📚 Parasitology Syllabus • General Parasitology (Host, Parasite, Vector) • Protozoa (Amoeba, Naegleria flowleri, Giardia, Leishmania, Plasmodium, Toxoplasma, Trichomonas) • Helminths (Cestodes, Trematodes, Nematodes) • Important Parasitic Diseases (Ascariasis, Enterobiasis, Hookworm, Filariasis, Trichinellosis, Dracunculiasis, Chagas Disease) • Laboratory Diagnosis • Prevention & Control of Parasitic Infections
Reading File
Finding Sources
Finding Sources
Reading File
Reading File
Reading File
Reading File
Reading File
Reading File
I now have comprehensive content from the textbooks. I have enough rich material to write a thorough, well-structured parasitology study guide. Let me now compile the full notes.
📚 Complete Parasitology Notes
Sources: Quick Compendium of Clinical Pathology 5th ed., Medical Microbiology 9e (Murray), Sherris & Ryan's Medical Microbiology 8th ed., Jawetz Melnick & Adelberg's Medical Microbiology 28th ed.
PART 1 - GENERAL PARASITOLOGY
Key Definitions
| Term | Definition |
|---|---|
| Parasite | An organism that lives in or on another organism (host) and benefits at the host's expense |
| Host | The organism that harbors the parasite |
| Definitive host | Host in which the parasite undergoes sexual reproduction (e.g., humans for Taenia, mosquito for Plasmodium) |
| Intermediate host | Host in which asexual reproduction or larval development occurs |
| Reservoir host | A non-human host that harbors the parasite and serves as a source of human infection |
| Paratenic host | Carries the larval form without further development; acts as a "transport" host |
| Vector | An arthropod that transmits the parasite (biological or mechanical) |
| Zoonosis | Infection transmitted from animals to humans |
Types of Parasitism
- Ectoparasite - lives on the surface (e.g., lice, scabies)
- Endoparasite - lives inside the host (e.g., Plasmodium, Ascaris)
- Obligate parasite - cannot survive without a host
- Facultative parasite - can live free or parasitically (e.g., Naegleria)
Parasite Life Stages
- Trophozoite - active, feeding, motile form (vegetative)
- Cyst - dormant, infective, environmentally stable form
- Sporozoite - infective stage injected by mosquito
- Merozoite - released after hepatic schizogony; invades RBCs
- Gametocyte - sexual stage; ingested by vector
Types of Vectors
- Biological vector - parasite develops/multiplies inside (e.g., Anopheles mosquito for malaria, Aedes for filariasis)
- Mechanical vector - parasite is carried without development (e.g., fly carrying cysts)
PART 2 - PROTOZOA
Overview
Protozoa are unicellular eukaryotes. Classified by mode of motility:
- Sarcodina - move by pseudopodia (amoeba)
- Mastigophora - move by flagella (Giardia, Leishmania, Trichomonas)
- Ciliophora - move by cilia (Balantidium)
- Sporozoa/Apicomplexa - non-motile adults (Plasmodium, Toxoplasma, Cryptosporidium)
2.1 ENTAMOEBA HISTOLYTICA (Amoebiasis)
| Feature | Detail |
|---|---|
| Transmission | Fecal-oral; contaminated food/water |
| Infective stage | Cyst (4 nuclei) |
| Disease stage | Trophozoite (ingested RBCs = pathognomonic!) |
| Habitat | Large intestine |
| Disease | Amoebic dysentery, amoebic liver abscess |
Pathogenesis:
- Trophozoites invade colonic mucosa → flask-shaped ulcers
- Portal spread → liver abscess ("anchovy paste" / chocolate brown pus)
- Rarely: lung, brain abscess
Cyst morphology:
- 10-20 μm, 4 nuclei with central karyosome
- Chromatoid bars (cigar-shaped) with rounded ends
- Glycogen vacuoles
Trophozoite morphology:
- 15-60 μm, ingested RBCs visible inside
- Eccentric nucleus with central karyosome
Diagnosis:
- Stool O&P (3 specimens, ≥24 hrs apart)
- Serology (positive in invasive disease)
- Trichrome stain on stool
Treatment: Metronidazole + luminal agent (paromomycin or iodoquinol)
Non-pathogenic species to know: E. dispar, E. coli, E. hartmanni, Iodamoeba bütschlii, Endolimax nana
2.2 NAEGLERIA FOWLERI
| Feature | Detail |
|---|---|
| Classification | Free-living amoeba (thermophilic) |
| Habitat | Warm stagnant freshwater, soil |
| Entry | Nasal mucosa → cribriform plate → olfactory nerve → frontal lobe |
| Disease | Primary Amoebic Meningoencephalitis (PAM) |
| Population | Children/young adults swimming in warm freshwater |
