chagas disease
Reading File
Finding Sources
Searching PubMed
"Chagas disease" AND treatment
Searching the Web
Chagas disease overview pathogenesis clinical features treatment 2025
Reading File
Reading File
Reading File
Reading File
Reading File
Reading File
Finding Sources
Finding Sources
Loading Image
Finding Sources
I now have all the content needed for a comprehensive, well-sourced answer. Let me compile it.
Chagas Disease (American Trypanosomiasis)
Definition
Chagas disease, also called American trypanosomiasis, is caused by the protozoan parasite Trypanosoma cruzi. It is a lifelong infection that progresses through acute and chronic phases, with the heart and gastrointestinal (GI) tract as the principal targets of chronic injury.
- Goldman-Cecil Medicine, Chapter 318
The Pathogen
T. cruzi belongs to the genus Trypanosoma. Only two species cause human disease: the African trypanosome T. brucei (sleeping sickness) and the American T. cruzi (Chagas). The parasite exists in three main morphological forms: the trypomastigote (flagellated, circulates in blood), the amastigote (intracellular, replicates within host cells), and the epimastigote (replicates in the insect midgut).
Epidemiology
Vector and Reservoir
- Transmitted by triatomine bugs (reduviid "kissing bugs"), which defecate near their bite wound after taking a blood meal at night. The trypomastigote in insect feces enters through abraded skin or mucous membranes - not through the bite itself.
- Reservoirs: armadillos, wood rats, raccoons, opossums. Dogs are the main domestic reservoir.
- Vectors are found from southern Argentina to the southern United States.
Global Burden
- ~6-8 million people chronically infected in 21 endemic countries (Latin America, not Caribbean islands)
- ~28,000 new cases and ~12,000 deaths annually (PAHO, 2018)
- Vector control programs since 1991 have dramatically reduced transmission; Uruguay (1997), Chile (1999), and Brazil (2006) were certified free of vector transmission.
United States
- Estimated 240,000-350,000 T. cruzi-infected persons in the US, mainly Latin American immigrants
- Autochthonous (locally acquired) acute Chagas disease is extremely rare - only 7 confirmed cases ever reported
- Blood donor screening started in 2007; ~1 in 13,300 donors confirmed positive
- 63-315 babies estimated born with congenital Chagas disease per year in the US
Other Routes of Transmission
-
Blood transfusion and organ transplantation
-
Congenital (mother-to-child)
-
Oral (contaminated food or juice - documented outbreaks in Brazil)
-
Laboratory accidents
-
Goldman-Cecil Medicine, Chapter 318; Rosen's Emergency Medicine, Chapter
Lifecycle
- Triatomine bug ingests blood from an infected mammal, taking up trypomastigotes
- Trypomastigotes differentiate into epimastigotes in the midgut, then back into metacyclic trypomastigotes in the hindgut
- Bug defecates near the bite; trypomastigotes in feces enter host through wound, conjunctiva, or mucosa
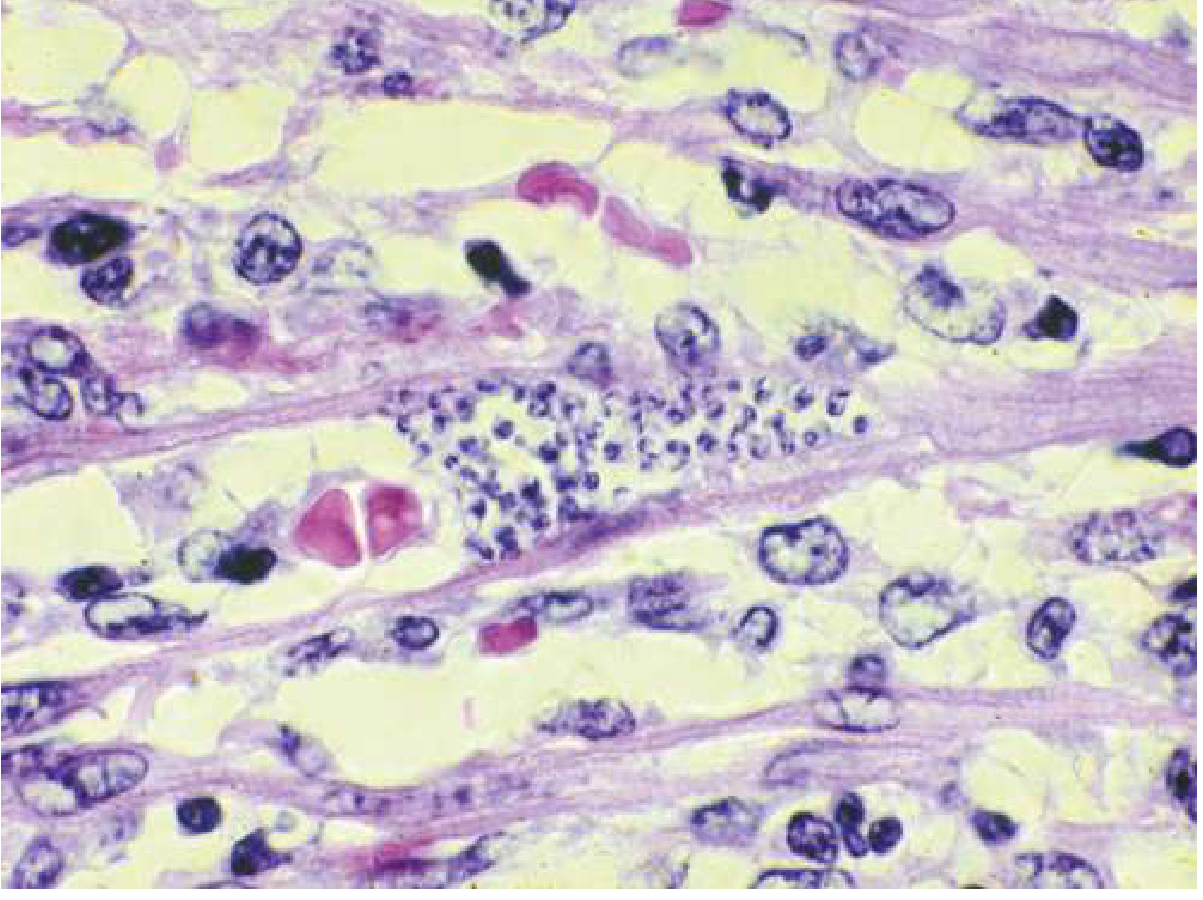
- Inside host cells (cardiac myocytes, smooth muscle, macrophages), trypomastigotes convert to amastigotes and replicate by binary fission
- Amastigotes convert back to trypomastigotes, rupture the cell, and disseminate via bloodstream
- A feeding bug ingests trypomastigotes from infected blood, completing the cycle
Pathobiology
Acute Phase
The parasite invades virtually any nucleated cell but has tropism for cardiac muscle, smooth muscle, and autonomic ganglia. Local tissue destruction and inflammatory response drive acute illness.
Chronic Phase - Cardiac
