By doing ct chest scan the doctor gets to know about the patient smokes or not
Reading File
Searching the Web
CT chest findings that indicate smoking history radiological signs
Finding Sources
Finding Sources
Reading File
Reading File
Loading Image
Loading Image
Finding Sources
Here is a thorough answer based on authoritative radiology and pulmonary medicine textbooks:
What a CT Chest Scan Reveals About Smoking
Yes - a radiologist can often tell a patient smokes (or has smoked) from CT findings alone, even before asking. The scan does not show nicotine directly, but it shows the structural damage tobacco smoke causes. These findings are characteristic enough that experienced radiologists describe them as "smoker's lungs."
Key CT Findings That Indicate Smoking
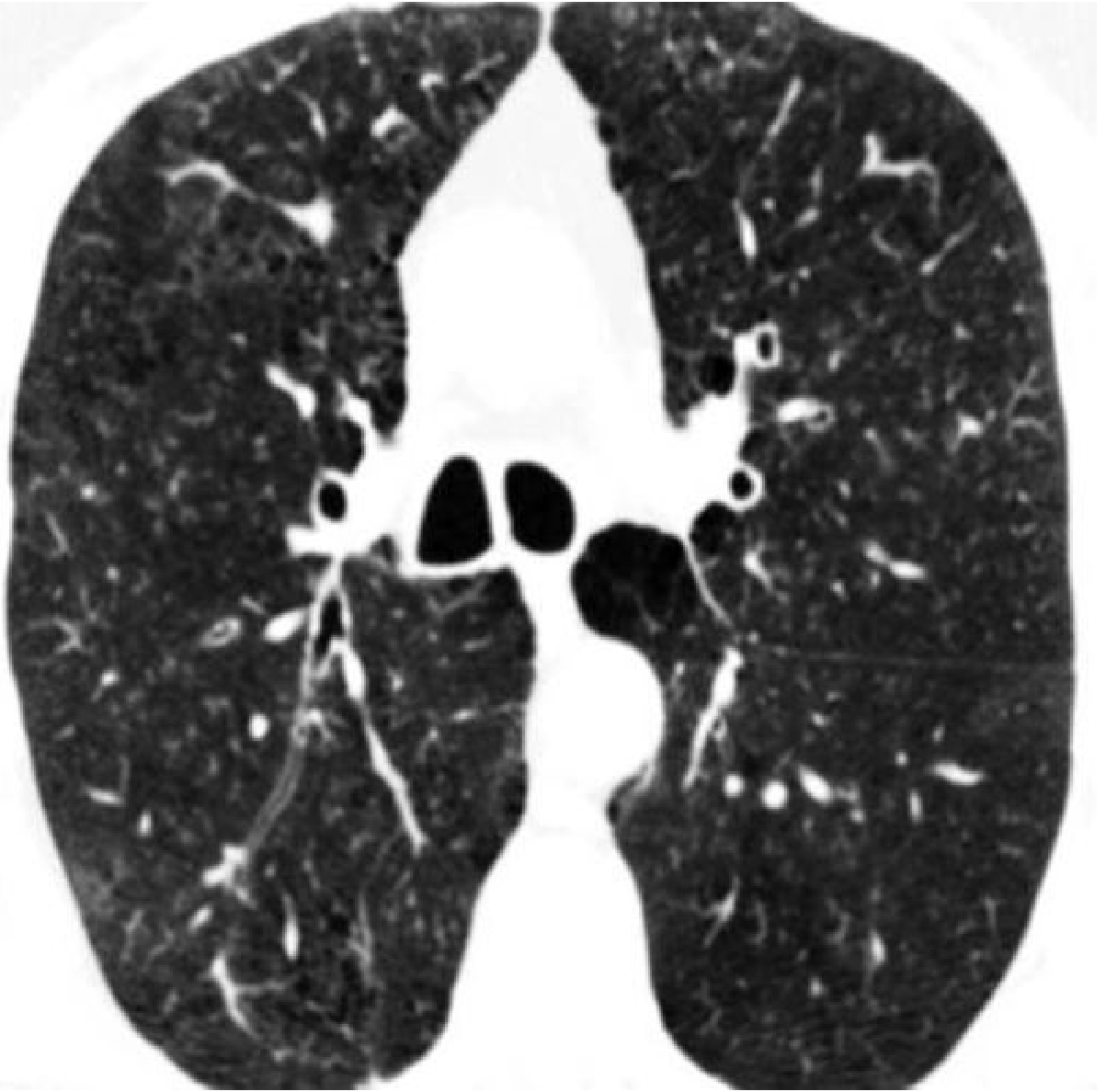
1. Centrilobular Emphysema (most specific finding)
This is the hallmark. Tobacco smoke destroys the walls of alveoli around the central part of the secondary pulmonary lobule, creating small, round, air-filled "holes" (areas of very low attenuation) scattered throughout the lung parenchyma - classically upper-lobe predominant. CT is far more sensitive for this than plain chest X-ray.
2. Paraseptal Emphysema
Large, cyst-like black spaces (bullae) along the pleural margins and interlobar fissures. These are aligned in rows near the pleura and are strongly associated with smoking.
