Pap report of atypical glandular cell NOS
Reading File
Finding Sources
Finding Sources
Searching PubMed
"atypical glandular cells" cervical cytology management
Reading File
Reading File
Reading File
Finding Sources
Finding Sources
Loading Image
Reading File
Finding Sources
Reading File
Reading File
Here is a comprehensive summary of Atypical Glandular Cells (AGC) - NOS on a Pap smear report:
Pap Report: Atypical Glandular Cells (AGC) - NOS
What It Means
AGC-NOS is a Bethesda 2001 classification term used when glandular cells show atypia that exceeds normal reactive changes but falls short of adenocarcinoma in situ (AIS) or frank malignancy. "NOS" (Not Otherwise Specified) indicates the atypia cannot be further characterized as favoring neoplasia.
- Previously called AGCUS (atypical glandular cells of undetermined significance), the "US" was dropped in Bethesda 2001 because the incidence of significant pathology is too high to imply uncertainty
- These cells originate from endocervical or endometrial glandular epithelium (as opposed to squamous cells in ASC-US or HSIL)
- Pfenninger and Fowler's Procedures for Primary Care notes: "10% cancers and 25% high-grade lesions" are found in women with AGC - far higher than with ASC-US
Bethesda System AGC Classification
| Category | Risk of High-Grade Lesion/Carcinoma |
|---|---|
| AGC-NOS | 9% to 41% |
| AGC, favor neoplasia | 27% to 96% |
| AIS (adenocarcinoma in situ) | Very high |
Initial Workup (ASCCP Guidelines)
For all AGC subcategories EXCEPT atypical endometrial cells:
- Colposcopy with endocervical sampling (ECC)
- HPV DNA testing (high-risk/oncogenic types)
- Endometrial sampling - if the patient is:
- Age >35 years, OR
- Any age with unexplained vaginal bleeding or risk factors for endometrial neoplasia (e.g., chronic anovulation, obesity)
For atypical endometrial cells specifically:
- Endometrial AND endocervical sampling first
- If no endometrial pathology found: proceed to colposcopy
Key rule: Repeat cytology alone is NOT acceptable as initial management of AGC-NOS. Immediate colposcopy is mandatory.
Subsequent Management Flowchart
The ASCCP management algorithm for AGC-NOS after initial workup:
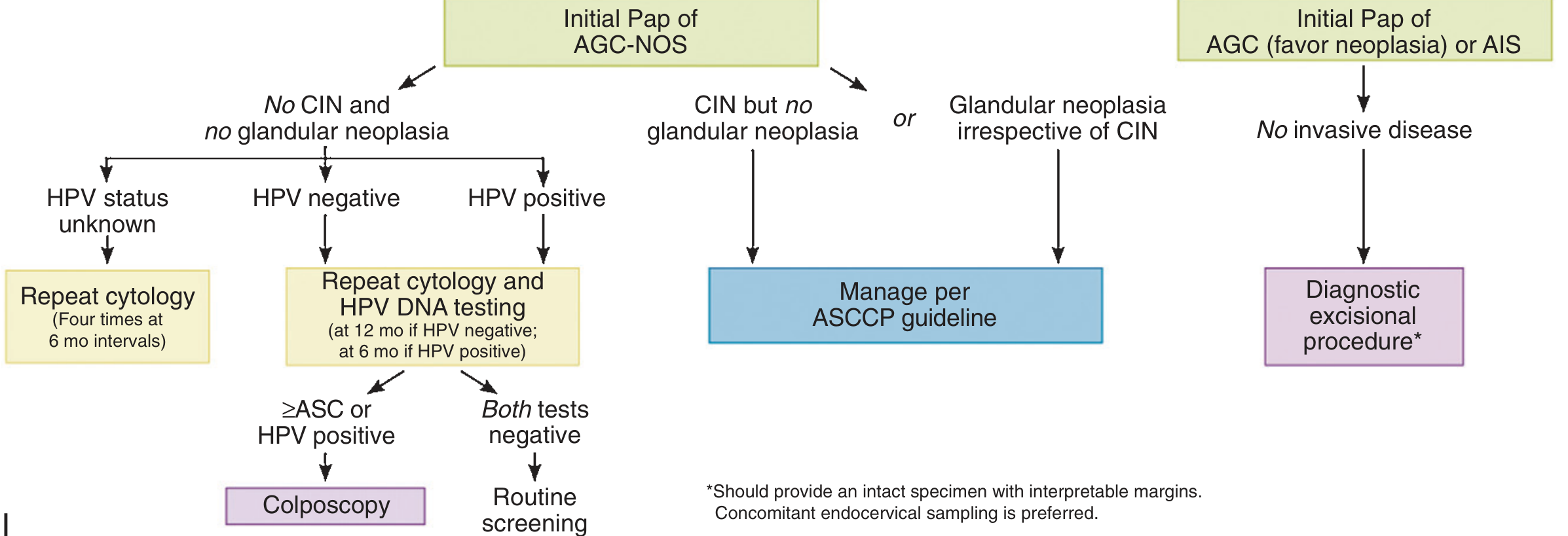
If initial workup shows NO CIN and NO glandular neoplasia:
- HPV status unknown: Repeat cytology x4 (every 6 months)
- HPV negative: Repeat co-testing (cytology + HPV DNA) at 12 months
- HPV positive: Repeat co-testing at 6 months
- If repeat shows ≥ASC or HPV positive: Colposcopy
- If both tests negative: Return to routine screening
If CIN is found but no glandular neoplasia:
- Manage per ASCCP guidelines for CIN
If glandular neoplasia is found (with or without CIN):
- Manage per ASCCP guidelines
If initial Pap was AGC "favor neoplasia" or AIS with no invasive disease:
- Diagnostic excisional procedure (LEEP/cold knife conization with intact specimen and interpretable margins; concomitant endocervical sampling preferred)
Special Populations
- Pregnancy: AGC in pregnancy is less likely to indicate malignancy compared to non-pregnant patients, but evaluation is limited because endocervical curettage (ECC) and endometrial sampling cannot be performed - Creasy & Resnik's Maternal-Fetal Medicine
- Immunocompromised patients (HIV, transplant): Require more aggressive follow-up; colposcopy is recommended whenever there is concern for severe or malignant changes
Why AGC-NOS is Taken Seriously
Unlike ASC-US (which often resolves), AGC carries substantial risk of underlying pathology that may be:
- High-grade cervical intraepithelial neoplasia (CIN 2/3)
- Endocervical adenocarcinoma or AIS
- Endometrial carcinoma
- Rarely: ovarian or fallopian tube cancer (5.4% ovarian cancers among malignancies found)
A systematic review of ~7,000 women with AGC on Pap found malignancy in 5.2% of patients overall - Berek & Novak's Gynecology.
Common Clinical Pitfall
Clinicians sometimes confuse AGC with ASC-US (atypical squamous cells) - these require different workup and the management algorithms are distinct. AGC always mandates immediate colposcopy; ASC-US may be triaged with reflex HPV testing first - Pfenninger and Fowler's Procedures for Primary Care, p. 1710.
Bottom line: AGC-NOS on Pap is a high-risk cytology finding requiring immediate workup (colposcopy + ECC + HPV testing ± endometrial biopsy based on age). It should never be dismissed or managed with repeat cytology alone.
This is a shared conversation. Sign in to Orris to start your own chat.