Scalp
Reading File
Finding Sources
Searching the Web
scalp anatomy layers clinical significance
Reading File
Reading File
Loading Image
Reading File
Loading Image
I now have comprehensive information from Gray's Anatomy for Students. Let me compose the full answer.
The Scalp
The scalp covers the cranial vault, extending from the superciliary arches (anteriorly) to the external occipital protuberance and superior nuchal lines (posteriorly), and laterally down to the zygomatic arch.
Layers - the SCALP Mnemonic
The five layers are remembered by the word SCALP:
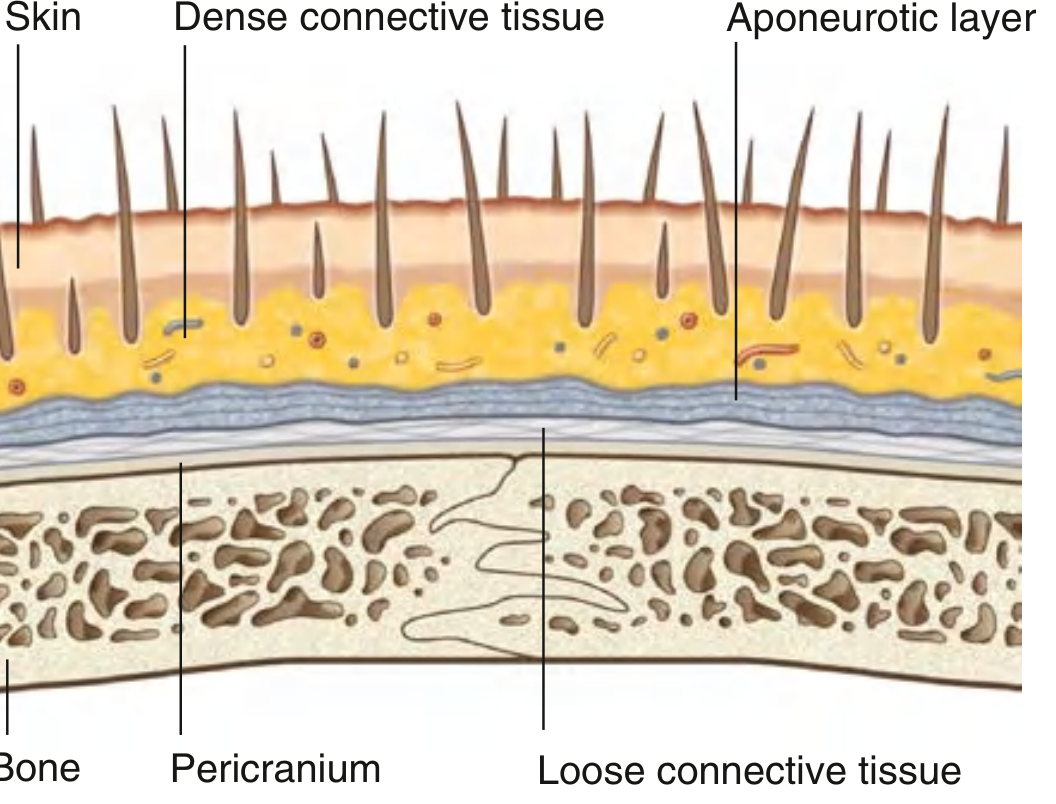
| Layer | Description |
|---|---|
| S - Skin | Contains hair follicles, sebaceous and sweat glands |
| C - Connective tissue (dense) | Fibrofatty layer anchoring skin to aponeurosis; contains all vessels and nerves |
| A - Aponeurotic layer (galea aponeurotica) | Tendinous sheet of the occipitofrontalis muscle |
| L - Loose areolar connective tissue | The "danger zone" - allows fluid/blood spread and scalp mobility |
| P - Pericranium | Dense periosteum firmly adherent to the outer surface of the calvaria |
The first three layers (S + C + A) are tightly fused and move as a single unit - this is the tissue avulsed in "scalping" injuries.
