Hiii
Hey! How can I help you today? 😊
Tecah me mullerian anomalies like a child
Reading File
Finding Sources
Finding Sources
Reading File
Reading File
Reading File
Reading File
Reading File
Loading Image
Okay, I've got everything I need! Let me explain Mullerian anomalies like you're hearing it for the first time. 🎉
🍭 Müllerian Anomalies - Like You're 5 (But Also Smart!)
🏗️ First, What ARE the Müllerian Ducts?
Imagine you're building a house. Inside every baby girl's belly, there are two tiny tubes called Müllerian ducts (also called paramesonephric ducts). These two tubes have one very important job: grow together and build the uterus, fallopian tubes, cervix, and upper vagina.
Think of it like two rivers that need to:
- 🌊 Flow (develop properly)
- 🤝 Merge (fuse together in the middle)
- 🧱 Remove the wall between them (resorb the septum)
If ANY of these three steps goes wrong - boom - you get a Müllerian anomaly!
🎭 The 3 Ways Things Can Go Wrong
| Problem | What Happens | Result |
|---|---|---|
| ❌ One duct doesn't grow | Only one tube shows up to the party | Unicornuate uterus |
| 🚫 Ducts don't fuse | The two tubes never join | Didelphys / Bicornuate |
| 🧱 Wall stays behind | Tubes fused but didn't remove the middle wall | Septate uterus |
🏷️ The AFS Classification (Class I - VII)
This is the American Fertility Society system - the most used one. Think of each class as a level of "oops" in building!
🔴 Class I - Müllerian Agenesis / Hypoplasia
"The building materials never arrived!"
The ducts just... didn't develop. The uterus, cervix, or vagina is missing or tiny.
- The big one here is MRKH Syndrome (Mayer-Rokitansky-Küster-Hauser)
- Girl has normal 46,XX chromosomes, normal ovaries, normal female hormones
- She looks totally normal on the outside - develops breasts, pubic hair
- BUT - has no uterus, no upper vagina
- Often found when she's a teenager and never gets her period (primary amenorrhea)
- May also have kidney problems, skeletal issues, or hearing problems
🔑 Key fact: MRKH accounts for 10-15% of all primary amenorrhea cases!
🟠 Class II - Unicornuate Uterus
"Only one side of the factory was built!"
One Müllerian duct develops, the other one mostly or completely fails.
- Uterus looks like a banana 🍌 - curved to one side
- May have a rudimentary (tiny, useless) horn on the other side
- Subtypes depend on whether the rudimentary horn has a cavity and whether it communicates
- The scariest subtype: a non-communicating horn with endometrium - blood gets trapped = pain = can rupture! (medical emergency)
🟡 Class III - Uterus Didelphys
"Two separate houses were built instead of one!"
Both ducts develop BUT they never fuse at all. You end up with:
- Two uteri
- Two cervices
- Often two vaginas (double vagina / longitudinal vaginal septum)
It looks dramatic on imaging but these women can actually get pregnant! The uterine spaces are just smaller.
🟢 Class IV - Bicornuate Uterus
"Two towers joined at the base!"
The ducts partially fused at the bottom but the tops are still separated. Looks like a heart shape 💙 or ram's horns 🐏 on imaging.
- Bicornuate bicollis = two horns + two cervices
- Bicornuate unicollis = two horns + one cervix (more common)
- Associated with: preterm labor, malpresentation, higher miscarriage risk
🔵 Class V - Septate Uterus
"The wall between the two rooms was never torn down!"
This is the MOST COMMON Müllerian anomaly. The ducts fused properly, but the dividing wall (septum) in the middle stayed behind.
- Uterus looks normal from the OUTSIDE - tricky to diagnose!
- But inside there's a wall (septum) dividing the cavity
- Partial septum = wall is only partway
- Complete septum = wall goes all the way down to the cervix
- This has the WORST reproductive outcomes - highest miscarriage rate
- Good news: It's also the most treatable! Hysteroscopic septum resection works well.
🩺 Differentiating septate (Class V) vs bicornuate (Class IV) is really important because septate is fixed with hysteroscopy while bicornuate may need open surgery - use 3D ultrasound or MRI!
🟣 Class VI - Arcuate Uterus
"Just a tiny dent in the ceiling!"
A mild indentation at the top of the uterine fundus. Barely a blip. Most consider this a normal variant - reproductive outcomes are essentially the same as a normal uterus.
