
Screenshot_20260619-203246.png
Explain ovarian cancer
Reading File
Finding Sources
Finding Sources
Finding Sources
Finding Sources
Reading File
Reading File
Reading File
Reading File
Finding Sources
Reading File
Finding Sources
Finding Sources
Reading File
Reading File
Reading File
Searching PubMed
ovarian cancer classification pathogenesis treatment
Reading File
Loading Image
Loading Image
I now have comprehensive information to provide a thorough answer covering all the learning objectives (PA 29.4). Here is the full structured explanation:
Ovarian Tumors - Classification, Etiology, Pathogenesis, Pathology, Morphology, Clinical Course, Spread & Complications
1. Overview & Epidemiology
Ovarian cancer is the sixth most common malignancy in women, behind breast, lung, colorectal, uterine cancer, and melanoma. Over 90% of cancers arise from the surface epithelium of the ovary (which shares embryological origins with the peritoneum). The peak incidence is at ages 56-70 years. Most cases (about 30% of all ovarian neoplasms) are malignant, but in premenopausal patients only ~7% of ovarian epithelial tumors are malignant. The overall 5-year survival is <50% because approximately two-thirds of women present with advanced disease.
- Bailey and Love's Short Practice of Surgery, p. 1613
- Berek & Novak's Gynecology, p. 2317
2. Classification of Ovarian Tumors
Ovarian tumors are broadly classified by cell of origin into three main groups, with a fourth category for metastatic tumors:
A. Epithelial Tumors (~90% of malignant ovarian tumors)
Each subtype can be benign, borderline (low malignant potential), or malignant:
| Histologic Type | Cellular Origin | Key Features |
|---|---|---|
| Serous (75-80% of epithelial cancers) | Endosalpingeal (fallopian tube) | Psammoma bodies, papillary pattern |
| Mucinous (8-10%) | Intestinal / endocervical | Large multilocular cysts, mucin-secreting epithelium |
| Endometrioid (10%) | Endometrial | Associated with endometriosis (15-20% co-exist with endometrial carcinoma) |
| Clear Cell (5%) | Mullerian | Hobnail cells, always high-grade; linked to DES exposure & endometriosis |
| Brenner (Transitional) | Transitional (Walthard rests) | Mostly benign; rare malignant form |
| Mixed Epithelial | Mixed | - |
| Undifferentiated | Anaplastic | Worst prognosis |
- Berek & Novak's Gynecology, Table 39-1, p. 2304
B. Germ Cell Tumors (~20% in young women)
Arise from primordial germ cells. More common in children and young women (<21 years - two-thirds of ovarian malignancies in this group are germ cell tumors). Types include:
- Teratoma (mature/dermoid = benign; immature = malignant)
- Dysgerminoma (most common malignant germ cell tumor)
- Endodermal sinus (yolk sac) tumor - secretes AFP
- Choriocarcinoma - secretes hCG
- Embryonal carcinoma
C. Sex Cord-Stromal Tumors
- Granulosa cell tumor - most common, secretes estrogen (feminizing effects, endometrial hyperplasia/cancer risk)
- Theca cell tumor (Thecoma)
- Sertoli-Leydig cell tumor - secretes androgens (virilization)
- Fibroma - associated with Meigs' syndrome (fibroma + ascites + pleural effusion)
D. Metastatic Tumors (to ovary)
- Krukenberg tumor - bilateral metastasis typically from gastric carcinoma (signet ring cells)
- Also from breast, colorectal, endometrial primaries
3. Etiology & Risk Factors
Genetic / Hereditary Risk
- BRCA1 mutation: 39% lifetime risk of ovarian cancer up to age 70
- BRCA2 mutation: 11-17% lifetime risk up to age 70
- Lynch syndrome (mismatch repair gene mutations): 9-12% increased lifetime risk (in addition to endometrial cancer risk)
- Referral to specialist cancer genetics services is recommended for these high-risk patients
Hormonal / Reproductive Factors
- Increased risk: nulliparity, early menarche, late menopause, infertility, hormone replacement therapy
- Decreased risk: oral contraceptive use, multiple pregnancies, breastfeeding, tubal ligation - all reduce ovulatory cycles
Environmental
- Talc/asbestos exposure (disputed)
- High-fat diet, industrialized societies
The "Incessant Ovulation" Hypothesis
Each ovulation causes minor trauma to the ovarian surface epithelium; repeated cycles of trauma and repair increase the chance of oncogenic mutation.
