1. Define erythropoiesis. Explain the stages of erythropoiesis. Detail about regulation of erythropoiesis. Add a note on Iron deficiency anemia.1. Define erythropoiesis. Explain the stages of erythropoiesis. Detail about regulation of erythropoiesis. Add a note on Iron deficiency anemia.1. Define erythropoiesis. Explain the stages of erythropoiesis. Detail about regulation of erythropoiesis. Add a note on Iron deficiency anemia.
Reading File
Finding Sources
Finding Sources
Reading File
Reading File
Reading File
Finding Sources
Reading File
Finding Sources
Finding Sources
Reading File
Finding Sources
Finding Sources
Reading File
Reading File
Finding Sources
Reading File
Reading File
Reading File
Finding Sources
Reading File
Loading Image
Loading Image
Reading File
Loading Image
Loading Image
I now have all the information needed for a comprehensive, well-illustrated answer. Let me compose it.
Erythropoiesis: Definition, Stages, Regulation, and Iron Deficiency Anemia
1. Definition of Erythropoiesis
Erythropoiesis is the process by which mature, circulating red blood cells (erythrocytes) are produced from hematopoietic stem cells in the red bone marrow. It is a continuous, demand-driven process that maintains the erythrocyte concentration in peripheral blood in a steady state. In adults, the body must replace approximately 200 billion red cells per day, each cell having a lifespan of about 120 days. Production is tightly regulated by the demands of oxygen delivery to the tissues.
- Histology: A Text and Atlas With Correlated Cell and Molecular Biology, p. 776
- Basic Medical Biochemistry - A Clinical Approach, 6e, p. 1536
2. Stages of Erythropoiesis
Erythropoiesis proceeds through two broad phases: a progenitor phase (morphologically unrecognizable, identified only by colony assays) and a precursor (normoblast) phase (morphologically recognizable under light microscopy).
A. Progenitor Phase (Bone Marrow - Morphologically Unrecognizable)
The pathway begins with the pluripotent hematopoietic stem cell (HSC) and progresses:
- HSC → committed to the myeloid lineage
- CFU-GEMM (Colony-Forming Unit - Granulocyte, Erythroid, Monocyte, Megakaryocyte) - a multipotent myeloid progenitor
- BFU-EMeg (Burst-Forming Unit - Erythroid/Megakaryocyte) - bipotent progenitor
- BFU-E (Burst-Forming Unit - Erythroid) - earliest erythroid-committed progenitor; responds weakly to EPO
- CFU-E (Colony-Forming Unit - Erythroid) - highly sensitive to erythropoietin; commits to erythroid differentiation
B. Precursor Phase (Morphologically Recognizable Normoblasts)
The first morphologically recognizable cell is the proerythroblast (pronormoblast). From here, each cell undergoes approximately 4 mitotic divisions, progressively decreasing in size while accumulating hemoglobin and condensing the nucleus, which is ultimately extruded.
| Stage | Key Features |
|---|---|
| 1. Proerythroblast | Largest precursor (~20 µm). Large nucleus with open chromatin and prominent nucleoli. Cytoplasm is deeply basophilic (many free ribosomes). No hemoglobin visible yet. Golgi appears as a pale perinuclear zone. |
| 2. Basophilic Erythroblast | Smaller than proerythroblast. Nucleus smaller; nucleoli disappear. Cytoplasm shows strong basophilia due to a massive increase in ribosomes actively synthesizing hemoglobin. Nuclear-to-cytoplasmic ratio decreased. |
| 3. Polychromatophilic Erythroblast | Intermediate stage. Cytoplasm shows a gray-blue color (polychromasia) - reflects a mixture of basophilic ribosomes and eosinophilic hemoglobin. Nucleus is smaller, chromatin increasingly condensed ("clock-face" clumping). Hemoglobin now detectable on staining. |
| 4. Orthochromatic (Acidophilic) Erythroblast | Small cell. Nucleus is tiny, pyknotic, and very densely staining. Cytoplasm is predominantly eosinophilic due to abundant hemoglobin. The last stage capable of division. The pyknotic nucleus is then extruded. |
| 5. Reticulocyte | Anucleate. Still contains residual ribosomes and mRNA, enabling continued hemoglobin synthesis. Slightly bluish on Romanowsky stain (polychromasia). Released from bone marrow into circulation. Matures over 1-2 days in the spleen, where ribosomes and mRNA are lost. Supravital stains (new methylene blue) reveal the ribosomal network. |
| 6. Mature Erythrocyte | Biconcave disc (~7.5 µm diameter). No nucleus, no ribosomes. Packed with hemoglobin. Lifespan: ~120 days. |
Key kinetics: Mitosis occurs in proerythroblasts, basophilic erythroblasts, and polychromatophilic erythroblasts. It takes approximately one week for the progeny of a newly formed basophilic erythroblast to reach the circulation. Bone marrow is not a significant storage site for erythrocytes; nearly all are released as soon as formed.