⚫ Class VII - DES-Related Anomalies
"The building materials were contaminated!"
Caused by Diethylstilbestrol (DES) exposure in utero. DES was a drug given to pregnant women in the 1950s-70s to prevent miscarriage - it backfired.
- T-shaped uterus
- Hypoplastic uterus
- Mostly historical now since DES was banned.
🖼️ What They Look Like on X-ray (HSG)
Here are actual hysterosalpingograms (HSG) showing how contrast dye fills different uterine shapes:
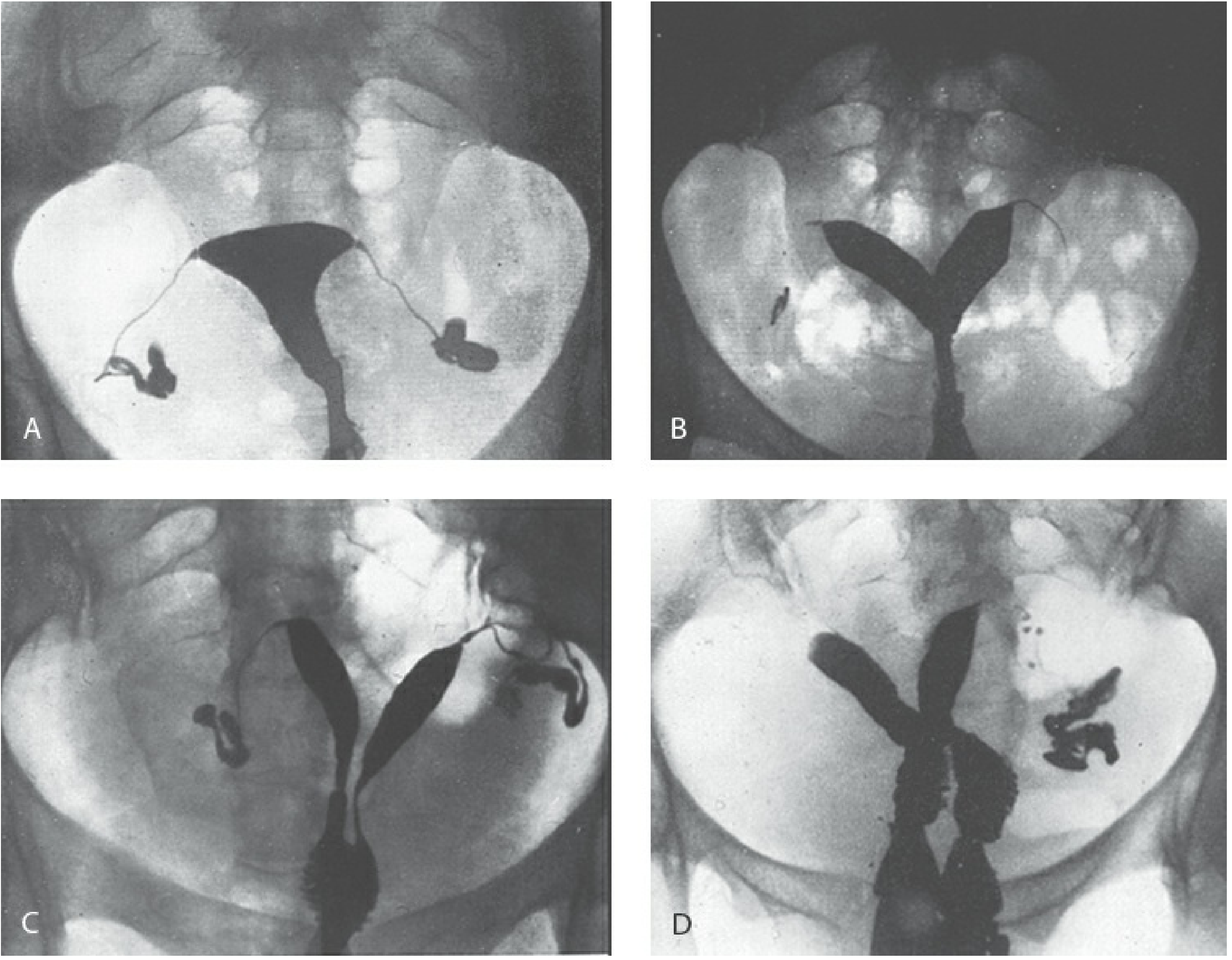
- A = Normal uterus (nice triangle shape)
- B = Bicornuate (two horns, joined at base - like a heart)
- C = Uterus didelphys (two completely separate cavities)
- D = Didelphys with double vagina
🩻 How Do We Diagnose Them?
