Breast carcinoma
Reading File
Finding Sources
Finding Sources
Searching PubMed
"breast cancer"[MeSH Terms] AND ("treatment"[MeSH Terms] OR "diagnosis"[MeSH Terms])
Reading File
Reading File
Reading File
Reading File
Reading File
Reading File
Reading File
Reading File
Reading File
Loading Image
Loading Image
I now have comprehensive content from multiple authoritative sources. Here is a thorough, well-organized overview of breast carcinoma:
Breast Carcinoma
Epidemiology
Breast cancer is the most common malignancy globally and the leading cause of cancer death in females worldwide. In 2020, it surpassed lung cancer as the most common cancer overall, with an estimated 2.3 million new cases (~12% of all new diagnoses). The lifetime risk for a female living to age 90 in the United States is 1 in 8; approximately 297,790 new invasive cases and >43,000 deaths are estimated annually in the US.
- Most cases (75%) are diagnosed after age 50
- Incidence is highest in North America, Northern and Western Europe, and Australia/New Zealand
- Females of African descent have the highest mortality rate and a higher proportion of TNBC
- The current overall risk of death after diagnosis is approximately 20%, declining by 1-2% per year
(Robbins, Cotran & Kumar Pathologic Basis of Disease; Robbins & Kumar Basic Pathology)
Risk Factors
| Risk Level | Factors |
|---|---|
| Relative risk >4.0 | Female sex, increasing age, germline high-penetrance mutations (BRCA1/2), strong family history (>1 first-degree relative), personal history of breast cancer, high breast density |
| Relative risk 2.1-4.0 | Moderate-penetrance germline mutations, high-dose chest radiation before age 18, family history (1 first-degree relative) |
| Relative risk 1.1-2.0 | Early menarche (<12 yrs), late menopause (>55 yrs), late first pregnancy (>35 yrs), nulliparity, absence of breastfeeding, exogenous hormone therapy, postmenopausal obesity, physical inactivity, high alcohol consumption |
About 20% of breast cancers can be attributed to modifiable risk factors (obesity, alcohol, low physical activity). Early pregnancy (before age 20) and prolonged breastfeeding are the major protective factors.
Risk reduction:
- Bilateral prophylactic mastectomy: reduces risk by ~90%
- Chemoprevention with ER antagonists (tamoxifen, raloxifene): reduces incidence of ER-positive cancers
(Robbins, Cotran & Kumar Pathologic Basis of Disease, p. 972)
Classification
Breast Cancer Classification Diagram
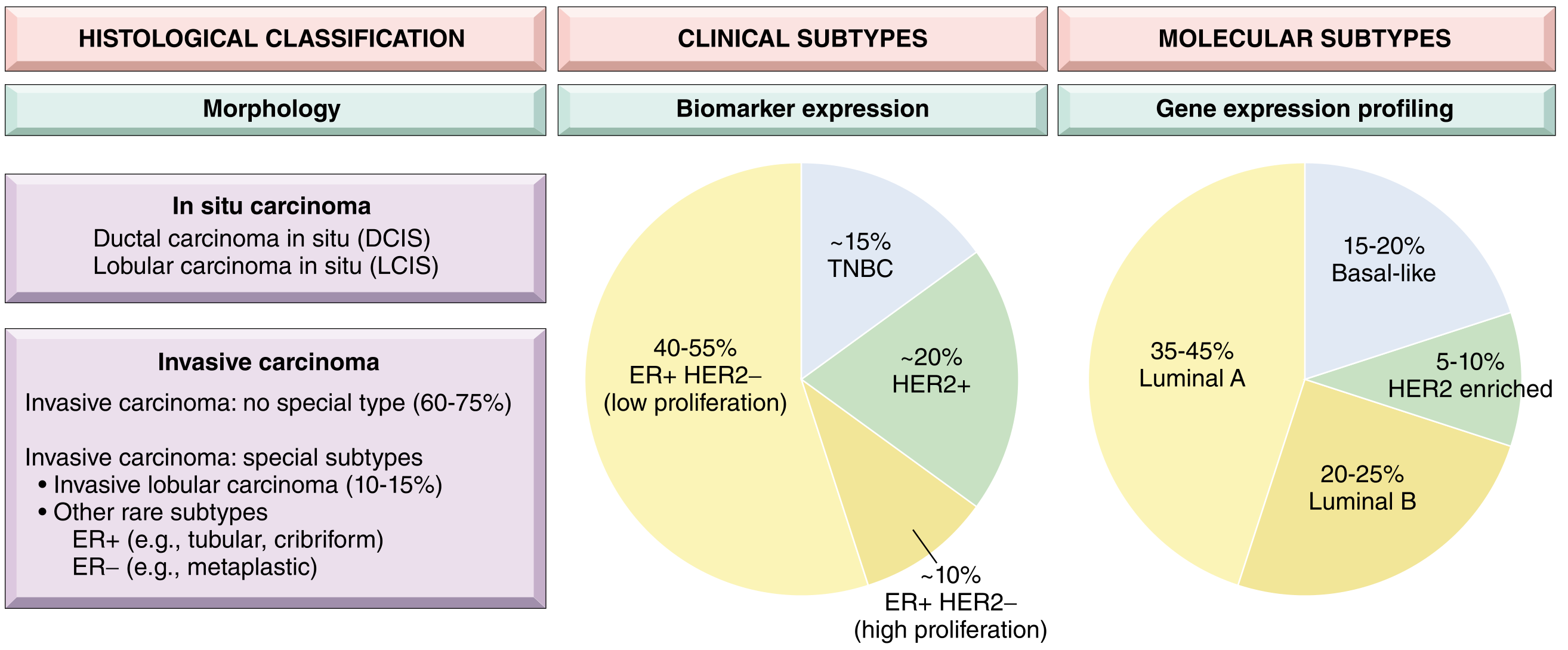