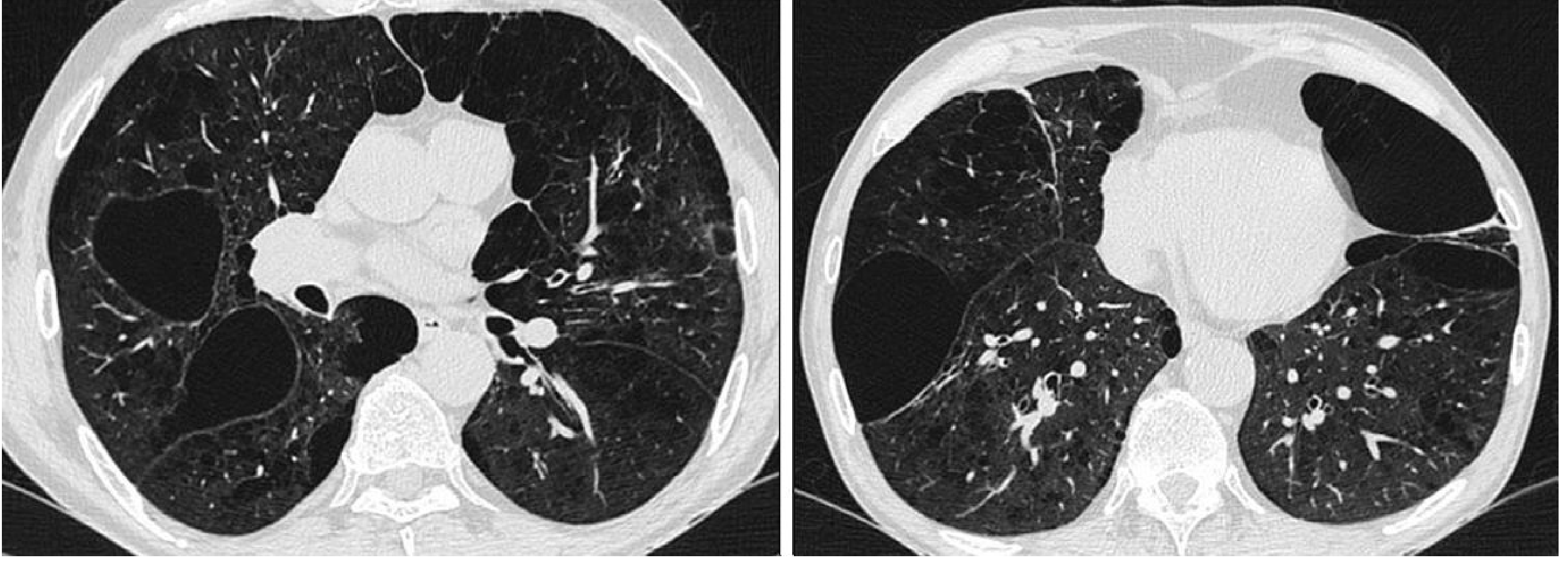
3. Bronchial Wall Thickening
Chronic bronchitis from smoking causes thickening of the bronchial walls. On CT this is visible as a "ring" sign where the airway wall appears disproportionately thick compared to its diameter (increased wall-to-lumen ratio).
4. Centrilobular Ground-Glass Nodules
These are subtle, ill-defined hazy nodular opacities in the upper lobes, representing "smoker's bronchiolitis" (respiratory bronchiolitis). Pathologically, these reflect accumulation of pigmented macrophages in the small airways in response to tobacco smoke. They may actually improve or disappear after smoking cessation.
5. Air Trapping (Gas Trapping)
On expiratory CT images, areas of lung that fail to increase in attenuation (stay dark) indicate obstructive small airway disease - caused by mucus plugging and inflammation from smoking.
6. Mosaic Attenuation Pattern
Patchy areas of different lung density (some darker, some lighter) reflect heterogeneous airflow obstruction across lung segments.
7. Smoking-Related ILD Patterns
- RB-ILD (Respiratory Bronchiolitis-ILD): upper lobe centrilobular ground-glass nodules, almost exclusively in smokers
- DIP (Desquamative Interstitial Pneumonia): diffuse ground-glass opacity, strongly linked to smoking
- Combined Pulmonary Fibrosis and Emphysema (CPFE): upper lobe emphysema + lower lobe fibrosis - a distinct smoking-related pattern
Summary Table
| CT Finding | Mechanism | Location |
|---|---|---|
| Centrilobular emphysema | Alveolar wall destruction | Upper lobes, central lobule |
| Paraseptal emphysema / Bullae | Peripheral alveolar destruction | Subpleural, along fissures |
| Bronchial wall thickening | Chronic bronchitis / mucus gland hypertrophy | Central airways |
| Centrilobular ground-glass nodules | Pigmented macrophage accumulation | Upper lobes |
| Air trapping (expiratory CT) | Small airway obstruction | Patchy, bilateral |
| Mosaic attenuation | Heterogeneous airflow obstruction | Diffuse |
Important Nuances
- CT findings suggest smoking history but are not 100% diagnostic - some changes overlap with other conditions (e.g., hypersensitivity pneumonitis can also cause centrilobular nodules)
- Severity correlates with pack-years - mild centrilobular emphysema can appear even in moderate smokers
- Some lesions (like RB nodules) can regress after quitting - so a former smoker may have fewer findings than a current smoker of the same pack-year history
- CT can detect these changes even when chest X-ray is normal and even before lung function tests show abnormality - making it the most sensitive non-invasive tool for smoking-related lung damage
Sources: Fishman's Pulmonary Diseases and Disorders, p. 969; Grainger & Allison's Diagnostic Radiology, pp. 171-172; RSNA lung abnormality progression in smokers
This is a shared conversation. Sign in to Orris to start your own chat.