Aortic stenosis in detail
Reading File
Finding Sources
Searching PubMed
"aortic stenosis"[MeSH Terms] AND management
Reading File
Reading File
Reading File
Finding Sources
Reading File
Reading File
Finding Sources
Reading File
Reading File
Reading File
Reading File
Reading File
Reading File
Loading Image
Loading Image
Finding Sources
Reading File
Reading File
Reading File
I now have comprehensive, authoritative content from multiple major textbooks. Let me compile the full detailed response.
Aortic Stenosis - Comprehensive Review
1. Definition and Epidemiology
Aortic stenosis (AS) is obstruction to left ventricular outflow at the level of the aortic valve, resulting in a pressure gradient between the left ventricle (LV) and the aorta during systole. It is the most common valvular heart disease requiring intervention in the developed world.
- Present in ~15% of adults ≥65 years old
- Severe AS (valve area <1 cm²) affects ~2% of those ≥65 years
- Prevalence is 3% in patients ≥75 years old
- Calcific AS rarely becomes clinically severe before age 70 in those with a tricuspid valve
(Braunwald's Heart Disease, p. 697; Symptom to Diagnosis, p. 9318)
2. Etiology
Three main causes, in order of current frequency in developed nations:
| Cause | Features |
|---|---|
| Calcific (senile) degenerative | Most common in Western countries; calcification of a normal tricuspid valve; typically presents age 70-85 |
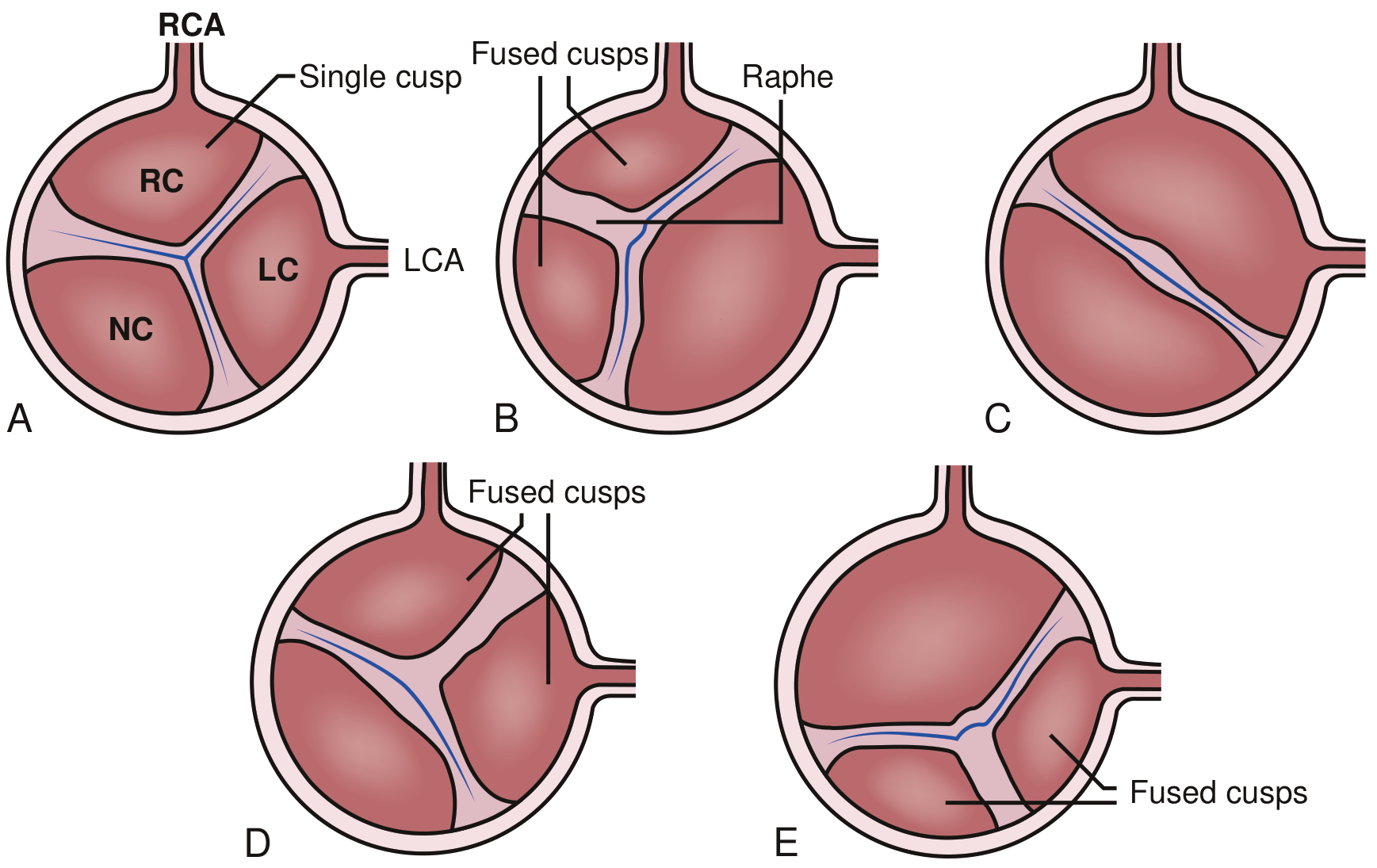
| Congenital bicuspid aortic valve (BAV) | 1-2% of the population; severe AS develops in ~66%; presents 1-2 decades earlier (age 50-60); associated with aortopathy (dilation, dissection risk) |
| Rheumatic | Commissural fusion + cusp calcification; almost always co-exists with mitral valve disease; decreasing in developed countries |
Subvalvar (e.g., HOCM, discrete fibromuscular ridge) and supravalvar (Williams syndrome) forms exist but are less common.
3. Pathophysiology
3a. Molecular Mechanisms of Calcification
Calcific AS is not simply "wear and tear." It is driven by active biological processes:
- Lipid infiltration and oxidative stress initiate the cascade - analogous to atherosclerosis
- Inflammatory cells are recruited; cytokines are elaborated