- Histology: A Text and Atlas, p. 776-777
- Junqueira's Basic Histology, 17e
3. Regulation of Erythropoiesis
Regulation operates at multiple levels: systemic (oxygen-sensing/EPO axis), nutritional (iron, B12, folate), and local (cytokines, feedback).
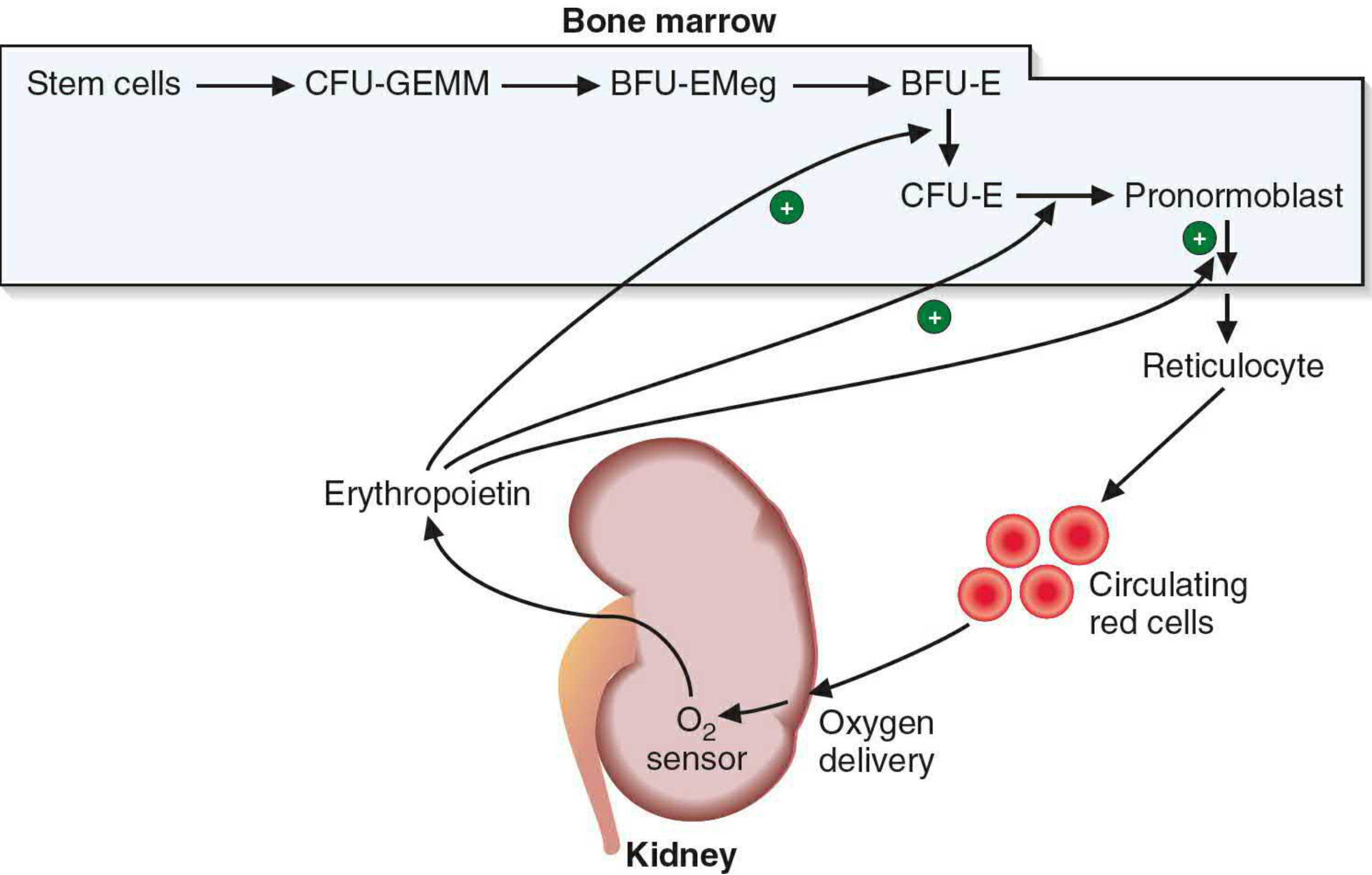
A. The Oxygen-Sensing / Erythropoietin Axis (Primary Regulator)
The fundamental stimulus for erythropoiesis is tissue hypoxia. Reduced oxygen delivery to the tissues triggers the following cascade:
- Hypoxia is sensed in the kidney (primarily by fibroblast-like peritubular interstitial cells in the cortex and outer medulla, and also by renal pericytes and epithelial cells).
