Classify benzodiazepine
Reading File
Finding Sources
Finding Sources
Finding Sources
Finding Sources
Reading File
Reading File
Reading File
Finding Sources
Reading File
Reading File
Loading Image
I now have everything needed for a thorough classification answer. Here it is:
Classification of Benzodiazepines
Benzodiazepines are a group of CNS depressants that act as positive allosteric modulators of the GABA-A receptor, increasing the frequency of chloride channel opening in response to GABA. They can be classified by several criteria.
1. Classification by Duration of Action (Half-life)
This is the most clinically important classification:
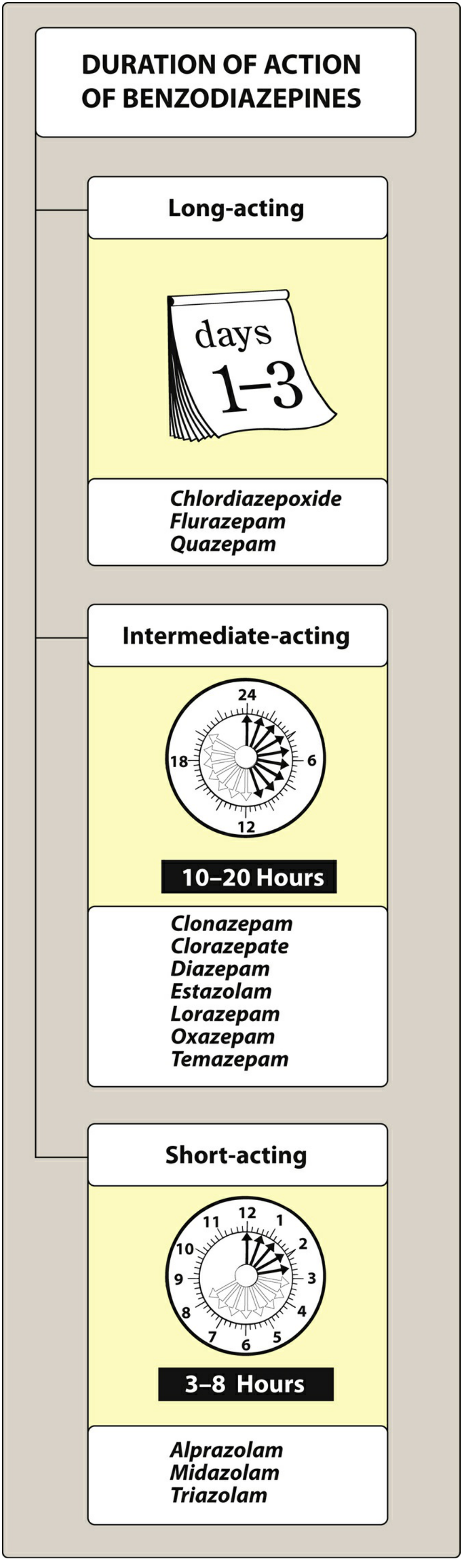
Figure 16.4 - Lippincott Illustrated Reviews: Pharmacology
| Category | Half-life | Examples | Clinical Use |
|---|---|---|---|
| Ultra-short-acting | < 1-4 hrs | Midazolam, Triazolam | Pre-anaesthesia, procedural sedation |
| Short-acting | 3-8 hrs | Alprazolam, Triazolam | Panic disorder, acute anxiety |
| Intermediate-acting | 10-20 hrs | Clonazepam, Clorazepate, Diazepam, Estazolam, Lorazepam, Oxazepam, Temazepam | Anxiety, insomnia |
| Long-acting | 1-3 days (t½ > 24 hrs) | Chlordiazepoxide, Flurazepam, Quazepam | Alcohol withdrawal, daytime anxiety |
Longer-acting agents tend to form pharmacologically active metabolites (e.g., diazepam forms desmethyldiazepam/nordiazepam), which extend duration further. Short-acting agents such as triazolam produce more abrupt and severe withdrawal reactions on discontinuation.