- Valve interstitial cells (VICs) undergo osteogenic reprogramming
- Mineralization of the extracellular matrix progresses (fibrocalcific remodeling)
- Genetic factors contribute: Lipoprotein(a) [Lp(a)] is the strongest genetic association (SNP in Lp(a) associated with AS, HR 1.68). Other polymorphisms: vitamin D receptor, IL-10, TGF-β receptor, ApoE4
(Braunwald's Heart Disease, p. 697)
3b. Hemodynamic Consequences
As valve obstruction develops, a pressure gradient builds between the LV and aorta:
- LV pressure overload → concentric LV hypertrophy (LVH) as the compensatory response
- LVH maintains wall stress (by Laplace's law: stress = P × r / 2h) and preserves ejection fraction for years-decades
- However, LVH causes:
- Increased LV stiffness → diastolic dysfunction (impaired early filling, LA dependence)
- Increased myocardial oxygen demand with reduced coronary flow reserve → angina even without obstructive CAD
- As stenosis worsens, LV cannot sustain adequate output → symptoms emerge
- Eventually, LV decompensates → systolic dysfunction, pulmonary hypertension, right heart failure
The nozzle effect (Guyton physiology): Blood jets through the small orifice at very high velocity, creating severe turbulence in the aortic root - this is the mechanism of the systolic murmur and post-stenotic dilatation.
(Guyton & Hall, p. 291)
4. Classification of Severity (ACC/AHA Stages)
| Stage | Description | Peak Jet Velocity | Mean Gradient | AVA |
|---|---|---|---|---|
| A | At risk | Normal | Normal | Normal |
| B | Progressive (mild-moderate) | 2.0-3.9 m/s | <40 mmHg | >1.0 cm² |
| C1 | Asymptomatic severe, normal EF | ≥4.0 m/s | ≥40 mmHg | ≤1.0 cm² |
| C2 | Asymptomatic severe, reduced EF (<50%) | ≥4.0 m/s | ≥40 mmHg | ≤1.0 cm² |
| D1 | Symptomatic severe, high gradient | ≥4.0 m/s | ≥40 mmHg | ≤1.0 cm² |
| D2 | Symptomatic severe, low flow/low gradient, reduced EF | <4.0 m/s | <40 mmHg | ≤1.0 cm² |
| D3 | Symptomatic severe, low gradient, normal EF (paradoxical) | <4.0 m/s | <40 mmHg | ≤1.0 cm² |
Classic severe AS criteria: Peak jet velocity ≥4.0 m/sec or mean gradient ≥40 mm Hg, usually with AVA ≤1.0 cm² (or ≤0.6 cm²/m² body surface area).
