3rd degree uterine prolapse
Reading File
Finding Sources
Searching PubMed
"uterine prolapse" AND "pelvic organ prolapse" management
Reading File
Finding Sources
Searching Images
uterine prolapse degree grade classification
Reading File
Finding Sources
Reading File
Reading File
Finding Sources
Loading Image
Finding Sources
Reading File
Reading File
Reading File
I now have comprehensive information to provide a thorough answer on 3rd degree uterine prolapse. Let me compile this.
3rd Degree Uterine Prolapse (Procidentia)
Definition & Classification
3rd degree uterine prolapse (also called procidentia or complete prolapse) is defined as descent of the uterus such that the cervix protrudes beyond the vaginal introitus — i.e., the entire uterus lies outside the vulva.
Classification Systems Compared
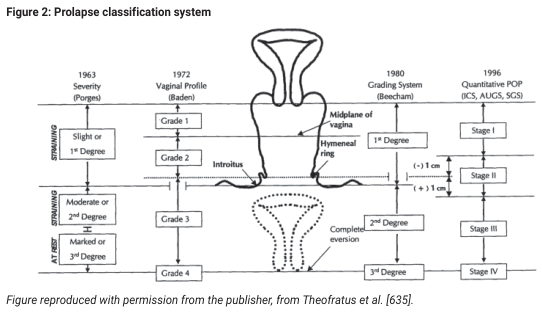
| System | 3rd Degree Definition |
|---|---|
| Beecham (1980) | Complete eversion of the uterus |
| Baden-Walker (1972) | Grade 3–4: descent halfway or more past the hymen |
| Porges (1963) | "Marked" / 3rd degree |
| POPQ (ICS, 1996) | Stage III–IV: leading edge >1 cm beyond hymen; Stage IV = complete eversion |
The modern standard is the POPQ (Pelvic Organ Prolapse Quantification) system, which uses anatomic measurement points (Aa, Ba, C, D, Ap, Bp) relative to the hymenal ring. Stage III/IV corresponds to clinical 3rd degree. — Campbell-Walsh-Wein Urology, p. 3407
Anatomy & Pathophysiology
The uterus is normally suspended by the cardinal-uterosacral ligament complex. The broad ligament provides little structural support. Prolapse results from:
- Attenuation or tearing of the cardinal and uterosacral ligaments
- Pelvic floor muscle weakness (levator ani damage)
- Progressive loss of apical vaginal support
Risk factors include: vaginal delivery (especially prolonged/obstructed labor), increasing parity, advancing age, menopause (estrogen deficiency), obesity, chronic raised intra-abdominal pressure (constipation, COPD), and connective tissue disorders. — Campbell-Walsh-Wein Urology, p. 3406
Clinical Features
- Sensation of a lump protruding from the vagina
- Pelvic pressure, heaviness, dragging discomfort
- Difficulty walking or sitting
- Ulceration and decubitus ulcers on the exposed cervix/vaginal epithelium (from friction and dryness)
- Urinary symptoms: retention, incomplete emptying, incontinence (or paradoxically, stress incontinence may be masked by urethral kinking)
- Defecatory symptoms: incomplete evacuation, constipation, the need for manual reduction to void/defecate
- Sexual dysfunction
Note: Symptom severity does not always correlate with anatomic stage — some women with Stage III/IV prolapse are minimally symptomatic. — Berek & Novak's Gynecology, p. 1620
Management
1. Conservative (Non-Surgical)
Pessary — the cornerstone of non-surgical management for 3rd degree prolapse:
- Donut pessary — preferred for 3rd degree / complete procidentia with decreased perineal support
- Gellhorn pessary — provides strong support via space occupation and suction; can remain in situ up to 6–8 weeks
- Cube/Tandem-Cube pessary — for maximum support; must be removed daily
- Ring pessaries are generally not sufficient for 3rd degree prolapse (better for 1st–2nd degree)
Pessary fitting is empirical (trial-and-error). Adequate fit is confirmed when a finger can sweep between the pessary and vaginal wall, the patient can void with it in place, and the pessary is retained during Valsalva/cough. Follow-up at 1–2 weeks, then 4–6 weeks, then every 6–12 months (or 4–12 weeks if provider-dependent removal). — Berek & Novak's Gynecology, pp. 1618–1619
Other conservative measures: pelvic floor muscle training, weight reduction, estrogen therapy (local), management of chronic cough/constipation.
2. Surgical Management
Surgery is indicated when conservative treatment has failed or is declined, and prolapse is symptomatic (or ≥ Stage II with progression). — Berek & Novak's Gynecology, p. 1620
Surgical approaches: vaginal, abdominal, laparoscopic, or combined.