- Lippincott Illustrated Reviews: Pharmacology, p. 552-553
2. Classification by Primary Therapeutic Use
| Use | Drugs of Choice |
|---|---|
| Anxiety (GAD, panic disorder) | Alprazolam, Lorazepam, Diazepam, Chlordiazepoxide |
| Insomnia (hypnotic) | Temazepam, Flurazepam, Triazolam, Estazolam, Quazepam |
| Anticonvulsant / Seizures | Clonazepam, Diazepam (IV), Lorazepam (IV) |
| Pre-anaesthetic sedation / procedural | Midazolam |
| Alcohol withdrawal | Chlordiazepoxide, Diazepam, Lorazepam |
| Muscle relaxant | Diazepam |
| Status epilepticus | Lorazepam (first-line IV), Diazepam |
3. Classification by Chemical Structure
All benzodiazepines share a core benzene ring fused to a 1,4-diazepine ring, but differ in side chain substitutions:
| Subtype | Features | Examples |
|---|---|---|
| 2-keto compounds | Classic structure; long-acting | Diazepam, Chlordiazepoxide, Clorazepate, Flurazepam, Halazepam |
| 3-hydroxy compounds | Hydroxyl at C-3; directly glucuronidated (no active metabolites) | Lorazepam, Oxazepam, Temazepam |
| Triazolo compounds | Triazole ring fused; high potency, short-acting | Alprazolam, Triazolam, Estazolam |
| Imidazo compounds | Imidazole ring; water-soluble at low pH | Midazolam |
| Nitro compounds | Nitro group at C-7 | Clonazepam, Nitrazepam |
4. Classification by Metabolism
| Category | Features | Examples |
|---|---|---|
| Phase I + II metabolism | Hepatic oxidation (CYP3A4/CYP2C19) then glucuronidation; form active metabolites; accumulate in liver/renal disease | Diazepam, Chlordiazepoxide, Flurazepam |
| Phase II only (LOT drugs) | Direct glucuronidation only; no active metabolites; safer in hepatic/renal impairment, elderly, pregnancy | Lorazepam, Oxazepam, Tamazepam |
The "LOT" drugs (Lorazepam, Oxazepam, Temazepam) are preferred in hepatic dysfunction and the elderly because they bypass CYP-mediated phase I metabolism entirely.
- Lippincott Illustrated Reviews: Pharmacology, p. 553
5. Classification by Potency
| Potency | Examples |
|---|---|
| High potency | Alprazolam, Clonazepam, Lorazepam, Triazolam |
| Intermediate potency | Oxazepam, Temazepam |
| Low potency | Chlordiazepoxide, Diazepam, Flurazepam |
6. Four-Category Classification (Tietz / Clinical Labs)
The Tietz classification based on elimination half-life divides benzodiazepines into:
- Ultra-short-acting (t½ < 4 hrs) - Midazolam
- Short-acting (t½ < 6 hrs) - Triazolam
- Intermediate-acting (t½ 6-24 hrs) - Alprazolam, Lorazepam, Oxazepam
- Long-acting (t½ > 24 hrs) - Diazepam, Chlordiazepoxide, Clonazepam, Flurazepam
- Tietz Textbook of Laboratory Medicine, 7th Edition
Key Clinical Pearls
-
All benzodiazepines are Schedule IV controlled substances (high abuse potential; physical and psychological dependence)
-
They cross the placental barrier and are excreted in breast milk - avoid in pregnancy
-
CYP3A4 inhibitors (erythromycin, ritonavir, ketoconazole, grapefruit juice) significantly increase levels of most benzodiazepines
-
Antagonist: Flumazenil (competitive GABA-A benzodiazepine site antagonist) reverses sedation but has a short half-life
-
Withdrawal risk is greatest with short-acting, high-potency agents (e.g., alprazolam, triazolam)
-
Lippincott Illustrated Reviews: Pharmacology, pp. 546-558
-
Tietz Textbook of Laboratory Medicine, 7th Edition, pp. 4096-4115
No I want classification on based on pharmacological
Finding Sources
Finding Sources
Reading File
Reading File
Reading File
Finding Sources
Finding Sources
Reading File
Reading File
Excellent. I now have comprehensive content from multiple authoritative textbooks. Here is the complete pharmacological classification:
Classification of Benzodiazepines - Based on Pharmacological Actions
All benzodiazepines share the same core mechanism - they are positive allosteric modulators of the GABA-A receptor. They bind at the α/γ subunit interface (distinct from the GABA binding site) and increase the frequency of Cl⁻ channel opening, causing neuronal hyperpolarization. However, they differ in which pharmacological actions predominate, largely based on which GABA-A receptor subunits they engage.
The 5 Core Pharmacological Actions
| Action | GABA-A Subunit Responsible | Effect |
|---|---|---|
| Anxiolytic | α2, α3 subunits | Inhibits limbic system neuronal circuits |
| Sedative / Hypnotic | α1 subunit (BZ1/ω1 receptor) | Reduces arousal, produces sleep |
| Anticonvulsant | α1, α2 subunits (partially) | Suppresses seizure spread |
| Muscle Relaxant | α2 subunit in spinal cord | Increases presynaptic inhibition in spinal cord |
| Anterograde Amnesia | α1 subunit (GABA-A) | Impairs encoding of new memories |
All benzodiazepines exhibit all five actions to varying degrees - the difference lies in their relative potency at each action.