- Bailey and Love's Short Practice of Surgery, p. 1615
4. Pathogenesis
A key conceptual shift has occurred in recent decades:
Most serous carcinomas do NOT originate from the ovarian surface epithelium - they originate from the fimbrial end of the fallopian tube. Evidence comes from examination of risk-reducing salpingo-oophorectomy specimens from BRCA patients. Clear cell and endometrioid subtypes are derived from endometriosis.
Type I vs. Type II Serous Carcinoma (molecular classification)
| Feature | Type I (Low-grade serous) | Type II (High-grade serous) |
|---|---|---|
| Growth | Slow | Rapid, aggressive |
| Genetics | Stable; KRAS or BRAF mutations; no p53 mutations | Unstable; p53 mutations (almost universal) |
| Origin | Borderline serous tumors | Fimbrial precursor lesions (STIC) |
| Stage at diagnosis | Often early | Usually advanced |
| Behavior | Good prognosis | Poor prognosis |
Neoplastic transformation occurs when cells are genetically predisposed and/or exposed to an oncogenic agent.
- Berek & Novak's Gynecology, p. 2303-2305
5. Morphology & Histopathology
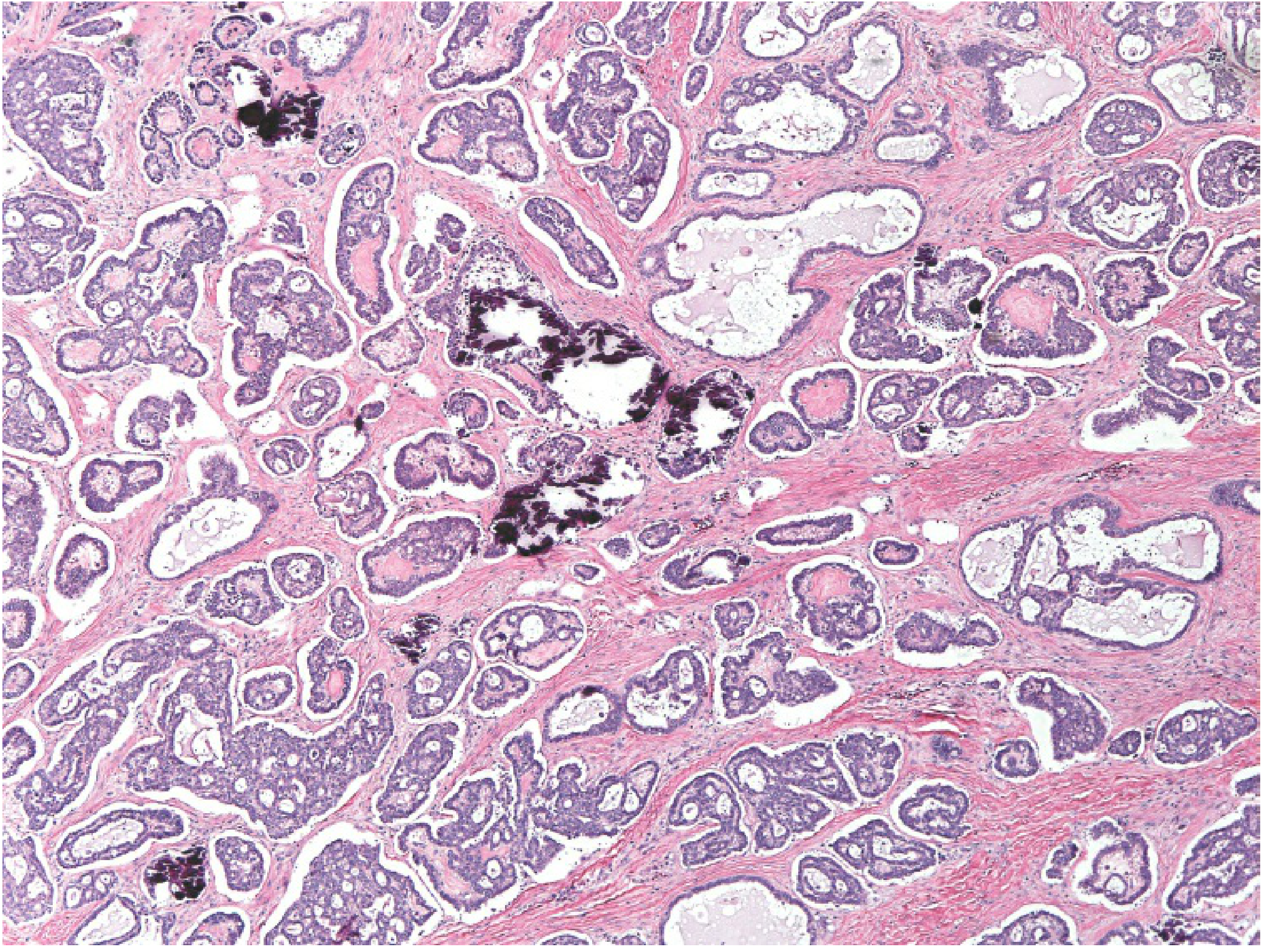
Serous Tumors (most common)
Psammoma bodies (concentric laminated calcifications) are characteristic. Show papillary structures lined by cuboidal to columnar cells.