| Tool | What it does | Best for |
|---|---|---|
| 3D Ultrasound | Non-invasive, first line | Most anomalies - high accuracy |
| MRI | Gold standard when US unclear | Complex anomalies, best for external contour |
| HSG | Dye through cervix + X-ray | Shows internal cavity shape |
| Hysteroscopy | Camera inside uterus | Best for septa, polyps, adhesions |
| Laparoscopy | Camera outside uterus | Differentiates bicornuate vs septate (external view) |
🎯 Key diagnostic challenge: Septate vs Bicornuate - look at the EXTERNAL fundal contour! A septate uterus has a FLAT or slightly indented fundus externally. A bicornuate uterus has a deep external notch (>1 cm).
🍼 What Problems Do They Cause?
- Primary amenorrhea (no periods) - obstructive anomalies
- Recurrent pregnancy loss (RPL) - especially septate uterus
- Preterm labor - less space in the uterus
- Malpresentation - baby can't get into head-down position
- Retained placenta
- Endometriosis - from retrograde blood flow in obstructed anomalies
- Renal anomalies - Müllerian ducts develop alongside the kidney system, so check the kidneys in EVERY patient! (horseshoe kidney, pelvic kidney, absent kidney)
💊 Treatment Summary
| Anomaly | Treatment |
|---|---|
| MRKH / vaginal agenesis | Progressive vaginal dilation (Frank technique) or surgery (McIndoe) |
| Obstructive transverse septum | Surgical excision |
| Imperforate hymen | Simple surgical incision |
| Septate uterus | Hysteroscopic septum resection (most successful, minimally invasive) |
| Unicornuate with painful rudimentary horn | Remove the rudimentary horn |
| Bicornuate / Didelphys | Usually expectant management; metroplasty rarely needed |
🧠 Quick Memory Tricks
- "Fused but walled in" = Septate (Class V) - most common, most fixable
- "Two separate everything" = Didelphys (Class III) - dramatic but liveable
- "Half-built" = Unicornuate (Class II) - one side only
- "Missing parts" = Agenesis/MRKH (Class I) - most severe
- "Always check the kidneys!" - Müllerian + renal development are buddies

IMG_2019.jpg
Make me undeestand the whole topic like a child for my neet pg preparation with basics and make it easy
analyse_media
Reading File
Finding Sources
Finding Sources
Finding Sources
Finding Sources
Reading File
Reading File
Reading File
Finding Sources
Reading File
I have everything I need! Now let me write the full, child-friendly NEET PG guide covering your notes + the whole topic.
🧠 INFERTILITY - NEET PG Complete Guide
(Explained Like a Child, Built for Your Exam!)
🌱 STEP 1: What IS Infertility?
"You've been trying to have a baby but it's just not happening!"
Definition:
- Failure to conceive after 1 year of regular, unprotected intercourse
- If age >35 years → investigate after only 6 months (biological clock is ticking faster!)
Why does age matter? Because after 35, egg quality and quantity decline rapidly. No time to waste!
📊 STEP 2: Who's to Blame? (Causes - MUST MEMORIZE!)
Think of it like a blame pie 🥧:
| Cause | % |
|---|---|
| 👩 Female factor | 30-35% |
| 👨 Male factor | 30% |
| 👫 Both together | 10-15% |
| 🤷 Nobody knows (Idiopathic) | 10-15% |
🔑 NEET PG Trick: Female factor is the MOST COMMON identified cause. But if you add up male + both = ~40-45% involve male factors too!
🔬 STEP 3: First Investigation = SEMEN ANALYSIS
Why start with semen analysis?
Because it's:
- Non-invasive (just a sample)
- Cheap
- Quick
- And male factor = 30% of all cases!
Rules for semen collection:
- 2-7 days abstinence before collection (not more, not less!)
- If results are abnormal → repeat in 4-6 weeks (sperm take ~72 days to form, so wait!)