Important: Over one-third of patients with AVA ≤1.0 cm² have a peak velocity <4 m/s or mean gradient <40 mmHg - the "low-flow, low-gradient" problem. These patients need careful distinction from truly moderate AS.
(Braunwald's Heart Disease, p. 706)
Progression rate (Stage B):
- Hemodynamic progression occurs in nearly all patients once even mild obstruction is present
- Interval from mild to severe: 5-10+ years (highly variable)
- Faster progression with: older age, heavier calcification, renal insufficiency, hypertension, obesity, metabolic syndrome, smoking, hyperlipidemia, elevated Lp(a)
5. Clinical Features
5a. The Classic Triad (Cardinal Symptoms)
These appear when AS becomes severe. Prognosis without valve replacement is dismal once symptoms develop:
| Symptom | Mechanism | Median Survival Without Intervention |
|---|---|---|
| Angina | Mismatch between O₂ supply and hypertrophied myocardium demand; subendocardial ischemia | 5 years (50% mortality) |
| Syncope | Inability to increase cardiac output with exertion; vasodepressor reflex from baroreceptor activation | 3 years (50% mortality) |
| Dyspnea / HF | Elevated LV filling pressure; pulmonary venous hypertension; reduced cardiac reserve | 2 years (50% mortality) |
The most common presenting symptoms are reduced exercise tolerance and exertional dyspnea - the dramatic triad is a late presentation.
(Symptom to Diagnosis, p. 9340-9344)
5b. Other Manifestations
- Atrial fibrillation - poorly tolerated because the non-compliant LV is dependent on atrial kick for filling
- Acquired von Willebrand syndrome - mechanical disruption of large vWF multimers by turbulent flow; occurs in 67-92% of severe AS; causes a bleeding tendency (Heyde syndrome when associated with GI angiodysplasia)
- Systemic embolization (calcific emboli, rarely)
(Miller's Anesthesia, p. 3908-3909)
6. Physical Examination
| Finding | Significance |
|---|---|
| Harsh, crescendo-decrescendo systolic ejection murmur | Heard best at right 2nd intercostal space, radiates to carotids; the hallmark |
| Pulsus parvus et tardus | Small, slowly rising, delayed carotid upstroke (reduced stroke volume + slow ejection); less reliable in elderly due to arterial stiffness |
| Diminished or absent A2 | Immobile, calcified valve cannot close audibly |
| Paradoxical splitting of S2 | Prolonged LV ejection delays A2 beyond P2 |
| S4 gallop | Hypertrophied, non-compliant LV |
| Sustained, non-displaced apex beat | Concentric LVH (vs. volume overload which displaces apex) |
| Radiation to right clavicle | Absence of radiation to right clavicle has LR- of 0.1 for ruling out AS |
Note: The classic carotid upstroke delay (pulsus parvus et tardus) is often absent in elderly patients with arterial stiffening, making this sign unreliable in the population most commonly affected.
7. Investigations
7a. Echocardiography (First-line, Gold Standard)
Transthoracic Echo (TTE) with Doppler is the cornerstone of assessment:
- Valve morphology: leaflet number, thickening, calcification, mobility
- Quantification:
- Peak jet velocity (Vmax)
- Mean pressure gradient - by modified Bernoulli equation: ΔP = 4v²
- Aortic valve area (AVA) by continuity equation: AVA = SV / VTI_AV, where SV = CSA_LVOT × VTI_LVOT
- This is based on conservation of flow: flow in LVOT = flow through AV (in absence of shunts)
- LV size and EF - mandatory; reduced EF alters interpretation
- LV wall thickness - degree of hypertrophy
- Doppler velocity ratio (VTI_LVOT/VTI_AV): <0.25 suggests severe AS
TEE with 3D planimetry: Overcomes acoustic limitations; allows direct measurement of anatomical orifice area at mid-systole.
Stress echocardiography (dobutamine): Used in low-flow, low-gradient AS to distinguish true severe AS (valve area stays ≤1 cm² as flow increases) from pseudo-severe AS (valve area normalizes).