| Prognosis | Nearly always fatal (>97% mortality) |
Key facts:
- No cysts found in brain tissue (unlike Acanthamoeba)
- Trophozoites: 10-35 μm, small nucleus with large dense central karyosome; can be mistaken for macrophages in CSF
- Culture: grown on agar with E. coli lawn
- CSF specimens must NOT be refrigerated before culture (organisms die in cold)
Diagnosis: Trophozoites in CSF; PCR; culture on E. coli
Treatment: Amphotericin B + azithromycin + rifampin (rarely successful)
Compare with other free-living amoeba:
| Feature | Naegleria | Acanthamoeba | Balamuthia |
|---|---|---|---|
| Disease | PAM | GAE + Keratitis | GAE |
| Host | Immunocompetent | Immunocompromised | Both |
| Cysts in brain? | No | Yes | Yes |
| Entry route | Nasal (cribriform) | Hematogenous | Hematogenous |
| Course | Acute (days) | Subacute/chronic | Subacute/chronic |
| Contact lens risk? | No | Yes (keratitis) | No |
Quick Compendium of Clinical Pathology 5th ed., p. 124
2.3 GIARDIA INTESTINALIS (syn. G. lamblia, G. duodenalis)
| Feature | Detail |
|---|---|
| Transmission | Fecal-oral, contaminated water ("beaver fever") |
| Infective stage | Cyst (4 nuclei) |
| Disease stage | Trophozoite |
| Habitat | Duodenum and jejunum (NOT colon) |
| Disease | Giardiasis - fatty diarrhea, malabsorption, bloating, flatulence |
Trophozoite morphology (classic):
- Pear/teardrop-shaped, bilaterally symmetrical
- 2 nuclei (gives "owl-eye" or "monkey face" appearance)
- 4 pairs of flagella
- Sucking disk (adhesive disk) - attaches to intestinal villi
- Ventral concavity
Cyst morphology:
- Oval, 8-12 μm, 4 nuclei
- Intracytoplasmic fibrils
Pathogenesis: Mechanical blockade of intestinal epithelium + villous flattening → malabsorption (fat-soluble vitamins A, D, E, K)
Diagnosis:
- Stool O&P (3 specimens - intermittent shedding)
- String test (Enterotest)
- Stool antigen ELISA / DFA - more sensitive
- Note: no peripheral eosinophilia (intestinal protozoa don't invade)
Treatment: Metronidazole or tinidazole; nitazoxanide
2.4 LEISHMANIA SPECIES
| Disease | Species | Vector | Geography |
|---|---|---|---|
| Visceral (Kala-azar) | L. donovani, L. infantum | Female Phlebotomus sandfly | Asia, Africa, Mediterranean |
| Cutaneous (Oriental sore) | L. major, L. tropica | Female Phlebotomus sandfly | Middle East, Africa |
| Mucocutaneous (Espundia) | L. braziliensis | Lutzomyia sandfly | South America |
Life cycle:
- Promastigote (flagellated) - in sandfly, infective stage
- Amastigote (no flagellum) - intracellular in macrophages/reticuloendothelial cells of human host
Visceral leishmaniasis (Kala-azar):
- "Kala-azar" = black sickness (Hindi)
- Massive hepatosplenomegaly, fever, weight loss, pancytopenia
- Hypergammaglobulinemia
- Amastigotes in macrophages of liver, spleen, bone marrow
Cutaneous: Painless papule → ulcer with raised indurated borders ("volcano crater")
Diagnosis:
- Giemsa-stained bone marrow/spleen aspirate (amastigotes within macrophages)
- Culture on NNN medium
- PCR, serology (rK39 antigen for visceral)
Treatment: Liposomal amphotericin B (drug of choice); pentavalent antimonials (sodium stibogluconate)
2.5 PLASMODIUM SPECIES (Malaria)
Five species infecting humans:
| Species | Fever Pattern | RBC Change | Key Features | Relapse? |
|---|---|---|---|---|
| P. falciparum | Quotidian → malignant tertian (36-48h) | Smaller, multiple rings, Maurer's clefts | Most dangerous; cerebral malaria; banana-shaped gametocytes | No (no hypnozoites) |
| P. vivax | Benign tertian (48h) | Enlarged, Schüffner's dots | Widest distribution; DARC receptor | Yes (hypnozoites) |
| P. ovale | Benign tertian (48h) | Enlarged, fimbriated/oval edges, Schüffner's dots | Africa, milder | Yes (hypnozoites) |
| P. malariae | Quartan (72h) | Smaller, band trophozoites | Causes nephrotic syndrome | No (but recrudescence) |
| P. knowlesi | Daily (24h = quotidian) | Normal/small | Zoonosis (macaques), SE Asia | No |
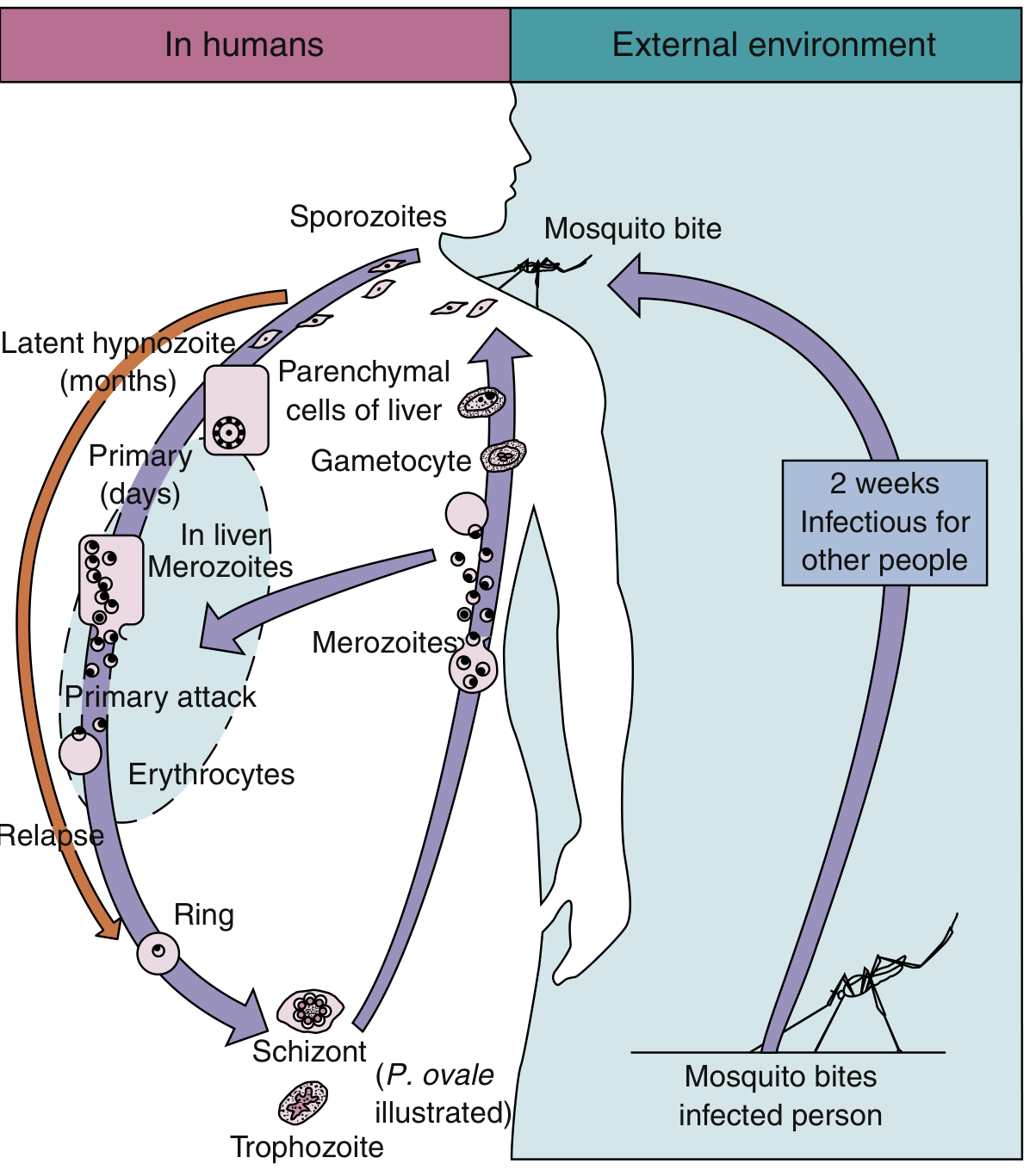
Life Cycle:
- Mosquito bite → sporozoites enter blood → liver (exoerythrocytic schizogony, 8-25 days)
- Hepatocytes rupture → merozoites released → enter RBCs
- Erythrocytic cycle: ring → trophozoite → schizont → rupture → merozoites (fever paroxysm at this point)