- Under normoxia, the transcription factor HIF-1α (Hypoxia-Inducible Factor-1α) is continuously hydroxylated by prolyl hydroxylases, then ubiquitinated by the VHL complex and degraded.
- Under hypoxia, prolyl hydroxylases are inhibited → HIF-1α is stabilized → HIF-1α/HIF-2α (EPAS-1) dimerizes with HIF-1β → binds to the hypoxia response element (HRE) in the erythropoietin gene → EPO gene transcription is activated.
- Erythropoietin (EPO): A 34 kDa glycoprotein hormone. ~90% produced by the kidneys; ~10% by the liver. It is secreted into the bloodstream within minutes of hypoxic stimulus, reaching peak production within 24 hours.
- EPO acts on specific receptors on erythroid progenitors (BFU-E and especially CFU-E), activating JAK2/STAT5 signaling, which promotes:
- Proliferation of erythroid progenitors
- Differentiation into proerythroblasts
- Survival (inhibition of apoptosis)
- Accelerated maturation through the normoblast stages
- New RBCs appear in circulation approximately 5 days after EPO stimulus begins.
- As more RBCs are produced and oxygen delivery improves, the hypoxic stimulus decreases and EPO production falls - a negative feedback loop.
- When both kidneys are removed or destroyed, only ~10% of normal EPO (from the liver) is produced, causing severe anemia - demonstrating the kidney's indispensability.
Additional stimulators of EPO production: norepinephrine, epinephrine, and certain prostaglandins. Guyton and Hall Textbook of Medical Physiology, p. 443-444
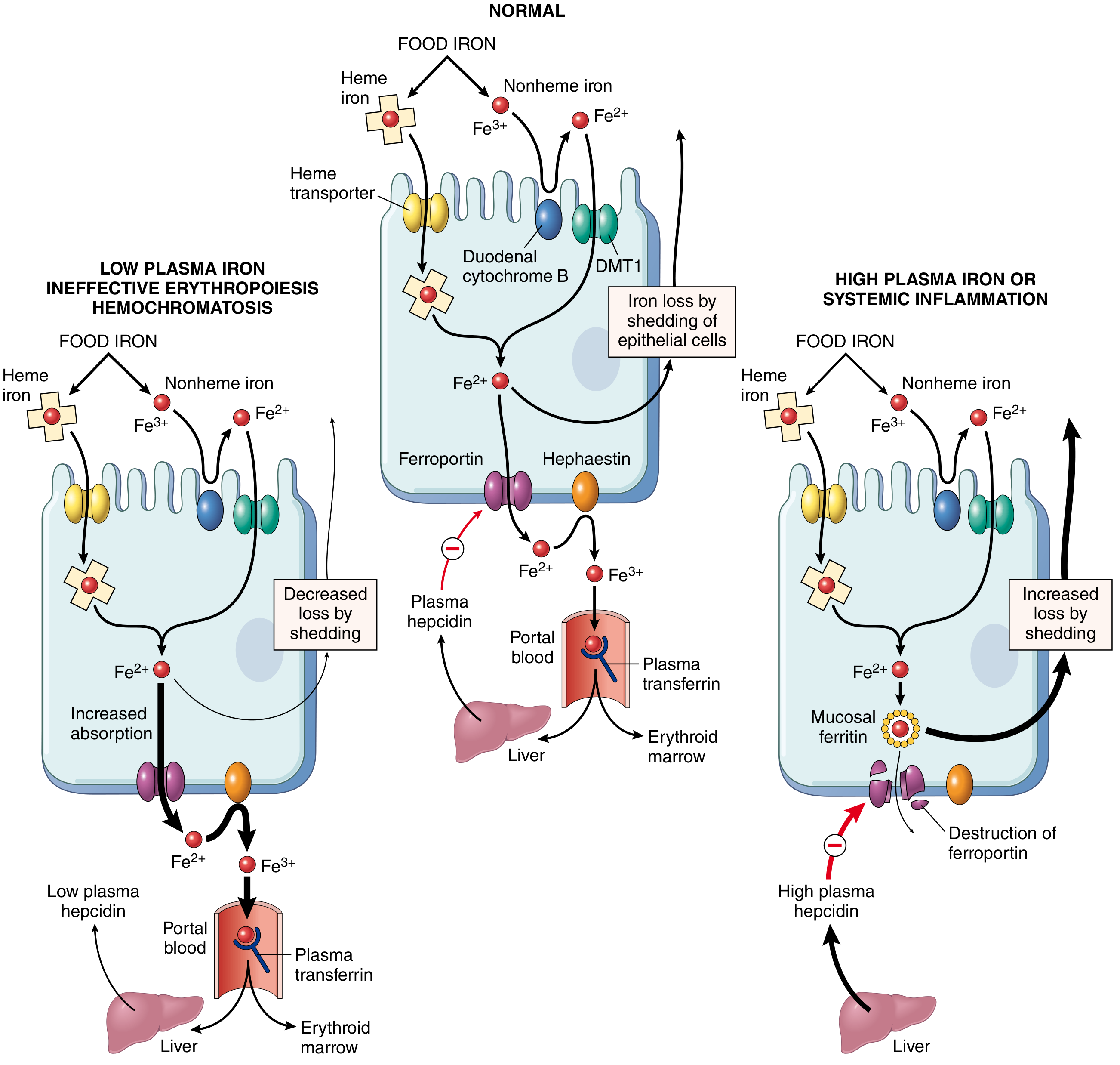
B. Role of Iron
Iron is indispensable for heme synthesis (protoporphyrin + Fe²⁺ = heme). Iron metabolism is tightly controlled:
- Absorption: In the proximal duodenum. Dietary heme iron (~20% absorbed) > nonheme iron (~1-2% absorbed). Fe³⁺ is reduced to Fe²⁺ by duodenal cytochrome B (ferrireductase) → transported into enterocytes via DMT1 (Divalent Metal Transporter 1) → exported to plasma via ferroportin → oxidized to Fe³⁺ by hephaestin/ceruloplasmin → bound to transferrin.
- Transport: Transferrin (synthesized in liver) carries iron to erythroid precursors via receptor-mediated endocytosis (transferrin receptor, TfR1). Transferrin is normally ~one-third saturated; serum iron averages 120 µg/dL (males) and 100 µg/dL (females).