The Aponeurotic Layer (Galea Aponeurotica) in Detail
The aponeurotic layer is the tendon of the occipitofrontalis muscle, which has:
- A frontal belly - attached to the skin of the eyebrows, innervated by temporal branches of CN VII (facial nerve)
- An occipital belly - arises from the superior nuchal line and mastoid process, innervated by the posterior auricular branch of CN VII
- Functions: moves the scalp, wrinkles the forehead, raises the eyebrows
The "Danger Zone" - Loose Areolar Layer (Layer 4)
This layer is clinically significant for several reasons:
- It allows the superficial three layers to glide freely over the pericranium
- It contains emissary veins - valveless veins connecting extracranial scalp veins to intracranial dural venous sinuses (e.g., superior sagittal sinus)
- Because emissary veins are valveless, infection in this layer can spread intracranially, giving it the name "danger zone"
- Blood or pus can spread widely within this layer, reaching both upper eyelids (as in a "black eye" after a forehead blow)
Arterial Supply
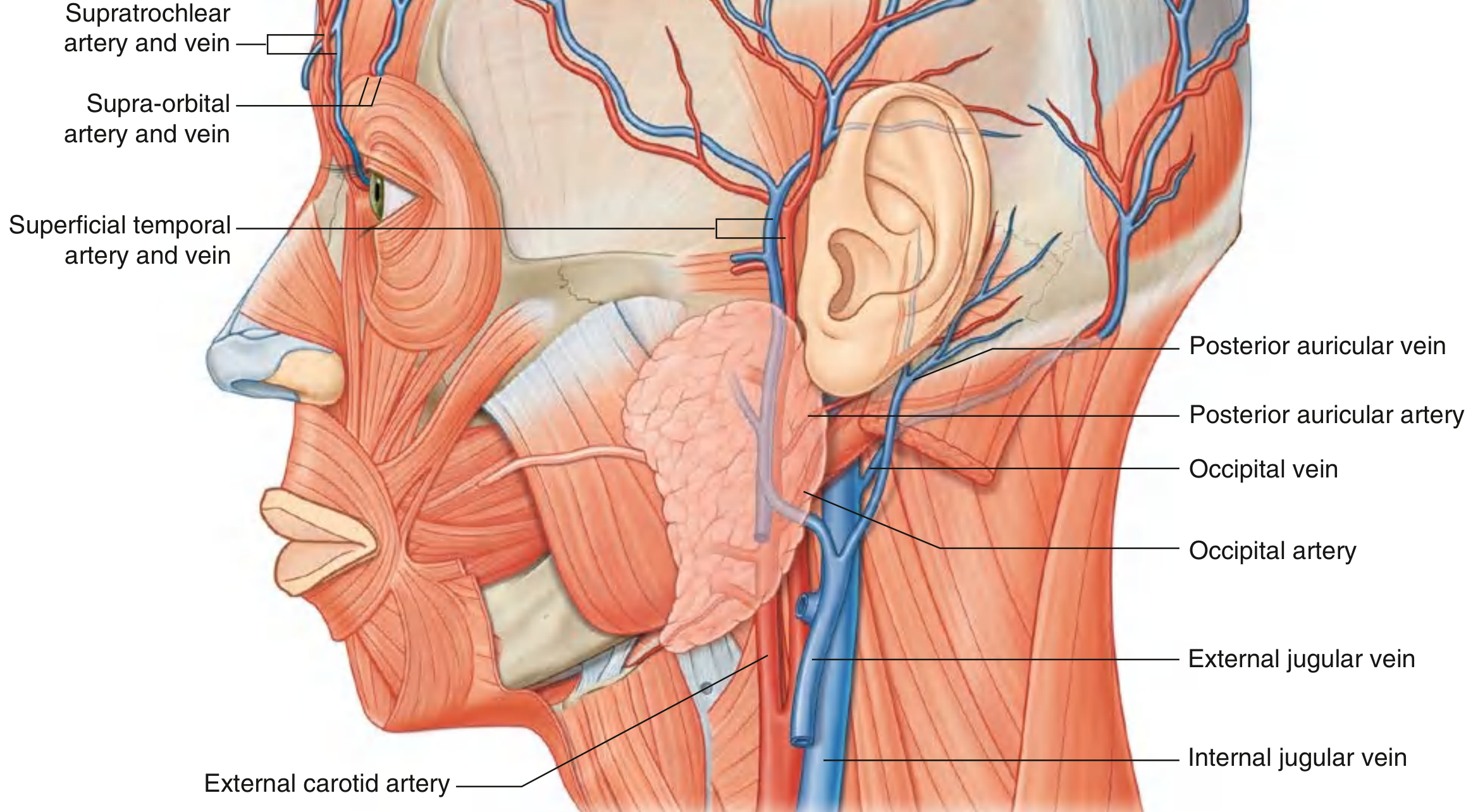
The scalp has a rich, anastomotic arterial supply from two sources:
From the ophthalmic artery (branch of internal carotid):
- Supratrochlear artery - anterior scalp
- Supra-orbital artery - anterior/superior scalp, reaching the vertex
From the external carotid artery:
- Superficial temporal artery (terminal branch) - entire lateral scalp; divides into anterior and posterior branches just anterior to the ear
- Posterior auricular artery - scalp posterior to the ear
- Occipital artery - large part of the posterior scalp
All five arteries anastomose freely across the midline, making the scalp highly resistant to ischemia and able to survive large flaps - but also difficult to stop bleeding from.
Venous Drainage
Venous drainage mirrors the arterial pattern:
- Supratrochlear and supra-orbital veins → angular vein → facial vein
- Superficial temporal vein → retromandibular vein
- Posterior auricular vein → retromandibular vein tributary
- Occipital vein → suboccipital venous plexus
Nerve Supply