Fig. - Breast cancer classification based on morphology, biomarker expression, and gene expression profiling (Robbins, Cotran & Kumar Pathologic Basis of Disease)
A. In Situ Carcinomas
1. Ductal Carcinoma In Situ (DCIS)
- A precursor to invasive ductal carcinoma
- Most often detected on mammographic screening as clustered microcalcifications (see mammogram below)
- When invasion develops from untreated DCIS, it is usually an invasive ductal carcinoma in the same breast
- Classified by nuclear grade (low, intermediate, high) and architecture (comedo, cribriform, micropapillary, solid)
2. Lobular Carcinoma In Situ (LCIS)
- A marker of increased risk and a precursor lesion
- Non-calcifying; usually not detected by mammography alone
- When invasive carcinoma develops: 2/3 occur in the same breast, 1/3 in the contralateral breast
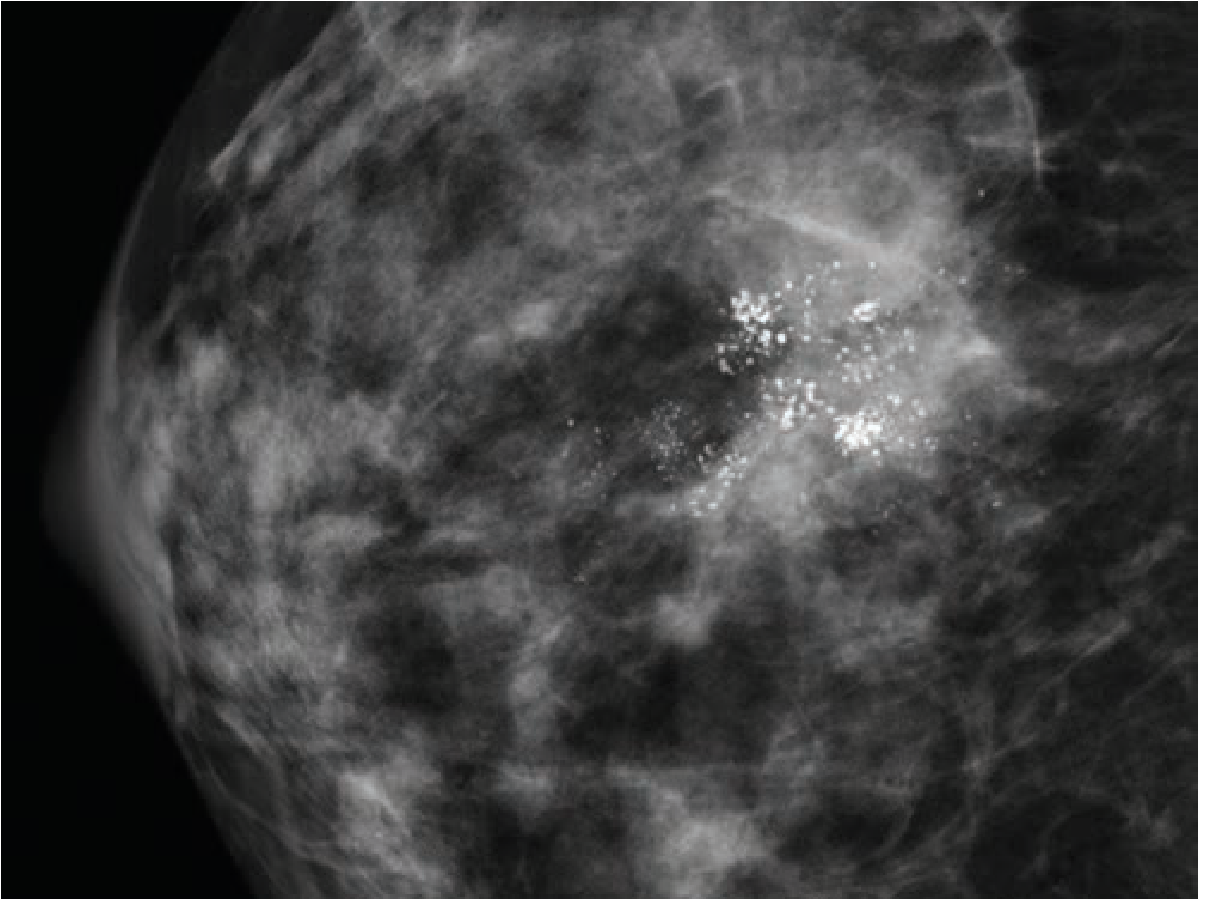
Mammogram showing DCIS with characteristic clustered microcalcifications (Schwartz's Principles of Surgery)
B. Invasive (Infiltrating) Carcinomas - Histological Types
| Type | Frequency | Notes |
|---|---|---|
| Invasive ductal carcinoma - No Special Type (NST) | ~80% | Most common; scirrhous, hard, stellate mass; generally worse prognosis than special types |
| Invasive lobular carcinoma | 10-15% | "Indian file" single-cell pattern; bilateral in up to 20%; tends to be ER+ |
| Medullary carcinoma | ~4% | Well-circumscribed, soft; lymphoplasmacytic infiltrate; paradoxically better prognosis despite high grade |
| Mucinous (colloid) carcinoma | ~2% | Abundant extracellular mucin; better prognosis; seen in older patients |
| Tubular carcinoma | ~2% | Well-differentiated tubular structures; excellent prognosis |
| Papillary carcinoma | ~2% | Well-defined papillary structures |
| Paget's disease of the nipple | Rare | Chronic eczematous eruption of nipple; pathognomonic Paget cells (large, pale, vacuolated) in rete pegs; associated with underlying DCIS or invasive carcinoma |
(Schwartz's Principles of Surgery, 11th Ed.)
Clinical Subtypes by Biomarker Expression
| Subtype | ER | PR | HER2 | Frequency | Key Features |
|---|---|---|---|---|---|
| Luminal A | + | + | - (low proliferation) | 40-55% | Best prognosis; responds to hormone therapy |
| Luminal B | + | +/- | - (high proliferation) | ~10% | Higher grade, worse prognosis than Luminal A |
| HER2-positive | +/- | +/- | + | ~20% | Aggressive; responds to anti-HER2 therapy |
| Triple Negative (TNBC) | - | - | - | ~15% | Basal-like; no targeted therapy; more common in young/African-descent females |
Molecular Pathology and Pathogenesis