- If still abnormal → check FSH + Testosterone levels
📋 STEP 4: Normal Semen Analysis Values (WHO 2010)
| Parameter | Normal Value (WHO 2010) |
|---|---|
| Volume | ≥ 1.5 mL |
| Sperm concentration | ≥ 15 million/mL |
| Progressive motility | ≥ 32% |
| Morphology (Strict criteria) | ≥ 4% normal forms |
| WBC | < 1 million/mL |
🎯 NEET Trick: Old WHO 1992 said >20 million/mL. New WHO 2010 says ≥15 million/mL. Exams love testing this difference!
🩺 STEP 5: Semen Analysis Terminology (Easy Memory!)
| Term | Meaning | Memory trick |
|---|---|---|
| Oligozoospermia | Low sperm count | "Oligo" = few |
| Asthenozoospermia | Poor motility | "Astheno" = weak |
| Teratozoospermia | Abnormal shapes | "Terato" = monster |
| Azoospermia | NO sperm at all | "A-zoo" = empty zoo |
| Aspermia | No ejaculate at all | "A" + spermia = nothing comes out |
| Necrozoospermia | All sperm dead | "Necro" = dead |
| OAT | All three abnormal | Oligo + Astheno + Terato |
🏭 STEP 6: APPROACH TO AZOOSPERMIA - The Big One!
Azoospermia = NO sperm in semen. Now we need to figure out WHY!
Think of sperm production like a factory pipeline:
🧠 Brain (Hypothalamus)
↓ sends GnRH
🏛️ Pituitary
↓ sends LH + FSH
🏭 Testes (make sperm + testosterone)
↓ sperm travel through
🚰 Tubes (epididymis → vas deferens → ejaculatory duct)
↓
💧 Ejaculate
If the sperm aren't coming out, the blockage is somewhere in this pipeline. Check FSH + Testosterone to locate it!
🔴 Type 1: PRE-TESTICULAR (Hypothalamus/Pituitary Problem)
FSH ↓ + Testosterone ↓
"The brain forgot to send orders to the factory!"
- The problem is ABOVE the testes
- Hypothalamus or pituitary isn't making GnRH/LH/FSH
- Without FSH → testes don't make sperm
- Without LH → testes don't make testosterone
- Both FSH AND testosterone are LOW = classic pattern
Causes:
- Kallmann syndrome (FSH↓, testosterone↓ + ANOSMIA = can't smell!) - 🌟 NEET FAVOURITE!
- Pituitary tumour (prolactinoma)
- Cushing disease
- Exogenous testosterone use (gym guys taking steroids!)
Treatment: Give back what's missing - GnRH pulses, hCG, exogenous FSH
🟡 Type 2: TESTICULAR (Testes Themselves are Broken)
FSH ↑ + Testosterone ↓
"The factory is broken! Brain is screaming for production but nothing comes out!"
- Testes are damaged → they can't make sperm or testosterone
- Brain senses low testosterone → keeps sending more FSH (hence FSH goes UP)
- This is the MOST COMMON cause of azoospermia!
Causes (remember VOTUM):
- Varicocele 🩸 (most common TREATABLE cause)
- Orchitis (mumps orchitis - classic!)
- Trauma
- Undescended testis (UDT / cryptorchidism)
- Medical - chemo/radiation
NEET High-Yield Extra: Klinefelter syndrome (47,XXY) = FSH↑, testosterone↓ - most common chromosomal cause of male infertility!
🟢 Type 3: POST-TESTICULAR (Obstructive - Plumbing Problem!)
FSH Normal + Testosterone Normal
"The factory is working perfectly! The pipes are just blocked!"
- Testes make sperm normally
- But the tubes that carry sperm out are blocked
- Hormones are BOTH NORMAL (because testes are fine!)
Star Causes:
- Cystic Fibrosis (CF) → Bilateral absence of vas deferens (CBAVD)
- ⚠️ Test CFTR gene mutation!
- Test female partner too!