The scalp receives sensory innervation from branches of CN V (trigeminal) anteriorly and cervical plexus posteriorly:
| Nerve | Origin | Territory |
|---|---|---|
| Supratrochlear | V1 (ophthalmic) | Medial forehead |
| Supra-orbital | V1 (ophthalmic) | Anterior scalp to vertex |
| Zygomaticotemporal | V2 (maxillary) | Small lateral area near temple |
| Auriculotemporal | V3 (mandibular) | Temporal scalp |
| Greater occipital | Posterior ramus C2 | Large area of posterior scalp to vertex |
| Lesser occipital | Anterior ramus C2 | Scalp behind the ear |
| Great auricular | C2/C3 | Just posterior to ear |
| Third occipital | Posterior ramus C3 | Lower posterior scalp |
Lymphatic Drainage
Lymphatic drainage follows the arterial pattern:
- Occipital region → occipital nodes → upper deep cervical nodes
- Posterior vertex → mastoid (retroauricular) nodes → upper deep cervical nodes
- Anterior vertex → preauricular/parotid nodes
- Forehead → submandibular nodes (via facial artery route)
Key Clinical Points
-
Profuse bleeding from lacerations: The dense connective tissue (layer 2) holds cut vessels open, preventing them from retracting and constricting. Bleeding is predominantly arterial due to low venous pressure in the erect position. - Gray's Anatomy for Students
-
Danger zone infections: Infections in the loose areolar layer (layer 4) can spread intracranially via valveless emissary veins → meningitis, cavernous sinus thrombosis.
-
Subgaleal hematoma vs. cephalhematoma: In neonates, a subgaleal hematoma (in layer 4) can cross suture lines and spread widely; a cephalhematoma (between pericranium and bone) is confined to one bone by periosteal attachments.
-
Scalp flaps in surgery: Due to the rich anastomotic blood supply, large scalp flaps survive on a single pedicle - exploited in reconstructive surgery.
-
Scalp blocks for anesthesia: The five terminal nerves entering the scalp peripherally can all be blocked at the scalp margin for regional anesthesia (e.g., awake craniotomy). - Miller's Anesthesia
Gray's Anatomy for Students, pp. 1062-1066
This is a shared conversation. Sign in to Orris to start your own chat.