Low-grade and high-grade breast carcinomas evolve along separate molecular pathways from distinct precursor lesions.
Hereditary Breast Cancer
- ~12% of all breast cancers result from germline mutations
- BRCA1 and BRCA2 account for half of single-gene mutation cases
- BRCA1 (chromosome 17q21): associated with high-grade, ER-negative, basal-like tumors. Also plays a role in differentiation of ER-negative progenitor cells
- BRCA2 (chromosome 13q12.3): associated with luminal-type tumors
- Other genes: PALB2, ATM, RAD51C, RAD51D, CHEK2 - all involved in homologous recombination repair of double-strand DNA breaks
- Homologous recombination deficiency makes tumor cells susceptible to PARP inhibitors (synthetic lethality)
- In Ashkenazi Jewish populations: ~1 in 40 individuals carries one of three specific mutations (2 in BRCA1, 1 in BRCA2)
Clinical Features
Symptoms and Signs:
- Painless, firm, irregular breast lump (most common presentation)
- Skin dimpling or tethering (Cooper's ligament involvement)
- Nipple retraction or discharge
- Peau d'orange (skin edema due to lymphatic obstruction - classic for inflammatory breast carcinoma)
- Axillary lymphadenopathy
- Rarely, first presentation is distant metastasis (bone, liver, lung, brain)
Inflammatory Breast Carcinoma - a special aggressive form:
- Rapid enlargement, skin erythema, warmth, and peau d'orange
- Due to dermal lymphatic invasion by tumor emboli
- Not necessarily a discrete mass; high-stage at diagnosis; poor prognosis
Diagnosis
Triple Assessment
- Clinical examination
- Imaging - Mammography ± ultrasound ± MRI
- Tissue biopsy - Core-needle biopsy (preferred) or FNA
Imaging
Mammography - primary screening tool
- Suspicious features: spiculated mass, asymmetric thickening, clustered microcalcifications (fine, stippled, linear branching pattern)
- Spot compression and magnification views improve characterization
- Sensitivity limited in dense breasts
Ultrasound
- Best for distinguishing solid vs. cystic lesions
- Assesses axillary lymph nodes for malignant morphology
MRI
- Detects multifocal/multicentric disease and contralateral tumors not seen on mammography
- Used in BRCA mutation carriers for screening
Biopsy
- Core-needle biopsy is preferred: gives histological diagnosis, grade, receptor status (ER, PR, HER2), and Ki-67
- FNA: cytology only; cannot determine invasive vs. in situ
- All primary invasive breast cancers must be tested for ER, PR, and HER2
- HER2 assessed by immunohistochemistry (IHC) for protein overexpression or FISH for gene amplification
(Schwartz's Principles of Surgery, 11th Ed.)