- Some merozoites → gametocytes (sexual stage)
- Anopheles mosquito ingests gametocytes → sporogony in mosquito → sporozoites in salivary glands
- P. vivax/ovale: some sporozoites become hypnozoites (dormant liver forms → relapse)
P. falciparum special features (most virulent):
- Cytoadherence (knobs on RBC surface) → capillary sludging → cerebral malaria
- Rosette formation
- No persistent liver stage (no relapse, only recrudescence)
- Infects all RBC ages; others are age-selective
- Banana/crescent-shaped gametocytes
Complications:
- Cerebral malaria (P. falciparum)
- Blackwater fever: massive hemolysis → hemoglobinuria → dark urine
- Nephrotic syndrome (P. malariae)
- Splenic rupture
- Severe anemia, thrombocytopenia
Diagnosis:
- Thick blood film (screening - concentration): Giemsa or Wright stain
- Thin blood film (speciation - morphology)
- Rapid diagnostic test (RDT) - antigen detection (HRP2 for P. falciparum)
- PCR (most sensitive/specific)
Treatment:
- Chloroquine-sensitive: chloroquine
- Chloroquine-resistant P. falciparum: artemisinin combination therapy (ACT)
- P. vivax/ovale relapse prevention: primaquine (G6PD screen first - risk of hemolysis)
- Severe malaria: IV artesunate (preferred) or IV quinine
Prevention: Mosquito nets, insect repellent (DEET), chemoprophylaxis (chloroquine, mefloquine, doxycycline, atovaquone-proguanil)
2.6 TOXOPLASMA GONDII
| Feature | Detail |
|---|---|
| Definitive host | Cats (only host for sexual cycle/oocysts in stool) |
| Intermediate host | Humans, most warm-blooded animals |
| Infective forms | Oocysts (in cat feces), tissue cysts (in undercooked meat), tachyzoites (congenital) |
| Transmission | Ingestion of oocysts (contaminated soil, cat litter), undercooked meat, congenital (transplacental), blood transfusion/organ transplant |
Forms:
- Tachyzoite - rapidly replicating, active infection, crescent/banana shaped (active disease)
- Bradyzoite - slowly replicating, in tissue cysts (latent infection, especially brain and muscle)
- Oocyst - sexual form shed in cat feces; environmentally resistant
Disease presentation:
| Population | Manifestation |
|---|---|
| Immunocompetent | Usually asymptomatic or mild mononucleosis-like (cervical lymphadenopathy) |
| AIDS/Immunocompromised | Toxoplasmic encephalitis (ring-enhancing lesions on MRI, basal ganglia) |
| Congenital | Triad: chorioretinitis, hydrocephalus, intracranial calcifications |
| Pregnant women | Can cause fetal death, spontaneous abortion |
Congenital toxoplasmosis - Classic Triad:
Chorioretinitis + Hydrocephalus + Intracranial calcifications (periventricular)
Diagnosis:
- Serology (IgM = acute; IgG = past/chronic)
- PCR of CSF or amniotic fluid
- Brain biopsy (ring-enhancing lesions)
- Neonatal IgM (does not cross placenta)
Treatment: Pyrimethamine + sulfadiazine + leucovorin (folinic acid to prevent myelosuppression)
- Prophylaxis in HIV: TMP-SMX (also prevents PCP)
2.7 TRICHOMONAS VAGINALIS
| Feature | Detail |
|---|---|
| Classification | Flagellated protozoan (mastigophora) |
| Transmission | Sexually transmitted (STI) - most common non-viral STI worldwide |
| Infective/disease stage | Trophozoite only (no cyst stage) |
| Habitat | Vagina/male urethra |
| Morphology | Pear-shaped, 4 anterior flagella + 1 recurrent flagellum (on undulating membrane), axostyle |
Clinical:
- Women: vaginitis, yellow-green frothy vaginal discharge, "strawberry cervix" (petechiae), pH >4.5
- Men: usually asymptomatic; urethritis possible
- Characteristic jerky, tumbling, non-directional motility on wet mount
Diagnosis:
- Wet mount (direct microscopy) - motile trophozoites; sensitivity ~60%
- Nucleic acid amplification test (NAAT) - most sensitive/specific
- Culture on Diamond's medium
- Pap smear can detect incidentally
Treatment: Metronidazole (2g single dose) - treat both partners; tinidazole is alternative
PART 3 - HELMINTHS
Helminths are multicellular worms. Divided into:
- Cestodes (tapeworms) - flat, segmented
- Trematodes (flukes) - flat, unsegmented
- Nematodes (roundworms) - cylindrical, unsegmented
General: Lab Finding - Eosinophilia
- Eosinophilia is the hallmark of tissue-invasive helminth infections