- Storage: As ferritin (soluble, in hepatocytes and macrophages) and hemosiderin (insoluble aggregates, Prussian blue stain positive). Normal serum ferritin: 12-300 µg/L.
- Hepcidin - The Master Iron Regulator: A peptide hormone synthesized by the liver. Hepcidin binds ferroportin → ferroportin is internalized and degraded → iron is trapped within enterocytes and macrophages → less iron enters plasma. When iron stores are replete or inflammation is present (via IL-6), hepcidin rises. When iron is low, hepcidin falls, increasing absorption. This is the central mechanism linking systemic iron status to absorption.
C. Role of Vitamin B12 and Folate
Both are essential for DNA synthesis (specifically thymidine triphosphate formation). Deficiency leads to impaired cell division → erythroblasts fail to divide normally but continue to grow → large, dysplastic cells called macrocytes → megaloblastic anemia (macrocytic, hypersegmented neutrophils on smear). B12 requires intrinsic factor (secreted by gastric parietal cells) for absorption in the terminal ileum. Folate is absorbed in the proximal small intestine.
D. Role of Cytokines and Growth Factors
| Factor | Source | Role |
|---|---|---|
| Erythropoietin (EPO) | Kidney (90%), Liver (10%) | Primary: drives CFU-E to proerythroblast, promotes survival and differentiation |
| SCF (Stem Cell Factor) | Marrow stroma | Supports early erythroid progenitors |
| IL-3 | T lymphocytes | Stimulates BFU-E proliferation |
| GM-CSF | T cells, macrophages | Supports early myeloid and erythroid progenitors |
| Androgens | Adrenal glands, gonads | Stimulate EPO production (explains higher RBC count in males) |
| Thyroid hormones | Thyroid gland | Support basal erythropoiesis |
E. Feedback Regulation
- Positive feedback: Hypoxia → ↑ EPO → ↑ RBC production → ↑ O₂ delivery
- Negative feedback: ↑ O₂ delivery → ↓ EPO production → ↓ RBC production
- The rate of RBC production can rise to 10 or more times normal when large quantities of EPO are produced and sufficient nutrients are available (e.g., at high altitude).
4. Note on Iron Deficiency Anemia (IDA)
Definition
Iron deficiency anemia is the most common nutritional disorder worldwide, resulting from depletion of iron stores severe enough to impair hemoglobin synthesis, producing a hypochromic microcytic anemia.