Staging (AJCC 8th Edition)
Staging is anatomic (clinical/pathological) based on:
- T - Tumor size and local extent
- N - Regional lymph node involvement
- M - Distant metastasis
| Stage | Approximate Description |
|---|---|
| 0 | DCIS / LCIS |
| I | T ≤2 cm, node negative |
| II | T >2 cm or 1-3 positive nodes |
| III | Locally advanced (chest wall, skin, or ≥4 nodes) |
| IV | Distant metastasis |
Post-neoadjuvant staging is prefixed with "yp" (e.g., ypT0ypN0 = pathological complete response, pCR).
Treatment
Surgery
Breast-conserving surgery (BCS / lumpectomy) + radiation is equivalent to mastectomy in survival for most early-stage cancers.
Mastectomy indications: large tumor:breast ratio, multicentric disease, prior chest radiation, BRCA mutation, patient preference.
Axillary staging:
- Sentinel lymph node biopsy (SLNB) - standard for clinically node-negative disease
- Axillary lymph node dissection (ALND) - if positive nodes confirmed clinically or on SLNB
Paget's disease: lumpectomy or mastectomy depending on extent of nipple-areolar complex and underlying DCIS/invasive cancer.
Systemic Therapy
1. Endocrine (hormone) therapy - for ER/PR-positive tumors
- Tamoxifen (ER antagonist): premenopausal women; reduces recurrence by ~50%
- Aromatase inhibitors (anastrozole, letrozole, exemestane): postmenopausal women; superior to tamoxifen in postmenopausal setting
- CDK4/6 inhibitors (palbociclib, ribociclib, abemaciclib): combined with aromatase inhibitors for ER+ HER2- metastatic disease
2. Anti-HER2 therapy - for HER2-positive tumors
- Trastuzumab (Herceptin): monoclonal antibody vs. HER2; dramatically improves outcomes in HER2-amplified disease
- Pertuzumab: dual HER2 blockade combined with trastuzumab
- T-DM1 (ado-trastuzumab emtansine): antibody-drug conjugate for residual disease after neoadjuvant therapy
3. Chemotherapy
- Anthracyclines (doxorubicin, epirubicin) and taxanes (paclitaxel, docetaxel) are the backbone agents
- Used in neoadjuvant (before surgery) or adjuvant (after surgery) settings
- TNBC and high-risk HER2+ cancers: neoadjuvant chemo +/- immunotherapy (pembrolizumab for TNBC)
4. PARP inhibitors - for BRCA1/2 germline mutation carriers with HER2-negative metastatic disease
- Olaparib, talazoparib
- Mechanism: synthetic lethality in homologous recombination-deficient tumors
Radiation
- Adjuvant radiation after BCS reduces local recurrence by ~70%
- Post-mastectomy radiation for high-risk features (positive margins, ≥4 nodes, T3/T4)
Prognosis
Prognosis depends on:
- Biologic subtype: Luminal A has the best prognosis; TNBC and HER2+ (pre-targeted therapy) have worse outcomes
- Anatomic stage: Tumor size and nodal status
- Grade: Histologic grade (Nottingham grading system - tubule formation, nuclear pleomorphism, mitotic index)
- Biomarker expression: ER+/HER2- tumors have better prognosis than TNBC
- Gene expression assays: Oncotype DX (21-gene recurrence score), MammaPrint (70-gene signature) - guide adjuvant chemotherapy decisions in ER+ early breast cancer
Key Sources:
- Robbins, Cotran & Kumar Pathologic Basis of Disease (primary reference for pathology, molecular classification)
- Robbins & Kumar Basic Pathology (epidemiology, in situ vs invasive distinctions)
- Schwartz's Principles of Surgery, 11th Ed. (histological types, staging, surgical management, biomarker testing)
- Bailey and Love's Short Practice of Surgery, 28th Ed. (clinical management, metastatic disease)
This is a shared conversation. Sign in to Orris to start your own chat.