Three broad categories:
| Category | Description |
|---|---|
| Reconstructive | Native tissue repair using endogenous support structures |
| Compensatory (Augmentation) | Graft/mesh to replace deficient support |
| Obliterative | Colpocleisis — partial/complete vaginal closure (for non-sexually active patients) |
Key Procedures for 3rd Degree Prolapse
Vaginal Hysterectomy + Apical Suspension (traditional standard):
- Vaginal hysterectomy alone is insufficient — apical suspension must be added to prevent vault prolapse recurrence
- McCall culdoplasty: posterior culdoplasty using uterosacral ligaments to suspend the vaginal apex and obliterate the cul-de-sac (prevents enterocele)
- Uterosacral ligament suspension (USLS)
- Sacrospinous ligament fixation (SSLF)
Uterine-Preserving Options (hysteropexy):
- Growing preference — up to 60% of women decline hysterectomy when given a choice
- Benefits include: reduced mesh erosion risk, shorter operative time, less blood loss, shorter hospital stay, no significant difference in short-term recurrence
- Manchester (Fothergill) procedure: cervical amputation + cardinal ligament plication
- Sacrospinous cervicopexy
- Laparoscopic/robotic sacrohysteropexy
Abdominal/Laparoscopic Sacrocolpopexy: uses mesh graft from vaginal apex to sacral promontory; the gold standard for vault prolapse, may be used with hysterectomy or uterine preservation.
Obliterative surgery (Colpocleisis): considered when sexual function is not desired; high success rates with lower morbidity in frail/elderly patients.
⚠️ Apical support is the key to a successful prolapse repair. Multiple studies show that correcting the anterior wall without addressing the apex markedly increases recurrence risk. — Berek & Novak's Gynecology, p. 1621
Complications of Untreated Prolapse
- Cervical/vaginal ulceration, keratinization, and infection
- Urinary retention and recurrent UTIs
- Hydronephrosis (in severe cases from ureteral kinking)
- Rarely: malignant transformation in chronic decubitus ulcers
POPQ Staging Summary
| Stage | Definition |
|---|---|
| 0 | No prolapse |
| I | Leading edge > 1 cm above hymen |
| II | Leading edge between −1 cm and +1 cm of hymen |
| III | Leading edge > 1 cm beyond hymen but < total vaginal length − 2 cm |
| IV | Complete eversion (= total vaginal length) |
Stage III/IV = clinical 3rd degree. — Campbell-Walsh-Wein Urology, p. 3407
Sources: Berek & Novak's Gynecology (pp. 1618–1623); Campbell-Walsh-Wein Urology (pp. 3406–3412); Management of Non-Neurogenic Female Lower Urinary Tract Symptoms (prolapse classification systems)
Gynae
Asking for Preferences
Arsenic poisoning in Fmt Mainly chronic
Reading File
Finding Sources
Finding Sources
Reading File
Reading File
Reading File
Reading File
Reading File
Searching Images
chronic arsenic poisoning skin changes keratosis hyperpigmentation Mees lines
Loading Image
Loading Image
Finding Sources
Reading File
Reading File
Reading File
Comprehensive data collected. Here is the full FMT-oriented answer on chronic arsenic poisoning.
Arsenic Poisoning — Forensic Medicine & Toxicology (Focus: Chronic)
1. Introduction & Forensic Significance
Arsenic (As) is a classic homicidal and suicidal poison in forensic toxicology due to:
- Tasteless, odourless (white arsenic/arsenic trioxide)
- Resemblance of acute symptoms to gastroenteritis → historically called the "King of Poisons" and "Poison of Kings"
- Chronic administration is difficult to detect clinically
- Inorganic arsenic is a recognised human carcinogen (lung, skin, bladder)
Arsenic ranks 20th in elemental abundance. Toxic forms are inorganic (trivalent As³⁺ > pentavalent As⁵⁺ in acute toxicity). — Dermatology 2-Volume Set 5e
2. Sources of Exposure
