadenopathy ± paratracheal nodes ± parenchymal disease
- Granulomas on biopsy (non-caseating)
- ACE level elevated in ~60%; hypercalcemia possible
Kawasaki Disease
- Cervical lymphadenopathy + fever >5 days, conjunctival injection, rash, oral changes, extremity changes
- Children <5 years most commonly affected
- Risk of coronary artery aneurysms
Kikuchi's Disease (Histiocytic Necrotizing Lymphadenitis)
- Young women, self-limited
- Tender cervical adenopathy + fever
- Histology: necrotic foci with histiocytes, no neutrophils
11. Approach Algorithm
Lymphadenopathy detected
↓
Localized or Generalized?
↓
History + Physical Exam + CBC, ESR, monospot, CXR
↓
Obvious cause found (viral URTI, dental) → Treat and observe 4–6 weeks
↓ (no resolution or high-risk features)
Size ≥2 cm? Fixed? Supraclavicular? B symptoms? Constitutional symptoms?
↓ YES → Biopsy (excisional preferred)
↓ NO → Targeted workup (serology, TB testing, CT imaging)
Summary Table
| Feature | Benign/Reactive | Malignant |
|---|---|---|
| Age | Child / young adult | >50 years (higher risk) |
| Duration | <2 weeks | Weeks–months, progressive |
| Size | <1 cm | >2 cm |
| Texture | Soft, tender | Rubbery (lymphoma) or hard, fixed (mets) |
| Location | Cervical, inguinal | Supraclavicular always abnormal |
| Associated features | URTI, fever, pharyngitis | Night sweats, weight loss, fatigue |
| Resolution | Spontaneous within 4–6 weeks | Progressive |
Sources:
- Harrison's Principles of Internal Medicine 22E (2025) — Chapters 70 (Lymphadenopathy and Splenomegaly)
- Goldman-Cecil Medicine — Hematologic section
- Sabiston Textbook of Surgery — Neck masses, lymphadenopathy
- Grainger & Allison's Diagnostic Radiology — Sarcoidosis imaging
This is a shared conversation. Sign in to Orris to start your own chat.