65 yrs old male htn, on telmisartan chlortalidone, and taking Aspirin. Came for regular checkup up and found to have 5-8 rbcs in the urine. 6 months ago done urine also had same. USG done 6 months had mild bph. Should we evaluate him?
Reading File
Finding Sources
Searching PubMed
asymptomatic microscopic hematuria evaluation guidelines
Searching the Web
asymptomatic microscopic hematuria evaluation guidelines 2023 2024 AUA
Reading File
Reading File
Reading Web Page
microscopic hematuria risk stratification 2025 AUA guidelines
Reading File
Searching PubMed
microscopic hematuria aspirin anticoagulant false positive
Loading Image
I have everything needed for a comprehensive, clinically actionable answer.
Yes — This Patient Requires Evaluation
Short answer: Persistent microscopic hematuria (MH) on two separate urinalyses 6 months apart in a 65-year-old male warrants full urologic evaluation. The hematuria is not explained by his medications (aspirin is not a recognized cause of true microscopic hematuria — it may unmask pre-existing disease, not cause false positives on microscopy), and no confirmed transient cause has been documented.
Why Evaluate?
Key Risk Factors in This Patient
| Factor | This Patient | Significance |
|---|---|---|
| Age | 65 years | >40 years = high-risk |
| Sex | Male | Higher baseline risk |
| Persistent MH | Two occasions, 6 months apart | Confirms persistence, not transient |
| RBC count | 5-8 RBCs/HPF | Threshold ≥3 RBCs/HPF meets criteria |
| BPH | Mild on USG | Does NOT exclude urothelial malignancy |
| HTN | Present | Raises nephrologic concern as well |
Per the textbook data, in males over 40 years, microscopic hematuria carries an 8% risk of malignancy on evaluation (predominantly bladder cancer) — Comprehensive Clinical Nephrology, 7th Ed.
The 2025 AUA/SUFU Risk Stratification (Most Current Guidelines)
This patient fits Intermediate–High Risk:
High-risk criteria include:
- Male, age >40 years ✅
- Smoking history (ask — important)
-
25 RBCs/HPF (he has 5-8, which is below this threshold)
- History of gross hematuria (ask)
Intermediate-risk criteria include:
- 11–25 RBCs/HPF, or
- Low-risk patient with persistent MH on repeat UA (3-25 RBCs/HPF on a repeat) ✅ — this applies here
A patient who was initially "low-risk" but has MH confirmed on a repeat urinalysis is reclassified as intermediate or high-risk under the 2025 AUA guideline, and should undergo cystoscopy and upper tract imaging. (2025 AUA Microhematuria Guideline)
First: Exclude Nephrologic Causes
Before urologic workup, assess for glomerular/renal parenchymal disease:
- Urinalysis microscopy: Are RBCs dysmorphic? Any RBC casts?
- Urine protein: Significant proteinuria (>0.3 g/24h) → refer nephrology
- Serum creatinine / eGFR: Reduced GFR → renal disease workup
- Blood pressure: He already has HTN on treatment
If dysmorphic RBCs, RBC casts, proteinuria, or reduced eGFR → nephrology referral for possible glomerulonephritis.