- Pure intestinal protozoa (Giardia, E. histolytica) do NOT cause eosinophilia
- Highest eosinophilia: Trichinella, visceral larva migrans, Strongyloides, early Ascaris migration
3.1 CESTODES (Tapeworms)
All tapeworms have:
- Scolex (head) - with suckers ± hooks for attachment
- Neck - region of growth
- Proglottids - body segments (immature → mature → gravid)
3.1.1 Taenia saginata (Beef Tapeworm)
- Transmission: ingestion of undercooked beef containing cysticerci
- Definitive host: humans; Intermediate host: cattle
- Scolex: 4 suckers, no hooks (unarmed)
- Proglottids: 15-30 uterine branches per side
- Does NOT cause cysticercosis in humans (eggs not infectious to humans)
- Treatment: praziquantel or niclosamide
3.1.2 Taenia solium (Pork Tapeworm)
- Transmission: ingestion of undercooked pork (cysticerci) → intestinal tapeworm; OR ingestion of eggs (fecal-oral) → cysticercosis
- Scolex: 4 suckers + hooks (armed/rostellum) - "armed tapeworm"
- Neurocysticercosis = most common cause of acquired epilepsy worldwide
- Cysts in brain (ring-enhancing lesions, calcifications on CT)
- Treatment: albendazole + steroids + antiepileptics
- Treatment of intestinal form: praziquantel or niclosamide
3.1.3 Echinococcus species (Hydatidosis / Cystic Echinococcosis)
- Definitive host: dogs; Intermediate hosts: sheep, cattle, humans (accidental)
- Transmission: ingestion of eggs from dog feces
- Disease: hydatid cysts in liver (70%), lungs (20%), rarely brain
- Cysts contain protoscoleces ("hydatid sand")
- Never aspirate/needle biopsy - risk of anaphylactic shock + dissemination
- Diagnosis: imaging (CT/US) + serology (IHA, ELISA)
- Treatment: PAIR (Puncture, Aspiration, Injection, Re-aspiration) + albendazole; surgical resection
3.1.4 Diphyllobothrium latum (Fish Tapeworm)
- Transmission: ingestion of raw/undercooked freshwater fish
- Intermediate hosts: copepods (1st) → freshwater fish (2nd)
- Largest tapeworm infecting humans (up to 10 meters)
- Vitamin B12 deficiency → megaloblastic anemia (tapeworm preferentially absorbs B12)
- Egg: oval with unshouldered operculum + abopercular knob
- Treatment: praziquantel
3.1.5 Hymenolepis nana (Dwarf Tapeworm)
- Smallest cestode infecting humans
- Unique: can complete entire life cycle in one host (autoinfection possible)
- Transmission: ingestion of infected beetles or person-to-person
- Treatment: praziquantel
3.2 TREMATODES (Flukes)
All trematodes (except Schistosoma) are hermaphroditic.
3.2.1 Schistosoma species (Blood Flukes)
- Unique: dioecious (separate sexes), the female lives in the groove of the male
- Vector: freshwater snails (Biomphalaria, Bulinus, Oncomelania)
- Transmission: cercariae penetrate intact skin while wading/swimming in freshwater
| Species | Site of Eggs | Disease |
|---|---|---|
| S. mansoni | Lateral spine, stool | Intestinal/hepatic schistosomiasis, periportal fibrosis |
| S. haematobium | Terminal spine, urine | Urogenital schistosomiasis, bladder cancer (SCC) |
| S. japonicum | Small lateral spine, stool | Most eggs per worm; severe hepatosplenomegaly |
Cercarial dermatitis ("swimmer's itch") = immediate hypersensitivity at entry site
Katayama fever = acute schistosomiasis - fever, urticaria, eosinophilia (Serum sickness-like)
Chronic: portal hypertension, "Symmer's clay pipe-stem fibrosis" (S. mansoni/japonicum)
Diagnosis: Eggs in stool/urine; Kato-Katz thick smear; serology; rectal biopsy
Treatment: Praziquantel (drug of choice for all species)
3.2.2 Fasciola hepatica (Liver Fluke)
- Transmission: ingestion of aquatic plants (watercress) with encysted metacercariae
- Intermediate host: freshwater snail (Lymnaea)
- Disease: biliary obstruction, cholangitis, eosinophilia
- Treatment: triclabendazole (NOT praziquantel - resistant)
3.2.3 Clonorchis sinensis (Chinese Liver Fluke)
- Transmission: raw freshwater fish
- Risk: cholangiocarcinoma (biliary)
- Treatment: praziquantel
3.2.4 Paragonimus westermani (Lung Fluke)
- Transmission: raw/undercooked crabs or crayfish
- Disease: pulmonary paragonimiasis - hemoptysis, brown eggs in sputum (mimics TB)
- Egg: oval, shouldered operculum
- Treatment: praziquantel
3.3 NEMATODES (Roundworms)
Key concept: Nematodes have separate sexes. Eosinophilia during migration phase.