(Grainger & Allison Radiology, p. 1711-1712; Textbook of Clinical Echocardiography)
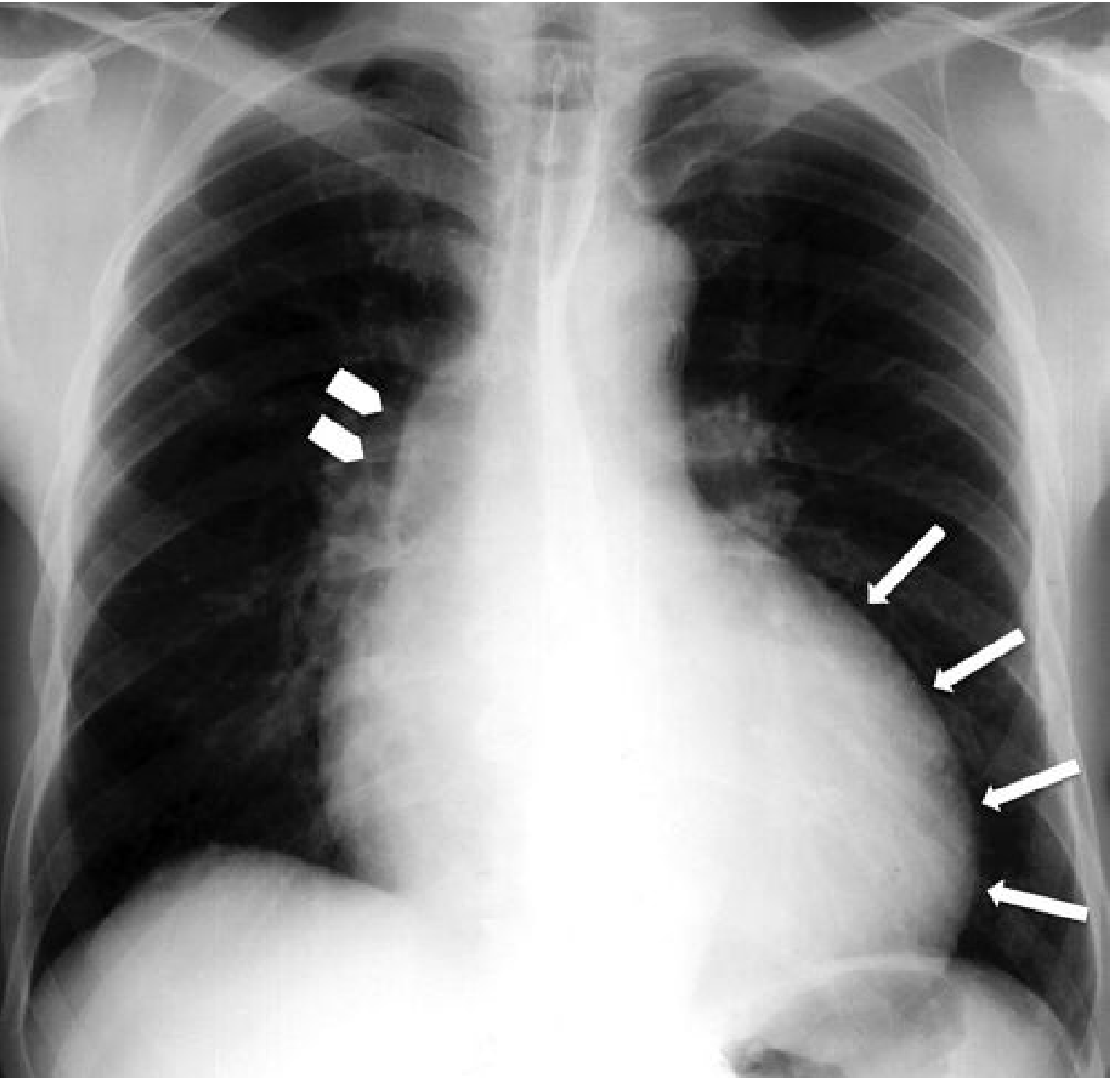
7b. Chest X-Ray
- Rounded cardiac apex - LVH (concentric pattern)
- Post-stenotic dilatation of ascending aorta (prominent first right cardiac arch)
- Aortic valve calcification - better seen on lateral view
- In late disease: pulmonary venous congestion
7c. ECG
- LVH (increased voltage + repolarization changes/strain pattern)
- Left axis deviation
- Left bundle branch block
- ST depression / T-wave inversion in lateral leads (strain pattern)
7d. Cardiac CT
- Aortic valve calcium score (AVC): Useful adjunct when echo findings are discordant; high calcium burden confirms true severe AS
- CT angiography: Aortic annulus sizing before TAVR; assessment of coronary anatomy; vascular access planning
7e. Cardiac Catheterization
- Now reserved for cases where non-invasive assessment is inconclusive
- Direct measurement of transvalvular gradient (Gorlin formula for AVA)
- Coronary angiography when PCI or CABG may be planned alongside valve surgery
7f. BNP / NT-proBNP
- Elevated levels reflect LV pressure overload and wall stress
- Useful for detecting subclinical LV decompensation in asymptomatic patients
- Elevated BNP predicts faster progression and adverse outcomes
8. Low-Flow, Low-Gradient AS (Special Situations)
This is a common clinical challenge (~40% of severe AS in elderly):
Type 1 - Classic low-flow, low-gradient (reduced EF)
- AVA ≤1.0 cm², mean gradient <40 mmHg, LVEF <50%, LV stroke volume index <35 mL/m²
- Distinguish true severe AS from "pseudo-severe" using dobutamine stress echo
- More common in men with dilated cardiomyopathy
Type 2 - Paradoxical low-flow, low-gradient (preserved EF)
- AVA ≤1.0 cm², mean gradient <40 mmHg, LVEF ≥50%, LV stroke volume index <35 mL/m²
- More common in women with small, hypertrophied LV cavities and AF
- High aortic valve calcium score on CT helps confirm true severity