- Lippincott Illustrated Reviews: Pharmacology, pp. 547-549
- Goodman & Gilman's Pharmacological Basis of Therapeutics, p. 447
Classification by Predominant Pharmacological Action
1. Anxiolytics (Anti-anxiety)
Act primarily on α2/α3-GABA-A subunits in the limbic system. At low doses, reduce anxiety without causing significant sedation.
| Drug | Notes |
|---|---|
| Alprazolam | First-line for panic disorder; high potency |
| Lorazepam | Also used in acute anxiety and status epilepticus |
| Diazepam | Long-acting; also used in alcohol withdrawal |
| Chlordiazepoxide | First benzodiazepine discovered; alcohol withdrawal |
| Oxazepam | Preferred in elderly/hepatic disease (no active metabolites) |
| Clonazepam | Also potent anticonvulsant |
2. Hypnotics (Sleep induction)
Act predominantly via α1 subunit (BZ1/ω1 receptors). Decrease sleep latency, increase stage II NREM sleep, and decrease REM and slow-wave sleep.
| Drug | Notes |
|---|---|
| Triazolam | Short-acting; sleep onset difficulty |
| Temazepam | Intermediate-acting; sleep maintenance |
| Flurazepam | Long-acting; risk of daytime hangover, avoid in elderly |
| Estazolam | Intermediate-acting hypnotic |
| Quazepam | Long-acting; selective for BZ1 receptors |
| Nitrazepam | Used in some countries for insomnia |
Short-acting hypnotics (e.g., triazolam) are better for difficulty falling asleep. Intermediate-acting agents (e.g., temazepam) are preferred for difficulty staying asleep.
- Lippincott Illustrated Reviews: Pharmacology, p. 550
3. Anticonvulsants
Suppress seizure activity by potentiating GABA-mediated inhibitory circuits at multiple CNS levels.
| Drug | Use |
|---|---|
| Clonazepam | Absence seizures, myoclonic seizures, Lennox-Gastaut syndrome |
| Diazepam (IV) | Status epilepticus (acute termination) |
| Lorazepam (IV) | First-line for status epilepticus |
| Nitrazepam | Infantile spasms (West syndrome) |
| Clorazepate | Adjunct therapy for partial seizures |
Note: Tolerance develops to the anticonvulsant effects over time, which limits long-term use for recurrent seizure disorders.
- Goodman & Gilman's, pp. 447-449
4. Muscle Relaxants
Relax skeletal muscle spasticity via enhanced presynaptic inhibition at spinal cord interneurons (α2-GABA-A). These do not act directly on skeletal muscle.
| Drug | Use |
|---|---|
| Diazepam | Most commonly used; skeletal muscle spasm, spasticity in MS, cerebral palsy |
| Clonazepam | Muscle relaxation in non-sedating doses |
Diazepam is the primary benzodiazepine with clinically relevant muscle relaxant activity. Most other benzodiazepines require doses that also cause significant sedation.
- Goodman & Gilman's, p. 447
5. Pre-anaesthetic / Amnestic Agents
Produce conscious sedation and anterograde amnesia (inability to form new memories after drug administration), mediated by α1-GABA-A receptors.
| Drug | Notes |
|---|---|
| Midazolam | Drug of choice for procedural sedation; water-soluble, rapid onset, short-acting, reliable anterograde amnesia |
| Lorazepam | Used for pre-op anxiety and sedation |
| Diazepam | Pre-anaesthetic medication |
Midazolam is the most widely used benzodiazepine for procedural sedation because it produces reliable anterograde amnesia, has rapid onset, and its effects are reversible with flumazenil.
- Lippincott Illustrated Reviews: Pharmacology, p. 551
Pharmacological Action vs. Receptor Subtype Summary
GABA-A Receptor Subtype → Pharmacological Effect
─────────────────────────────────────────────────
α1 (BZ1 / ω1) → Sedation, Hypnosis, Amnesia
α2 (BZ2 / ω2) → Anxiolysis, Muscle relaxation
α3 → Anxiolysis
α5 → Memory/cognitive effects
This is why Z-drugs (zolpidem, zaleplon, zopiclone) - which are selective for BZ1 (α1) receptors - produce mainly sedation/hypnosis but have less anxiolytic and no muscle relaxant activity compared to classical benzodiazepines.
BZ Receptor Subtypes (Peripheral vs. Central)
| Receptor | Location | Effect |
|---|---|---|
| BZ1 (ω1) | Brain (cortex, cerebellum) | Sedation, hypnosis, amnesia |
| BZ2 (ω2) | Limbic system, spinal cord | Anxiolysis, muscle relaxation, anticonvulsant |
| BZ3 (peripheral BZR) | Peripheral tissues, mitochondria | Steroidogenesis; NOT part of GABA-A complex |
Key Clinical Point: Dose-Dependent Spectrum
As stated in Goodman & Gilman's: "As the dose of a benzodiazepine is increased, sedation progresses to hypnosis and then to stupor." This means the pharmacological effects exist on a continuum:
Low dose → Anxiolysis → Medium dose → Sedation → Higher dose → Hypnosis → Very high dose → Anesthesia/Stupor
- Goodman & Gilman's Pharmacological Basis of Therapeutics, p. 447
- Lippincott Illustrated Reviews: Pharmacology, pp. 546-551
- Roberts and Hedges' Clinical Procedures in Emergency Medicine
This is a shared conversation. Sign in to Orris to start your own chat.