Mucinous Tumors
Loculi lined by mucin-secreting epithelium resembling intestinal or endocervical cells. May reach enormous size filling the abdominal cavity. Bilateral in only 8-10%. Can cause pseudomyxoma peritonei (gelatinous mucoid material throughout the peritoneal cavity).
Endometrioid Carcinoma
Complex glandular pattern resembling proliferative endometrium. Co-exists with endometrial carcinoma in 15-20% of cases. This combination may represent synchronous primary tumors (better prognosis: 75-80% 5-year survival) vs. metastatic disease (30-40% 5-year survival).
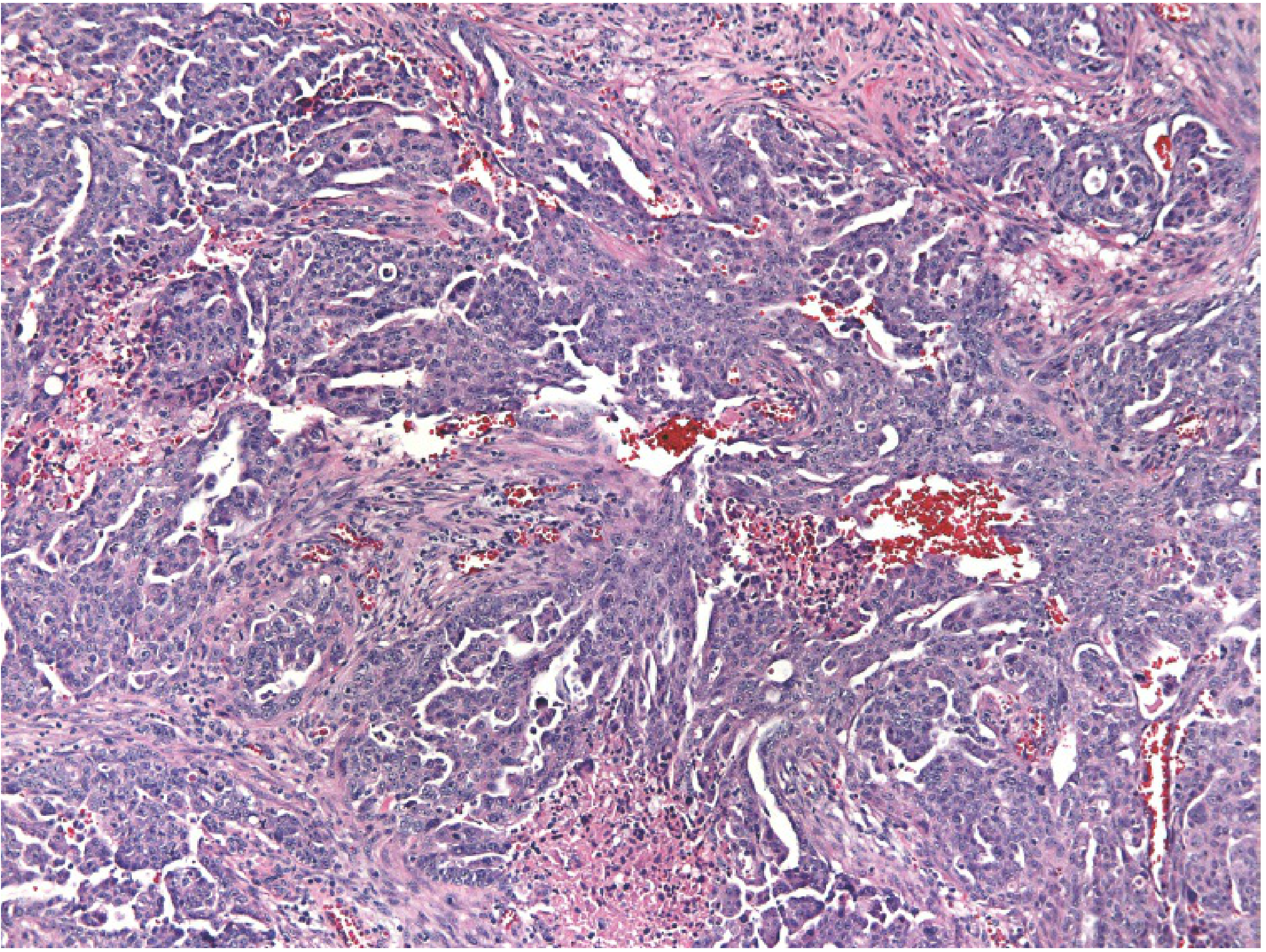
Clear Cell Carcinoma
Tubulocystic, papillary, reticular, or solid patterns. Cells have clear or vacuolated cytoplasm and hobnail cells (nuclei projecting into apical cytoplasm). Always high-grade - not graded separately.
Borderline (Low Malignant Potential) Tumors
-
No stromal invasion (key distinguishing feature from invasive carcinoma)
-
Occur predominantly in premenopausal women (peak age 30-50)
-
Very good prognosis; extraovarian implants can occur but are usually noninvasive
-
Berek & Novak's Gynecology, p. 2305-2315
6. Clinical Course & Presentation
Symptoms
Ovarian cancer is the "silent killer" because symptoms are often vague and non-specific:
- Abdominal distension and/or pain
- Change in appetite, early satiety
- Weight gain, increased girth (from ascites)
- Urinary symptoms (urgency/obstruction)
- Shortness of breath (pleural effusion)
- Gastrointestinal disturbance, change in bowel habit
Over half of women initially present to a specialty other than gynaecology with metastatic disease symptoms. A pelvic mass + ascites is the classic combination strongly suggesting ovarian cancer.
Rarely, paraneoplastic syndromes occur: disseminated intravascular coagulation (DIC), polyneuritis, dermatomyositis, hemolytic anemia, cerebellar degeneration.
Physical Signs
-
Solid, irregular, fixed pelvic mass = highly suspicious for malignancy
-
Upper abdominal mass with ascites = almost certain ovarian cancer
-
Bilateral adnexal masses are more likely malignant than unilateral
-
Berek & Novak's Gynecology, p. 2317-2329
7. Staging (FIGO)
| Stage | Description |
|---|---|
| I | Growth limited to the ovaries |
| II | Involvement of one or both ovaries with pelvic extension (uterus, bladder, sigmoid, rectum) |
| III | Peritoneal implants outside pelvis or retroperitoneal/inguinal lymph nodes |
| IV | Distant metastases (liver parenchyma, pleural effusion cytology positive) |
Approximately two-thirds of patients present at Stage III or IV.