In both patterns, all-cause long-term mortality is similar to high-flow, high-gradient AS with medical treatment; both benefit from AVR (except the high-flow/low-gradient subset which does not appear to benefit).
(Braunwald's Heart Disease, p. 1036)
9. Management
9a. Medical Management
There is no proven medical therapy that slows progression or replaces valve intervention. Management focuses on:
- Treat comorbidities: Hypertension, diabetes, dyslipidemia
- Statins: Despite initial observational promise, randomized trials (SALTIRE, SEAS) showed no benefit in slowing AS progression. Still indicated for concurrent atherosclerotic disease
- Avoid: Vasodilators (nitrates, ACE inhibitors, ARBs) in severe AS - can precipitate hypotension by reducing preload in a preload-dependent, fixed-output state
- Diuretics: Used cautiously for pulmonary congestion - avoid excessive preload reduction
- Beta-blockers: Used carefully; the hypertrophied LV needs adequate heart rate for filling
- AF management: Rapid AF extremely poorly tolerated; rate/rhythm control is important
- Endocarditis prophylaxis: No longer routinely recommended per current guidelines
- Lp(a)-lowering (e.g., RNA-targeted therapies): Under active investigation as disease-modifying treatment
9b. Valve Intervention - Indications
Per the 2020 ACC/AHA Guideline for Valvular Heart Disease:
Class I (Recommended):
- Symptomatic severe AS (Stage D) - AVR (surgical or TAVR) without delay
- Asymptomatic severe AS (Stage C2) with LVEF <50%
- Asymptomatic severe AS (Stage C1) undergoing other cardiac surgery
Class IIa:
- Asymptomatic very severe AS (Vmax ≥5 m/s) with low surgical risk
- Asymptomatic severe AS with rapid progression (Vmax increase ≥0.3 m/s/year) and low surgical risk
Timing controversy: The ongoing EARLY TAVR trial (USA) is addressing whether earlier intervention in asymptomatic severe AS with negative exercise tests improves outcomes.