- Robbins, Cotran & Kumar Pathologic Basis of Disease, p. 612
Epidemiology
Particularly affects toddlers, adolescent girls, females of childbearing age, and individuals in low-resource countries. In high-resource countries, chronic blood loss (especially gastrointestinal) is the dominant cause in adults.
Causes (4 main categories)
- Dietary deficiency: Inadequate intake - risk groups include infants (breast milk contains only ~0.3 mg/L iron), the impoverished, older adults, and vegans (lack of heme iron).
- Impaired absorption: Celiac disease (sprue), gastrectomy (reduces acidity and transit time through duodenum), Helicobacter pylori infection, achlorhydria.
- Increased demand: Infancy, adolescence, pregnancy, lactation.
- Chronic blood loss (most common cause in developed countries): GI bleeding (peptic ulcer, colorectal cancer, hookworm), menorrhagia, urinary tract bleeding. Iron deficiency in an adult male or postmenopausal female must be attributed to GI bleeding until proven otherwise - to avoid missing an occult cancer.
Pathogenesis (Sequential Stages of Depletion)
Stage 1 - Pre-latent (Iron depletion):
- Iron stores (ferritin, hemosiderin) depleted
- Serum ferritin falls
- No anemia; Hb, serum iron, and transferrin saturation still normal
Stage 2 - Latent (Iron-deficient erythropoiesis):
- Serum iron falls; TIBC (total iron binding capacity) rises
- Transferrin saturation falls (<15%)
- Erythroid hyperplasia in bone marrow (increased erythroid activity)
- No frank anemia yet
Stage 3 - IDA (Frank anemia):
- Iron stores completely exhausted
- Hemoglobin and hematocrit fall
- Hypochromic microcytic anemia appears
Morphology (Blood Smear and Bone Marrow)
- Peripheral blood smear: Microcytic (MCV <80 fL) and hypochromic red cells (central pallor >1/3 cell diameter, hemoglobin seen only as a narrow peripheral rim). Poikilocytosis - characteristic "pencil cells" (small, elongated red cells).
- Bone marrow: Mild to moderate increase in erythroid progenitors. Absence of stainable iron in macrophages on Prussian blue stain - the most diagnostically significant finding.

Laboratory Findings
| Parameter | IDA | Normal |
|---|---|---|
| Serum iron | ↓ (<60 µg/dL) | 60-170 µg/dL |
| Serum ferritin | ↓ (<12 µg/L) | 12-300 µg/L |
| TIBC (Total Iron-Binding Capacity) | ↑ (>400 µg/dL) | 250-400 µg/dL |
| Transferrin saturation | ↓ (<15%) | 20-45% |
| MCV | ↓ (<80 fL) | 80-100 fL |
| MCHC | ↓ | Normal |
| Reticulocyte count | ↓ (inappropriately low) | Normal |
| Serum hepcidin | ↓ | Normal |
| Bone marrow iron stores (Prussian blue) | Absent | Present |
Clinical Features
- General: Fatigue, pallor, weakness, dyspnea on exertion, palpitations (features of anemia)
- Iron-specific features (in severe/long-standing IDA):
- Koilonychia (spoon-shaped nails)
- Alopecia
- Atrophic glossitis (smooth, painful tongue)
- Angular cheilitis (cracking at corners of mouth)
- Pica (craving for non-food substances - clay, ice [pagophagia], flour)
- Plummer-Vinson syndrome (rare triad): esophageal webs + microcytic hypochromic anemia + atrophic glossitis
- Gastric mucosal atrophy → intestinal malabsorption (a vicious cycle)
- Central nervous system effects: irritability, poor concentration (especially in children)
Treatment
- Identify and treat the underlying cause (most important - exclude occult GI malignancy in adults).
- Oral iron supplementation: Ferrous sulfate (first choice) - 150-200 mg elemental iron/day in divided doses. Take on an empty stomach with vitamin C (enhances absorption). Response: reticulocytosis within 5-7 days → steady rise in hemoglobin → normalization of red cell indices over weeks.
- Parenteral iron: For those who cannot tolerate oral iron or have severe malabsorption.
- Dietary advice: Increase heme iron intake; avoid tea/coffee with meals (inhibit iron absorption).
Sources
- Robbins, Cotran & Kumar: Pathologic Basis of Disease, pp. 612-615
- Basic Medical Biochemistry - A Clinical Approach, 6e, p. 1536
- Guyton and Hall Textbook of Medical Physiology, pp. 443-444
- Histology: A Text and Atlas With Correlated Cell and Molecular Biology, pp. 746, 776-777
This is a shared conversation. Sign in to Orris to start your own chat.