- Post-infection obstruction (gonorrhoea, TB)
- Post-vasectomy
Special Test: FRUCTOSE TEST 🍬
- Fructose in semen = made by SEMINAL VESICLES
- If fructose is ABSENT → seminal vesicle is blocked/absent (tells you the obstruction is at/above the ejaculatory duct)
- If fructose is PRESENT → obstruction is below the seminal vesicle (e.g. at vas deferens)
🗺️ MASTER TABLE - Azoospermia Types at a Glance
| Pre-testicular | Testicular | Post-testicular | |
|---|---|---|---|
| FSH | ↓ | ↑ | Normal |
| Testosterone | ↓ | ↓ | Normal |
| Testes size | Small | Small/atrophic | Normal |
| Cause | Kallmann, pituitary | Varicocele, orchitis, UDT | CF, obstruction |
| Spermatogenesis | Absent (no stimulus) | Absent (damaged) | Normal! |
| Treatment | Hormones (GnRH, hCG) | Often ICSI/donor | Surgical unblocking / TESE |
💉 STEP 7: TREATMENT Based on Sperm Count
Think of it as: "The fewer sperm, the more help we give!"
| Sperm Count | Treatment | Memory |
|---|---|---|
| 10-15 million/mL | IUI (Intrauterine Insemination) | Put sperm closer to egg |
| 5-10 million/mL | IVF (In Vitro Fertilisation) | Egg + sperm meet in lab |
| < 5 million/mL | ICSI (Inject 1 sperm into egg) | Ultra-severe, one-on-one |
| 0 (Azoospermia) | TESE / TESA / MESE | Surgically extract sperm |
🧰 Surgical Sperm Retrieval Methods:
| Method | Full Name | What it does |
|---|---|---|
| TESE | Testicular Sperm Extraction | Open surgery, cut out testicular tissue |
| TESA | Testicular Sperm Aspiration | Needle into testis, suck out sperm |
| MESE | Microdissection + Sperm Extraction | High-power microscope, best for severe oligospermia |
| MESA | Microsurgical Epididymal Sperm Aspiration | From the epididymis (obstructive cases) |
🎯 NEET tip: ICSI = preferred when sperm count is very low OR when using surgically retrieved sperm (TESE/TESA)
🧩 STEP 8: FEMALE INFERTILITY - Quick Overview
For your notes context, female factor = 30-35%. Main causes:
| Factor | Cause | % of Female Infertility |
|---|---|---|
| Ovulatory dysfunction | PCOS (most common!), hypothyroidism, hyperprolactinaemia | ~40% |
| Tubal factor | PID, endometriosis, previous surgery | ~30% |
| Uterine factor | Fibroids, polyps, Asherman, Müllerian anomalies | ~10% |
| Cervical factor | Hostile mucus, stenosis | ~5% |
| Unexplained | ~10-15% |
⚡ NEET PG HIGH-YIELD FLASH POINTS
| 🏆 Fact | Answer |
|---|---|
| When to start investigating infertility? | 1 year (6 months if age >35) |
| Abstinence before semen analysis? | 2-7 days |
| If abnormal, when to repeat semen analysis? | 4-6 weeks |
| WHO 2010 normal sperm concentration? | ≥15 million/mL |
| Azoospermia with FSH↓ + Testosterone↓? | Pre-testicular (hypothalamic/pituitary) |
| Azoospermia with FSH↑ + Testosterone↓? | Testicular failure (MCC of azoospermia) |
| Azoospermia with Normal FSH + Normal Test? | Obstructive (post-testicular) |
| FSH↓ + Testosterone↓ + ANOSMIA? | Kallmann syndrome |
| Bilateral absence of vas deferens? | Cystic Fibrosis (CFTR mutation) |
| Fructose absent in semen = problem where? | Seminal vesicle or ejaculatory duct |
| Sperm count < 5 million → treatment? | ICSI |
| Sperm count 10-15 million → treatment? | IUI |
| Most common chromosomal cause of male infertility? | Klinefelter syndrome (47,XXY) |
| Most common treatable cause of male infertility? | Varicocele |
🧠 MEMORY PALACE: Azoospermia in 10 Seconds
"Low-Low = Look UP (brain problem)" FSH↓ Testosterone↓ = Pre-testicular = Hypothalamus/Pituitary
"High-Low = Factory BLOWN (testis destroyed)" FSH↑ Testosterone↓ = Testicular failure = orchitis/varicocele/UDT
"Normal-Normal = BLOCKED DRAIN (pipes blocked)" FSH N, Testosterone N = Obstructive = CF/vasectomy
You've got this! 🎉 The key is always to start with FSH + Testosterone to type the azoospermia, then treat accordingly. The note image you shared is a perfect summary - your teacher has nailed the NEET PG essentials right there!
Sources: Berek & Novak's Gynecology, Harrison's Principles of Internal Medicine 22E
This is a shared conversation. Sign in to Orris to start your own chat.