| Category | Examples |
|---|---|
| Homicidal/suicidal | Arsenic trioxide (white arsenic), Fowler's solution (liquor potassii arsenitis) |
| Contaminated water | Groundwater in Bangladesh, India, China, Chile, Argentina, Taiwan, western USA |
| Occupational | Pesticides, herbicides, mining/smelting, electroplating, glass manufacture, wood preservatives (chromated copper arsenate), semiconductor (gallium arsenide) manufacture |
| Food | Shellfish, seaweed, tuna, cod liver oil (organic arsenobetaine — non-toxic) |
| Medicinal (historical) | Fowler's solution (asthma, psoriasis), Salvarsan, arsenic trioxide (current use: acute promyelocytic leukaemia) |
WHO drinking water limit: 0.01 mg/L. — Dermatology 2-Volume Set 5e
3. Mechanism of Toxicity
Trivalent arsenic (As³⁺, arsenite) — primary toxic form:
- Binds sulfhydryl (–SH) groups of critical enzymes → inhibits the pyruvate dehydrogenase complex and Krebs cycle enzymes (especially lipoic acid's two –SH groups) → impaired gluconeogenesis and oxidative phosphorylation → depletion of cellular ATP
- Inhibits cardiac potassium channels → QT prolongation
- Induces oxidative stress, DNA damage, impairs DNA repair → carcinogenesis
- Alters gene expression via epigenetic mechanisms (arsenic methylation requires S-adenosylmethionine → disrupts one-carbon metabolism)
Pentavalent arsenic (As⁵⁺, arsenate):
- Substitutes for phosphate in biochemical reactions → uncouples oxidative phosphorylation
- In vivo interconversion between As³⁺ and As⁵⁺ occurs
Metabolism:
- Absorbed via GIT and lungs; distributed to liver, kidney, heart, lungs
- Methylated in liver → monomethylarsonic acid (MMA) → dimethylarsinic acid (DMA) (less toxic)
- Concentrated in keratin-rich tissues (hair, nails, skin)
- Excreted predominantly in urine (~⅔ within 2–3 days at low doses)
— Goldman-Cecil Medicine; Katzung's Basic & Clinical Pharmacology 16e
4. Chronic Arsenic Poisoning (Arsenicosis/Arsenicism)
Overt non-carcinogenic effects appear with chronic absorption of >0.01 mg/kg/day (~500–1000 µg/day in adults). Onset varies with dose and individual tolerance.
A. Constitutional Symptoms
- Fatigue, weakness, weight loss
- Non-specific GI complaints, diarrhoea
- Anorexia
B. Dermatological Features ⭐ (Most Characteristic — Forensically Important)
Hyperpigmentation — the hallmark:
- "Raindrops on a dusty road" pattern: mottled hyperpigmentation with superimposed guttate (raindrop) hypopigmentation
- Sites: axillae, groins, nipples, palms, soles, pressure points, trunk, extremities
- Mucous membrane melanosis (tongue) may also occur
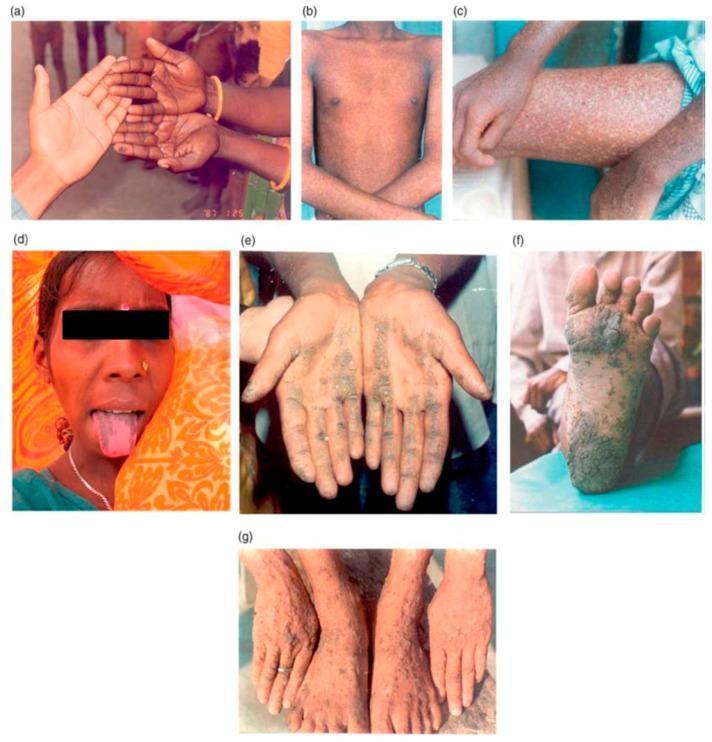
Arsenical keratoses — pre-malignant:
- Symmetric yellow, punctate, corn-like papules 2–10 mm
- Palms and soles (thenar/hypothenar eminences, distal palms, lateral fingers, weight-bearing plantar surfaces)
- Rarely: trunk, proximal extremities, eyelids, genitalia
- May coalesce into plaques
Mees' lines (Aldrich-Mees lines):
- Transverse white bands on nails (1–2 mm wide)
- Appear 8 weeks after acute exposure or with chronic poisoning
- Reflect growth interruption — of forensic importance for timing of exposure
- Also seen after acute poisoning (2–6 months later)
Alopecia — diffuse hair loss
Blackfoot disease (endemic in Taiwan):
- Peripheral vascular occlusive disease → gangrene and blackening of extremities

C. Neurological Features
- Peripheral neuropathy: diffuse, symmetrical, ascending, painful sensorimotor neuropathy in stocking-glove distribution (distal axonopathy — dying-back pattern)
- In severe poisoning: ascending weakness/paralysis → respiratory failure mimicking Guillain-Barré syndrome
- Encephalopathy: headache, drowsiness, confusion, delirium, convulsions
- CSF protein may be raised (50–100 mg/dL)