- Bailey and Love's Short Practice of Surgery, Table 87.15, p. 1615
8. Routes of Spread
- Direct extension - to adjacent pelvic structures (uterus, fallopian tube, bladder, rectum)
- Peritoneal seeding (most common) - exfoliated cells implant throughout the peritoneal cavity; preferentially to the omentum (omental caking), paracolic gutters, diaphragm
- Lymphatic spread - pelvic and para-aortic lymph nodes
- Hematogenous spread - liver parenchyma, lung (late/rare)
- Transdiaphragmatic spread - to pleural cavity causing pleural effusion
9. Investigations & Tumor Markers
CA-125
- A glycoprotein expressed on coelomic and Mullerian-derived epithelia
- Normal cut-off: 35 U/mL
- Elevated in 50% of stage I and >90% of advanced disease
- Primarily detects epithelial ovarian cancers
- Non-specific: also elevated in endometriosis, PID, pregnancy, other cancers
- Very high CA-125 (>200 U/mL) in postmenopausal women with adnexal mass = 96% positive predictive value for malignancy
Imaging
- Transvaginal ultrasound - preferred; malignant features: irregular borders, multiple echogenic patterns, dense irregular septae, bilateral, >8 cm, ascites
- CT scan - staging, assessing peritoneal disease and lymph nodes
- Screening with CA-125 + TVU has not been proven to reduce mortality in average-risk women (USPSTF recommends against routine screening)
Other Markers
- AFP - Yolk sac tumor
- hCG - Choriocarcinoma, dysgerminoma
- LDH - Dysgerminoma
- Inhibin - Granulosa cell tumor
10. Treatment
Surgery (Primary Cytoreduction)
- Total abdominal hysterectomy + bilateral salpingo-oophorectomy (TAH + BSO)
- Infracolic omentectomy
- Pelvic and para-aortic lymph node sampling
- Peritoneal washings (diaphragm, right and left abdomen, pelvis)
- Appendicectomy for mucinous tumors
- Biopsies of all suspicious peritoneal surfaces
Goal: reduce residual tumor to <1 cm (optimal cytoreduction)
Fertility-sparing surgery (unilateral oophorectomy) is an option only for young women with stage IA/IB disease or borderline tumors.
Chemotherapy
- First-line: Carboplatin + Paclitaxel (IV or intraperitoneal)
- BRCA-mutated: PARP inhibitors (olaparib, niraparib) as maintenance therapy
- Bevacizumab (anti-VEGF) as add-on for advanced disease
Prophylactic Risk Reduction
- Prophylactic bilateral salpingo-oophorectomy (PBSO) recommended for BRCA carriers after childbearing is complete; reduces but does not eliminate risk (2-3% residual peritoneal carcinoma risk remains)
11. Complications
| Complication | Notes |
|---|---|
| Ascites | From peritoneal seeding and lymphatic obstruction |
| Intestinal obstruction | From peritoneal implants and adhesions (leading cause of death) |
| Pleural effusion | Transdiaphragmatic spread or lymphatic obstruction |
| Ureteric obstruction | From pelvic mass |
| Paraneoplastic syndromes | DIC, cerebellar degeneration, dermatomyositis |
| Malnutrition/cachexia | Advanced disease |
| Deep vein thrombosis/PE | Hypercoagulable state associated with malignancy |
| Pseudomyxoma peritonei | From mucinous tumors; gelatinous mucoid material fills peritoneal cavity |
Summary Points for Exam
- 90% of malignant ovarian tumors are epithelial (most: serous type)
- Most high-grade serous carcinomas originate from the fallopian tube fimbria, NOT the ovary
- Type I (low-grade, KRAS/BRAF mutations) vs. Type II (high-grade, p53 mutations) is the key molecular distinction
- BRCA1 = 39% lifetime risk; BRCA2 = 11-17% lifetime risk
- Classic spread = peritoneal seeding (omentum, diaphragm, paracolic gutters)
- CA-125 >35 U/mL is the main marker; elevated in 50% Stage I, >90% advanced disease
- No effective screening in average-risk women
- Treatment: cytoreductive surgery + carboplatin/paclitaxel chemotherapy
- Borderline tumors = no stromal invasion, good prognosis, occur in younger women (30-50 yrs)
Sources: Berek & Novak's Gynecology, pp. 2303-2340; Bailey and Love's Short Practice of Surgery, 28th Ed., pp. 1613-1616
This is a shared conversation. Sign in to Orris to start your own chat.