3.3.1 Intestinal Nematodes
Ascaris lumbricoides (Giant Roundworm)
- Largest intestinal nematode (up to 35 cm)
- Transmission: fecal-oral, ingestion of embryonated eggs
- Löffler's syndrome (pulmonary eosinophilia) during larval migration through lungs
- Worms may obstruct intestines, bile duct, appendix
- Diagnosis: eggs in stool (mammillated outer coat), adults may be passed in stool
- Treatment: albendazole or mebendazole
Enterobius vermicularis (Pinworm)
- Most common helminth infection in the US
- Transmission: fecal-oral, autoinfection; nocturnal perianal migration of female worm
- Perianal pruritus (especially nocturnal) = hallmark
- Diagnosis: Scotch tape test (cellophane tape applied to perianal area at night)
- Eggs: asymmetrically flattened on one side ("D-shaped")
- Treatment: mebendazole or albendazole (repeat dose in 2 weeks); treat entire household
Hookworm (Ancylostoma duodenale, Necator americanus)
- Transmission: filariform larvae penetrate intact skin (walking barefoot)
- "Ground itch" at entry site; Löffler's syndrome during lung migration
- Adults attach to small intestinal mucosa → iron-deficiency anemia (blood-sucking)
- A. duodenale also transmits via ingestion/breast milk; more aggressive blood-sucking
- N. americanus = most common hookworm worldwide (Americas, Africa, Asia)
- Diagnosis: eggs in stool (thin shell, 4-8 cell morula inside)
- Treatment: albendazole or mebendazole + iron supplementation
Trichuris trichiura (Whipworm)
- Transmission: fecal-oral (embryonated eggs)
- Egg: "barrel/football" shaped with 2 polar plugs (pathognomonic)
- Anterior end (thin/whip) embeds in mucosa; posterior (thick) hangs free
- Heavy infection: "whip-worm dysentery," rectal prolapse in children
- Treatment: mebendazole or albendazole
Strongyloides stercoralis
- Unique: can cause hyperinfection/dissemination in immunocompromised hosts
- Transmission: filariform larvae penetrate skin; unique direct development cycle
- Autoinfection possible (larvae can penetrate intestinal wall without leaving host)
- Hyperinfection in corticosteroid users, HTLV-1 infection, transplant recipients
- Larva currens = rapidly migrating urticarial track in skin
- Diagnosis: stool O&P (rhabditiform larvae); serology (ELISA); Baermann technique
- Treatment: ivermectin (drug of choice); albendazole as alternative
3.3.2 Tissue Nematodes
Wuchereria bancrofti / Brugia malayi - Lymphatic Filariasis
- Vector: Culex mosquito (W. bancrofti), Mansonia/Anopheles (B. malayi)
- Disease: lymphatic obstruction → elephantiasis (lymphedema of limbs/scrotum)
- Microfilariae show nocturnal periodicity (peak at night in peripheral blood)
- Diagnosis: blood smear (thick film, midnight sample); microfilariae in blood
- Treatment: DEC (diethylcarbamazine) ± albendazole; ivermectin + albendazole
Onchocerca volvulus - River Blindness
- Vector: Simulium (blackfly), breeds in fast-flowing rivers
- Disease: skin nodules (onchocercomas), dermatitis ("leopard skin"), blindness (keratitis, chorioretinitis from microfilariae dying in eye)
- No blood microfilaremia (microfilariae stay in skin/eye)
- Diagnosis: skin snip (not blood) - microfilariae in superficial skin; slit lamp exam
- Treatment: Ivermectin (drug of choice, mass distribution program); kills microfilariae NOT adults; DEC is contraindicated (causes Mazzotti reaction → severe inflammation)
Loa loa (African Eye Worm)
- Vector: Chrysops (mango fly / deer fly)
- Disease: Calabar swellings (transient migratory subcutaneous edema), adult worm migrating across conjunctiva
- Diurnal periodicity of microfilariae (peak during daytime)
- Diagnosis: microfilariae in daytime blood sample; observing worm under conjunctiva
- Treatment: DEC
PART 4 - IMPORTANT PARASITIC DISEASES (Detailed)
4.1 ASCARIASIS
- Causative agent: Ascaris lumbricoides
- Transmission: ingestion of embryonated eggs (fecal-oral); contaminated soil/vegetables
- Life cycle highlights:
- Eggs ingested → hatch in small intestine → larvae penetrate intestinal wall
- Larvae migrate via portal blood → liver → heart → lungs (Löffler's syndrome)
- Larvae migrate up trachea → swallowed → mature in small intestine
- Adults (up to 35 cm) live in jejunum
- Clinical:
- Pulmonary phase: cough, wheezing, eosinophilia (Löffler's syndrome)
- Intestinal phase: usually asymptomatic; heavy infection → malnutrition, obstruction
- Complications: biliary/pancreatic duct obstruction, intestinal obstruction, appendicitis
- Diagnosis: Eggs in stool (fertilized egg: oval, brown, mammillated); unfertilized eggs also seen
- Treatment: Albendazole (400 mg single dose) or mebendazole; pyrantel pamoate
4.2 ENTEROBIASIS (Pinworm)
- Causative agent: Enterobius vermicularis