Hearts at autopsy show biventricular enlargement, ventricular wall thinning, mural thrombi, and a characteristic apical aneurysm of the left ventricle. At the cellular level: chronic mononuclear cell infiltration, diffuse interstitial fibrosis, and myocyte atrophy. The conduction system is selectively affected. PCR studies have shown a correlation between parasite persistence and tissue inflammation - the current consensus favors persistent parasite-driven inflammation (not autoimmunity) as the main pathogenetic mechanism.
Chronic Phase - GI (Mega-syndromes)
Destruction of neurons in the myenteric plexus (Auerbach's plexus) causes parasympathetic denervation. Esophageal dysfunction appears after ~50% of ganglia are lost, and megaesophagus/megacolon develops after ~90% loss. The esophagus and colon are most commonly affected; the ureters, biliary tree, and other hollow viscera can also be involved.
Clinical Phases
1. Acute Phase
- Usually affects children; can occur at any age
- Chagoma: indurated skin lesion at site of parasite entry, with local lymphadenopathy
- Romaña sign (pathognomonic but rarely seen): painless, unilateral periorbital/palpebral edema when conjunctiva is the entry point
- Systemic: fever, malaise, anorexia, facial and lower extremity edema, generalized lymphadenopathy, hepatosplenomegaly
- Severe myocarditis (occasionally fatal) and rare meningoencephalitis can occur
- Resolves spontaneously in 6-8 weeks even without treatment, transitioning to the indeterminate phase
2. Indeterminate (Latent) Phase
- Subpatent parasitemia, no symptoms or signs
- Specific IgG antibodies detectable
- Can persist for the patient's lifetime (~70-80% of infected people remain here forever)
3. Chronic Phase (develops in ~20-30% of infected persons over years to decades)
Chronic Chagas Cardiomyopathy (most common cause of death)
- ECG changes: RBBB, left anterior fascicular block, PVCs - often the earliest signs
- Arrhythmias: ventricular tachycardia, complete heart block, atrial fibrillation, sudden cardiac death
- Sustained monomorphic VT from scar-related reentry (typically inferolateral LV, RBBB morphology with right axis)
- Biventricular dilated cardiomyopathy; right-sided failure predominates in advanced disease
- Apical LV aneurysm - characteristic feature
- Mural thrombi leading to stroke, pulmonary embolism, or peripheral arterial embolism
- Chronic Chagas disease is an independent risk factor for stroke
GI Chagas (Mega-syndromes)
- Megaesophagus: dysphagia, regurgitation, aspiration - indistinguishable from idiopathic achalasia manometrically and radiographically; LES dysfunction occurs late
- Megacolon: constipation, obstipation, toxic megacolon risk
- Other: megaduodenum, megaureter
Diagnosis
Acute Phase
- Wet mount / Giemsa-stained blood smear: motile trypomastigotes in anticoagulated blood or buffy coat
- PCR: most sensitive method; also used for congenital disease and immunosuppression-driven reactivation
- Culture in special liquid media (slower)
Chronic Phase
- Serology (standard): requires two different positive tests (ELISA + indirect immunofluorescence, or chemiluminescence) detecting IgG against T. cruzi antigens
- Cross-reactions can occur with malaria, syphilis, leishmaniasis, and some collagen vascular diseases
- PCR sensitivity in chronic disease is 44-100% - useful for borderline serology, suspected congenital/acute disease, or post-treatment monitoring; a negative PCR does not exclude infection
Treatment
Antiparasitic Drugs
| Drug | Dosing | Duration | Notes |
|---|---|---|---|
| Benznidazole | 5-7 mg/kg/day (adults); 5-10 mg/kg/day (neonates/children) orally in 2 divided doses | 60 days | Drug of choice; FDA-approved for ages 2-12; fewer side effects |