If isomorphic RBCs, no casts, no significant proteinuria → urologic evaluation proceeds.
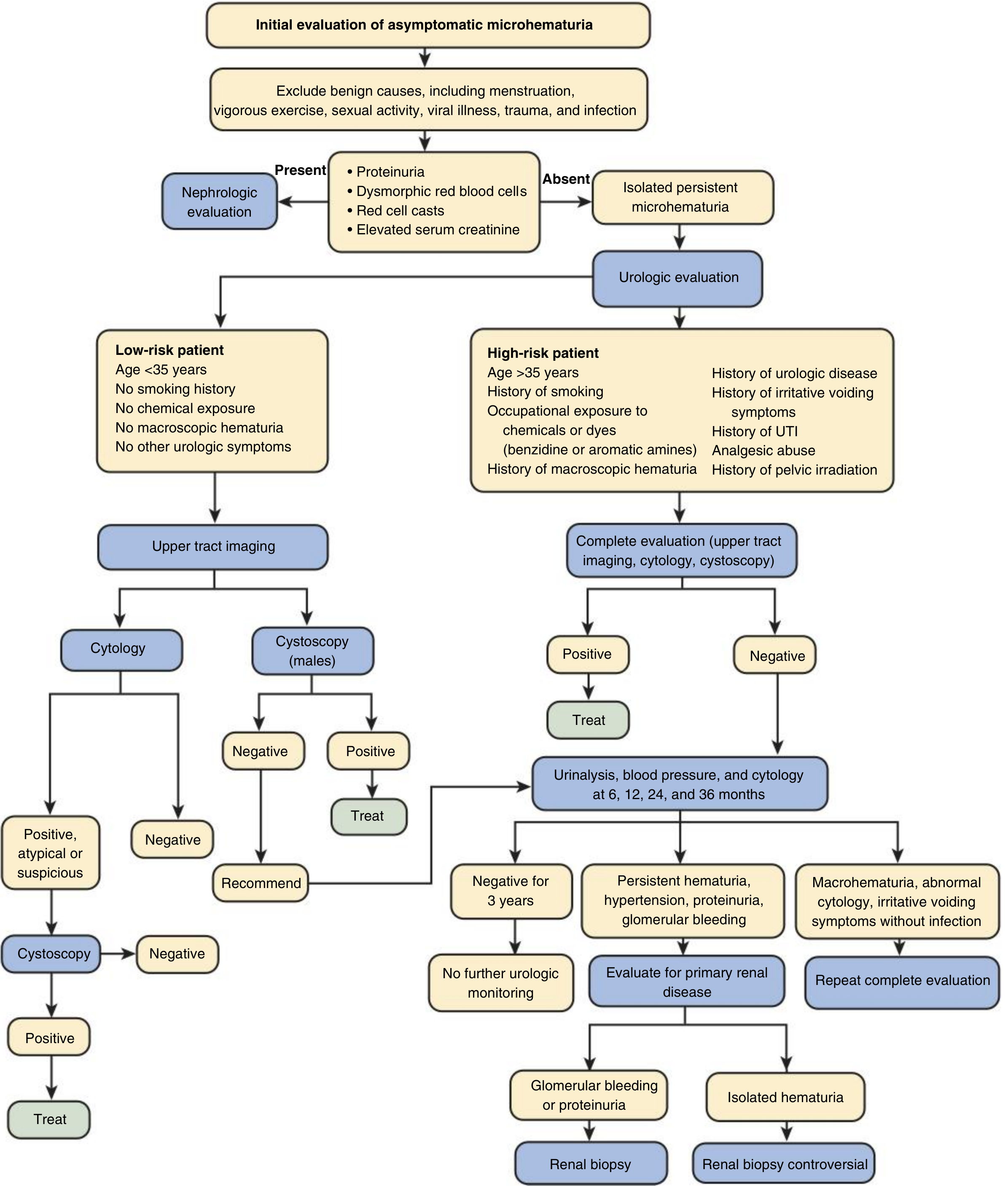
Recommended Workup (Urologic Pathway)
1. Repeat urinalysis + urine microscopy (if not done recently)
- Confirm 5-8 RBCs/HPF with fresh mid-stream sample
- Exclude UTI (urine culture if any pyuria)
- Assess RBC morphology
2. Upper Tract Imaging
- CT Urography (preferred) — highest sensitivity/specificity for renal masses, urothelial lesions, stones
- If CT unavailable or contraindicated (e.g., poor renal function): Renal ultrasound + IVP, or MR Urography
- Note: BPH on prior USG is insufficient — it doesn't image the upper tracts adequately, and does not evaluate for urothelial malignancy
3. Cystoscopy
- Indicated for intermediate/high-risk patients
- At 65, male, with persistent MH → cystoscopy is recommended
- Evaluates for bladder cancer, which is the most common malignancy found (~5% of microscopic hematuria cases in clinic hematuria series)
4. Urine cytology — not routinely recommended by 2025 AUA guidelines unless high clinical suspicion of high-grade urothelial carcinoma
5. Labs
- Serum creatinine / eGFR
- Urine protein:creatinine ratio
- BP check
What About Aspirin and Telmisartan/Chlorthalidone?
- Aspirin: Does not cause microscopic hematuria per se. It does not produce false-positive results on urine microscopy. It may unmask pre-existing urinary tract pathology by promoting bleeding, which makes investigation even more important.
- Telmisartan + Chlorthalidone: Not a cause of hematuria. Chlorthalidone (thiazide-like diuretic) may actually reduce hypercalciuria but does not cause hematuria.
- Do not attribute hematuria to medications — this is a dangerous assumption that can delay diagnosis of bladder or renal cancer.
What About BPH?
Mild BPH can cause microscopic hematuria, but it is a diagnosis of exclusion. BPH should be attributed as the cause only after malignancy and other significant pathology have been excluded. The prior ultrasound showing mild BPH does not replace the need for upper tract imaging or cystoscopy.
Summary: Action Plan
- ✅ Confirm hematuria is true (repeat fresh mid-stream UA + microscopy)
- ✅ Exclude UTI
- ✅ Assess RBC morphology, eGFR, urine protein → if abnormal, refer nephrology
- ✅ CT Urography (upper tract imaging)
- ✅ Cystoscopy (given age, sex, persistent hematuria)
- ✅ Review smoking history — if positive, elevates to high-risk
Bottom line: Persistent microscopic hematuria in a 65-year-old male is a significant finding. BPH and aspirin do not explain it away. Full urologic evaluation with upper tract imaging and cystoscopy is warranted per 2025 AUA/SUFU guidelines.
— Comprehensive Clinical Nephrology, 7th Ed., p. 883–884; Campbell-Walsh-Wein Urology; AUA 2025 Microhematuria Guideline
This is a shared conversation. Sign in to Orris to start your own chat.