- Epidemiology: Most common helminth in USA; mainly children, institutional settings
- Transmission: Fecal-oral, autoinfection, airborne (eggs can float in dust)
- Life cycle: Eggs ingested → mature in cecum → females migrate to perianal area at night to deposit eggs → pruritus ani
- Complications: Secondary bacterial infection from scratching; rarely appendicitis; vaginal/pelvic migration in girls
- Diagnosis: Scotch tape test (morning, before bathing) - asymmetric D-shaped eggs
- Treatment: Mebendazole or albendazole (single dose, repeat in 2 weeks); treat all household members; hygiene measures
4.3 HOOKWORM DISEASE
- Causative agents: Ancylostoma duodenale (Old World), Necator americanus (New World)
- Transmission: Filariform (L3) larvae in warm moist soil penetrate intact skin
- Life cycle:
- L3 larvae penetrate skin → blood → lungs (Löffler's syndrome) → swallowed
- Mature in small intestine; attach to mucosa by buccal capsule with teeth/plates
- Blood-sucking causes iron deficiency anemia and hypoalbuminemia
- Clinical:
- "Ground itch" (dermatitis at penetration site)
- Pulmonary migration symptoms
- Iron-deficiency anemia (most important complication): weakness, pallor, dyspnea
- Hypoproteinemia, growth retardation in children
- Diagnosis: Eggs in stool; Harada-Mori filter paper technique to detect larvae
- Treatment: Albendazole or mebendazole; iron supplementation; nutritional support
4.4 FILARIASIS
- See tissue nematodes section above
- Key summary:
| Parasite | Vector | Microfilariae periodicity | Key disease | Dx sample |
|---|---|---|---|---|
| Wuchereria bancrofti | Culex mosquito | Nocturnal | Elephantiasis | Midnight blood |
| Brugia malayi | Mansonia/Anopheles | Nocturnal | Elephantiasis (arms) | Midnight blood |
| Loa loa | Chrysops fly | Diurnal | Calabar swellings, eye worm | Daytime blood |
| Onchocerca volvulus | Simulium blackfly | N/A (skin) | River blindness | Skin snip |
| Mansonella spp. | Midges (Culicoides) | Aperiodic | Mild/asymptomatic | Blood |
4.5 TRICHINELLOSIS (Trichinosis)
- Causative agent: Trichinella spiralis (and related species)
- Transmission: Ingestion of undercooked pork (or bear, wild boar) containing encysted larvae
- Unique: Humans are accidental dead-end hosts; the same individual is both definitive and intermediate host
- Life cycle:
- Encysted larvae in muscle → ingested → released in stomach → mature in small intestinal enterocytes
- Female worms release larvae → penetrate mucosa → migrate via blood → encyst in striated muscle (preferred: diaphragm, intercostal muscles, tongue, extraocular muscles)
- Clinical phases:
- Intestinal phase (day 1-7): nausea, vomiting, diarrhea
- Muscle invasion phase (day 7-21): myalgia (especially jaw, tongue, extraocular), periorbital edema (classic!), fever, eosinophilia
- Encystment phase: symptoms subside; calcified cysts remain in muscle
- Classic presentation: Periorbital edema + myalgia + eosinophilia after eating pork
- Diagnosis: Serology; muscle biopsy (encysted larvae "nurse cells"); CBC (marked eosinophilia); elevated CK
- Treatment: Albendazole or mebendazole + corticosteroids (for severe cases)
4.6 DRACUNCULIASIS (Guinea Worm Disease)
- Causative agent: Dracunculus medinensis
- Transmission: Ingestion of cyclops (copepods/water fleas) in contaminated drinking water
- Life cycle:
- Cyclops in water ingested → larvae released in intestine → penetrate gut wall → mature in retroperitoneum
- Gravid female (up to 1 m long!) migrates to skin (usually lower leg) over ~1 year
- Female creates blister → ruptures on contact with water → releases larvae into water → cyclops ingest larvae
- Clinical:
- Mostly asymptomatic during migration
- Blister and ulcer on lower extremity; intensely painful
- Secondary bacterial infection is the main complication
- Severe: arthritis, septicemia
- Diagnosis: Clinical (visible worm emerging from skin); no effective serological test
- Treatment: No drug treatment! Traditional slow extraction: wind worm around stick (a few cm/day over weeks); cannot pull quickly (worm breaks → anaphylaxis + severe infection)
- Prevention/Eradication: Filtering drinking water through fine cloth/pipe filter; education; DEET in water sources to kill cyclops. Currently near-complete global eradication (Carter Center program)
4.7 CHAGAS DISEASE (American Trypanosomiasis)
- Causative agent: Trypanosoma cruzi
- Vector: Triatomine bug (Triatoma, Rhodnius, Panstrongylus) = "Kissing bug" / "Reduviid bug"
- Transmission: Bug defecates near bite wound; parasite in feces enters wound (NOT the bite itself); also: blood transfusion, congenital, organ transplant, undercooked food
- Distribution: Central and South America
- Life cycle:
- Trypomastigotes in bug feces enter wound → enter macrophages → transform to amastigotes (intracellular)
- Amastigotes replicate in tissue cells (especially heart muscle) → rupture → release trypomastigotes → infect other cells or ingested by another bug
Clinical Phases:
| Phase | Features |
|---|---|
| Acute | Romaña's sign (painless periorbital edema = entry via conjunctiva), chagoma (skin nodule at entry site), fever, lymphadenopathy, hepatosplenomegaly; rarely myocarditis/meningitis in children |
| Indeterminate | Asymptomatic, positive serology, normal ECG/imaging; most remain here |
| Chronic | Chagasic cardiomyopathy (dilated, arrhythmias, heart failure, sudden death); megaesophagus and megacolon (enteric nerve destruction) |
Romaña's sign = unilateral painless periorbital edema = classic sign of acute Chagas
"Megadisease" = hallmark of chronic Chagas (megaesophagus, megacolon)
Diagnosis:
- Acute: blood smear (trypomastigotes with C/U shape), buffy coat; PCR
- Chronic: serology (2 different tests required per WHO); xenodiagnosis (let clean bugs feed on patient then examine bug feces - gold standard historically)
- ECG: right bundle branch block + left anterior fascicular block is classic Chagas pattern
Treatment:
- Nifurtimox or benznidazole - effective in acute phase; limited efficacy in chronic phase
- Chronic cardiomyopathy: standard heart failure treatment, ICD, transplant
Compare with African Trypanosomiasis:
| Feature | Chagas (American) | African Sleeping Sickness |
|---|---|---|
| Agent | T. cruzi | T. brucei gambiense/rhodesiense |
| Vector | Triatome (kissing bug) | Tsetse fly (Glossina) |
| Transmission | Feces in wound | Bite |
| Reservoir | Many mammals | Humans (gambiense), animals (rhodesiense) |
| Target | Heart/GI tract (intracellular) | CNS (extracellular) |
| CNS disease | Rare | Hallmark (sleeping sickness) |
| Treatment | Nifurtimox/Benznidazole | Suramin, melarsoprol, eflornithine |
PART 5 - LABORATORY DIAGNOSIS OF PARASITES
Stool Examination (O&P - Ova and Parasites)
- Specimen requirement: 3 specimens collected at least 24 hours apart (to account for intermittent shedding)
- Fresh specimen: examine within 1 hour; if delay, use preservative (formalin, PVA, SAF)
- Do NOT refrigerate specimens if cultured for free-living amoeba
Techniques:
| Technique | Purpose |
|---|---|
| Direct wet mount | Motile trophozoites (Giardia, Trichomonas, amoeba) |
| Concentration methods (zinc sulfate flotation, formalin-ethyl acetate) | Increase sensitivity for cysts/eggs/larvae |
| Permanent stains (Trichrome, Iron hematoxylin) | Morphologic identification of protozoa |
| Modified acid-fast stain | Cryptosporidium, Cyclospora, Cystoisospora (oocysts are acid-fast) |
| Giemsa stain | Blood parasites (malaria, Leishmania, trypanosomes, microfilariae) |
| Scotch tape test | Enterobius vermicularis (pinworm) eggs |
| Kato-Katz | Helminth egg counts (intensity of infection) |
| Harada-Mori | Culture of hookworm/Strongyloides larvae |
| Baermann technique | Strongyloides larvae (uses gravity and heat) |
| Skin snip | Onchocerca volvulus microfilariae |
| NNN/Diamond's medium | Culture of Leishmania (NNN), Trichomonas (Diamond's) |
Blood Parasite Diagnosis:
| Method | Detail |
|---|---|
| Thick blood film | Concentration; used for screening/detection |
| Thin blood film | Morphology; used for species identification |
| Giemsa stain | Standard for blood parasites |
| Wright stain | Alternative to Giemsa |
| Midnight blood sample | Wuchereria (nocturnal microfilariae) |
| Daytime blood sample | Loa loa (diurnal microfilariae) |
| Buffy coat | Trypanosomes, microfilariae concentration |
Immunological Methods:
- Serology (ELISA, IFA, IHA): Toxoplasma, Echinococcus, Leishmania (rK39), Schistosoma, Trypanosoma
- Antigen detection: Giardia/Cryptosporidium (stool EIA/immunochromatography); Plasmodium RDTs (HRP-2)
- PCR: Most sensitive/specific; used for malaria, Toxoplasma, Leishmania, microsporidia, Strongyloides
Parasite by Body Site Summary (from Quick Compendium of Clinical Pathology):
| Body Site | Key Parasites |
|---|---|
| Intestinal tract | Entamoeba, Giardia, Cryptosporidium, Ascaris, Enterobius, hookworm, Strongyloides, Taenia, Schistosoma (eggs) |
| Blood | Plasmodium (RBCs), Leishmania (leukocytes), Trypanosoma, microfilariae |
| CNS | Naegleria fowleri, Acanthamoeba, Toxoplasma, T. solium (neurocysticercosis), Trypanosoma brucei |
| Liver/Spleen | Echinococcus, E. histolytica, Leishmania, Fasciola, Schistosoma |
| Muscle | Trichinella, Taenia (cysticercus), T. cruzi |
| Lungs | Paragonimus, Echinococcus, Strongyloides larvae, Toxoplasma |
| Skin | Leishmania, Onchocerca, microfilariae, Sarcoptes scabiei, Loa loa |
| Urogenital | Trichomonas vaginalis, Schistosoma haematobium (eggs) |