D. Haematological Features
- Pancytopenia (anaemia + leukopenia + thrombocytopenia)
- Anaemia — normocytic normochromic or megaloblastic
- Basophilic stippling of erythrocytes
- Karyorrhexis
- Eosinophilia
E. Other Systemic Effects
| System | Features |
|---|---|
| Cardiovascular | QT prolongation → torsades de pointes; peripheral vascular disease; increased cardiovascular mortality |
| Hepatic | Non-cirrhotic portal hypertension, hepatomegaly, hepatic fibrosis |
| Renal | Renal dysfunction |
| Pulmonary | Dose-dependent lung function decline; obstructive/restrictive disease |
| ENT | Nasal septum perforation |
| Metabolic | Diabetes mellitus |
F. Malignancies (Arsenic as Human Carcinogen)
- Skin: Bowen disease (squamous cell carcinoma in situ), basal cell carcinoma, squamous cell carcinoma — histologically almost identical to actinic neoplasia
- Lung carcinoma
- Bladder carcinoma
- Possibly kidney and liver
5. Diagnosis
Investigations — Forensically Critical
| Sample | Normal | Abnormal / Diagnostic |
|---|---|---|
| Urine (spot) | <20 µg/L (inorganic + MMA + DMA) | >50 µg/L → do 24-hr collection |
| Urine (24-hr) | — | >50 µg or >100 µg/g creatinine |
| Blood | <1 µg/L | Elevated in acute; clears quickly — unreliable for chronic |
| Hair | <1 ppm (<0.1 mg/100 mg) | >0.1 mg/100 mg = significant |
| Nails | <1 ppm | >1 ppm = significant |
⚠️ Forensic caveat: Seafood consumers may have urine arsenic >1500 µg/L from non-toxic organic arsenic (arsenobetaine). Speciation (inorganic vs. organic) is essential. Seafood must be avoided ≥3 days before sampling.
Segmental hair analysis: Arsenic is incorporated into hair within 2 weeks of exposure and remains for long periods → used forensically to determine the timing and duration of poisoning. Neutron activation analysis or synchrotron radiation are preferred methods.
ECG: QT prolongation, ST-T changes
Nerve conduction studies: Distal symmetrical sensorimotor axonopathy; conduction slowing in severe cases
Blood film: Basophilic stippling, karyorrhexis
6. Treatment
| Priority | Measure |
|---|---|
| First | Remove from source of exposure |
| Supportive | Fluid resuscitation, electrolyte correction |
| Chelation (acute severe) | Dimercaprol (BAL) 3–5 mg/kg IM every 4–6 hours or Unithiol (DMPS) 3–5 mg/kg IV every 4–6 hours — start immediately if high suspicion, do not await labs |
| Oral chelation | Succimer (DMSA) — effective; preferred over BAL (higher therapeutic index, less toxic); oral route may be limited in acute GI involvement |
| Chronic poisoning | Chelation benefit not clearly proven; removal from exposure is the primary intervention; empiric short-course oral succimer/unithiol may be considered for symptomatic individuals |
| Arsine gas (special case) | Exchange transfusion (removes arsenic, hemoglobin pigments, restores RBCs) + dialysis for renal failure |
Once peripheral neuropathy is established, it is little affected by BAL; recovery is slow and may be partial. Other manifestations (skin, bone marrow) respond more favourably. — Adams & Victor's Principles of Neurology 12e
7. Prognosis
- ECG changes and bone marrow suppression: reversible after exposure ceases
- Encephalopathy and neuropathy: may be permanent
- Skin changes: can improve with removal from exposure but may progress to malignancy
- High-dose arsine inhalation: can be fatal
Sources: Katzung's Basic & Clinical Pharmacology 16e; Goldman-Cecil Medicine; Dermatology 2-Volume Set 5e; Adams & Victor's Principles of Neurology 12e; Henry's Clinical Diagnosis and Management
What is fracture
Your credits are exhausted. Your daily credits reset tomorrow, or you can purchase a top-up for more.
This is a shared conversation. Sign in to Orris to start your own chat.