| Nifurtimox | Adults 8-10 mg/kg/day; adolescents 12.5-15; children 15-20 mg/kg/day in 4 divided doses | 90-120 days | FDA-approved for <18 yrs (2020); obtain via CDC if needed (404-639-2888) |
Indications for treatment:
- All patients with acute or congenital infection
- All chronically infected children up to age 18
- Reasonable to treat anyone up to age 18 years known to have acquired infection within the past 17 years
Efficacy:
- Congenital Chagas in neonates: >90% cure with benznidazole
- Acute phase (nifurtimox): ~70% parasitologic cure; reduces symptoms and mortality
- Adults with long-standing chronic infection: cure rates may be <10%
- The landmark BENEFIT trial (adults with established Chagas cardiomyopathy treated with benznidazole) showed that parasitemia suppression did not translate into reduced cardiac outcomes - this remains the subject of ongoing debate
Side effects:
- Benznidazole: rash, peripheral neuropathy, granulocytopenia
- Nifurtimox: anorexia, nausea/vomiting, weight loss, insomnia, restlessness, paresthesias, polyneuritis, seizures
Symptomatic Management (Chronic Chagas Cardiomyopathy)
- Heart failure: standard therapy (ACE inhibitors, beta-blockers, diuretics, aldosterone antagonists)
- Arrhythmias: antiarrhythmics, ICD placement for sustained VT or high risk of sudden death
- Heart block: permanent pacemaker
- Thromboembolism: anticoagulation
- End-stage: cardiac transplantation (with immunosuppression monitoring for reactivation)
GI Mega-syndromes
- Treatment of megaesophagus/megacolon mirrors that of idiopathic achalasia (pneumatic dilation, surgical myotomy for esophagus; bowel resection for severe megacolon)
- Antiparasitic treatment is of no proven benefit for established chronic GI disease
Special Populations
Immunocompromised Patients (HIV, transplant)
- T. cruzi reactivation can occur, presenting with severe myocarditis or meningoencephalitis
- A 2024 systematic review (PMID 38697392) found pooled reactivation rates are substantial and that this remains a serious concern in transplant recipients
Pregnancy / Congenital Chagas
- Congenital transmission rate ~5% in seropositive mothers
- Most congenitally infected babies are asymptomatic, but some have fever, hepatosplenomegaly, myocarditis
- All babies born to seropositive mothers should be tested
Prevention and Control
- Vector control: insecticide spraying of domiciliary triatomines, housing improvement (replastering walls, replacing thatched roofs)
- Blood donor screening: universal in endemic countries; selective in the US since 2007
- Organ donor screening: recommended for donors from endemic regions
- No vaccine currently available
Key Points Summary
| Feature | Detail |
|---|---|
| Pathogen | Trypanosoma cruzi |
| Vector | Triatomine (kissing) bugs |
| Transmission | Fecal contamination of bite wound; also transfusion, congenital, oral, transplant |
| Pathognomonic sign | Romaña sign (unilateral painless periorbital edema) |
| Cardiac hallmark | Apical LV aneurysm + RBBB + dilated cardiomyopathy |
| Histology | Amastigote nests in myocytes |
| Drug of choice | Benznidazole (especially in children and early infection) |
| Indeterminate phase | Asymptomatic; lasts lifelong in ~70-80% |
| Chronic phase frequency | ~20-30% of infected individuals |
Sources: Goldman-Cecil Medicine (25th ed.), Braunwald's Heart Disease, Rosen's Emergency Medicine, Sleisenger & Fordtran's GI and Liver Disease - all via the medical textbook library. Recent systematic reviews via PubMed (2023-2024).
This is a shared conversation. Sign in to Orris to start your own chat.