9c. Surgical Aortic Valve Replacement (SAVR)
- Gold standard for younger, lower-risk patients
- Tissue (bioprosthetic) valve preferred in older adults (avoids anticoagulation; durability adequate for remaining lifespan); degenerates more slowly in older patients
- Mechanical valve considered in younger patients (<65 years) willing to accept lifelong anticoagulation
- Operative mortality: <2% at experienced centers for low-risk patients; higher with LV dysfunction
9d. Transcatheter Aortic Valve Replacement (TAVR)
TAVR has transformed management, providing an alternative to open surgery across the risk spectrum:
Key trial data:
- PARTNER trial (inoperable patients): 1-year mortality TAVR 30% vs. medical therapy 50%
- High/intermediate surgical risk: TAVR showed similar 30-day and 1-year survival vs. SAVR
- Low-risk patients (PARTNER 3, Evolut Low Risk) (mean age 73): Composite risk of death/stroke/hospitalization at 1 year was significantly lower with TAVR (8.5% vs. 15.1%), shorter hospital stay, less new-onset AF
TAVR recommended (per 2020 ACC/AHA guidelines) for:
- Symptomatic severe AS of any age with high or prohibitive surgical risk, if predicted survival >12 months with acceptable quality of life
- Patients >80 years or those with life expectancy <10 years
- Ages 65-80: Either SAVR or TAVR after shared decision-making
TAVR risks (compared to SAVR):
- Higher: stroke, vascular complications, permanent pacemaker implantation, paravalvular leak
- Lower: new-onset AF, shorter hospital stay
Antithrombotic after TAVR: Daily aspirin 75-100 mg recommended; debate ongoing regarding dual antiplatelet or anticoagulation.
(Braunwald's Heart Disease, p. 1036-1037)
9e. Balloon Aortic Valvuloplasty (BAV)
- Percutaneous balloon dilation of the aortic valve
- Very high restenosis rate; not a definitive treatment
- Used as a bridge to TAVR/SAVR in hemodynamically unstable patients or as palliation in those ineligible for any definitive intervention
10. Asymptomatic Severe AS - Surveillance
Asymptomatic severe AS (Stage C) requires close surveillance:
- Serial Doppler echocardiography: every 6-12 months for severe AS
- Exercise stress testing: Recommended in apparently asymptomatic patients to unmask true symptoms; ~50% develop symptoms or abnormal findings on exercise testing
- BNP/NT-proBNP: Monitoring for subclinical LV stress
- The strongest predictor of symptom development is the severity of aortic valve calcification and the initial hemodynamic gradient
11. Special Situations
Perioperative/Anesthesia Considerations
- Moderate-to-severe AS is associated with increased risk of perioperative cardiovascular complications
- Asymptomatic severe AS can proceed to major elective noncardiac surgery with appropriate hemodynamic monitoring and preserved ventricular function
- Symptomatic severe AS: Valve replacement should be considered before elective noncardiac surgery
- Hemodynamic goals during anesthesia: Maintain adequate preload, avoid tachycardia (reduces diastolic filling time in stiff LV), avoid hypotension, maintain sinus rhythm
(Miller's Anesthesia, p. 3908)
Pregnancy (Maternal-Fetal Medicine)
- Severe AS poorly tolerated in pregnancy (fixed obstruction cannot accommodate the normal 50% increase in cardiac output)
- Management requires multidisciplinary team; balloon valvuloplasty or even SAVR may be needed
Aortic Stenosis with Concomitant Amyloidosis
- Increasingly recognized: transthyretin amyloidosis (ATTR) co-exists with AS in ~15% of TAVR patients
- Apical sparing pattern on LV strain imaging, bone scintigraphy (Perugini grade 2+), and CMR (transmural late gadolinium enhancement) are diagnostic
- Carries worse prognosis and requires specific ATTR treatment (tafamidis)
(Braunwald's Heart Disease, p. 706)
12. Prognosis Summary
- Asymptomatic severe AS: Annual mortality ~1-2%; event rate ~10% per year for developing symptoms
- Symptomatic severe AS without intervention:
- Angina: ~50% 5-year mortality
- Syncope: ~50% 3-year mortality
- Heart failure/dyspnea: ~50% 2-year mortality
- After successful AVR or TAVR: Survival approximates age-matched controls; dramatic symptom improvement and quality of life benefit
Sources:
- Braunwald's Heart Disease: A Textbook of Cardiovascular Medicine, 12th ed. - Chapters 72-73 (Calcific AS, TAVR)
- Guyton and Hall Textbook of Medical Physiology, 14th ed. - p. 291
- Symptom to Diagnosis: An Evidence-Based Guide, 4th ed. - p. 9318-9350
- Grainger & Allison's Diagnostic Radiology, 6th ed. - p. 1700-1768
- Miller's Anesthesia, 10th ed. - p. 3908-3909
- Textbook of Clinical Echocardiography - Chapters on Valvular Stenosis Assessment
This is a shared conversation. Sign in to Orris to start your own chat.