| Eye | Acanthamoeba (keratitis), Toxoplasma (chorioretinitis), Onchocerca, Loa loa |
PART 6 - PREVENTION & CONTROL OF PARASITIC INFECTIONS
General Principles (Interrupting Transmission)
| Strategy | Examples |
|---|---|
| Safe food/water | Boiling/filtering water (Giardia, Cryptosporidium, cholera), cooking meat well (Trichinella, Toxoplasma, Taenia), avoiding raw fish (Diphyllobothrium, Clonorchis) |
| Personal protection | Wearing shoes (hookworm, Strongyloides), insect repellent (DEET), bed nets (malaria, filariasis) |
| Vector control | Insecticides (indoor residual spraying - malaria), larval control, draining stagnant water |
| Sanitation | Proper sewage disposal, handwashing, avoiding open defecation |
| Mass drug administration (MDA) | Ivermectin (onchocerciasis, lymphatic filariasis), DEC + albendazole (LF elimination program) |
| Animal reservoir control | Treating dogs (Echinococcus, Leishmania), meat inspection (Taenia, Trichinella) |
| Chemoprophylaxis | Malaria prophylaxis (chloroquine, mefloquine, doxycycline, atovaquone-proguanil) |
| Water filtering | Dracunculiasis - filtering with pipe filter/cloth |
| Vaccination | No licensed human vaccines for most parasites; trials ongoing for malaria (RTS,S/AS01 = MosquirixTM) |
Disease-Specific Control:
| Disease | Key Control Measures |
|---|---|
| Malaria | Insecticide-treated bed nets (ITNs), IRS (indoor residual spraying), ACT treatment, RTS,S vaccine (partial efficacy), chemoprophylaxis |
| Filariasis | Annual MDA (albendazole + ivermectin or DEC), vector control, morbidity management (lymphedema care) |
| Onchocerciasis | Annual ivermectin MDA (CDTI - community-directed treatment); blackfly control (larviciding rivers) |
| Dracunculiasis | Water filtering, health education, case containment, ABATE (temephos) in water sources; near eradication globally |
| Chagas Disease | Triatomine bug control (insecticide spraying), blood screening, congenital screening |
| Schistosomiasis | Praziquantel MDA, snail control (molluscicides), avoiding contaminated water, sanitation |
| Soil-transmitted helminths | Periodic deworming (MDA with albendazole/mebendazole), sanitation, hygiene education |
| Giardia/Cryptosporidium | Water treatment (boiling, filtration, UV - NOT chlorination for Cryptosporidium), handwashing |
| Neurocysticercosis | Meat inspection, sanitation, pork cooking, taeniasis treatment in communities |
| Toxoplasmosis | Avoid cat litter in pregnancy, cook meat well, wash produce; screening of pregnant women |
HIGH-YIELD MNEMONICS & QUICK FACTS
Malaria Species Memory Aid: "FaKt Vivid Oh My"
- Falciparum - malignant tertian, cerebral, banana gametocytes
- Knowlesi - quotidian, zoonosis (monkeys, SE Asia)
- Tertian benign = Vivax - largest distribution, Schüffner's dots
- Ovale - benign tertian, Africa
- Mylariae (Malariae) - quartan (72h), nephrotic syndrome
Drug-Parasite Matches (High Yield):
| Drug | Key Use |
|---|---|
| Metronidazole | Giardia, E. histolytica, Trichomonas |
| Praziquantel | Most cestodes and trematodes |
| Albendazole | Broad spectrum: roundworms, hookworm, Echinococcus, neurocysticercosis |
| Mebendazole | Soil-transmitted helminths (Ascaris, hookworm, Trichuris, pinworm) |
| Ivermectin | Strongyloides (DOC), Onchocerca (DOC), lymphatic filariasis, scabies |
| DEC | Lymphatic filariasis (W. bancrofti, Brugia), Loa loa |
| Pyrimethamine + sulfadiazine | Toxoplasmosis |
| Nifurtimox / Benznidazole | Chagas disease |
| Triclabendazole | Fasciola hepatica (NOT praziquantel) |
| Primaquine | Radical cure of P. vivax/ovale (kills hypnozoites) |
| Artesunate (IV) | Severe malaria |
| Liposomal amphotericin B | Visceral leishmaniasis (drug of choice) |
| Amphotericin B | Naegleria fowleri PAM |
Vectors Summary:
| Vector | Parasite |
|---|---|
| Anopheles mosquito | Plasmodium (malaria) |
| Aedes mosquito | Brugia timori; also Dengue, Zika (not parasitic) |
| Culex mosquito | Wuchereria bancrofti, Brugia malayi |
| Simulium blackfly | Onchocerca volvulus |
| Chrysops (deer/mango fly) | Loa loa |
| Phlebotomus sandfly | Leishmania (Old World) |
| Lutzomyia sandfly | Leishmania (New World) |
| Tsetse fly (Glossina) | T. brucei (African sleeping sickness) |
| Triatomine bug (kissing bug) | T. cruzi (Chagas disease) |
| Cyclops (water flea) | Dracunculus medinensis |
| Freshwater snail | Schistosoma (cercariae), Fasciola, Paragonimus |
| Ixodes tick | Babesia |
Sources: Quick Compendium of Clinical Pathology 5th ed. | Medical Microbiology 9e (Murray, Rosenthal, Pfaller) | Sherris & Ryan's Medical Microbiology 8th ed. | Jawetz, Melnick & Adelberg's Medical Microbiology 28th ed.
This is a shared conversation. Sign in to Orris to start your own chat.