Alveolar arterial gradient Full details for md exams 10 marks answer
Reading File
Finding Sources
Finding Sources
Finding Sources
Reading File
Reading File
Reading File
Reading File
Reading File
Reading File
Reading File
Finding Sources
Loading Image
Loading Image
Loading Image
I now have excellent, comprehensive material from multiple authoritative sources. Let me compose the full 10-mark MD exam answer.
Alveolar-Arterial (A-a) Gradient - Complete Answer for MD Exams
Definition
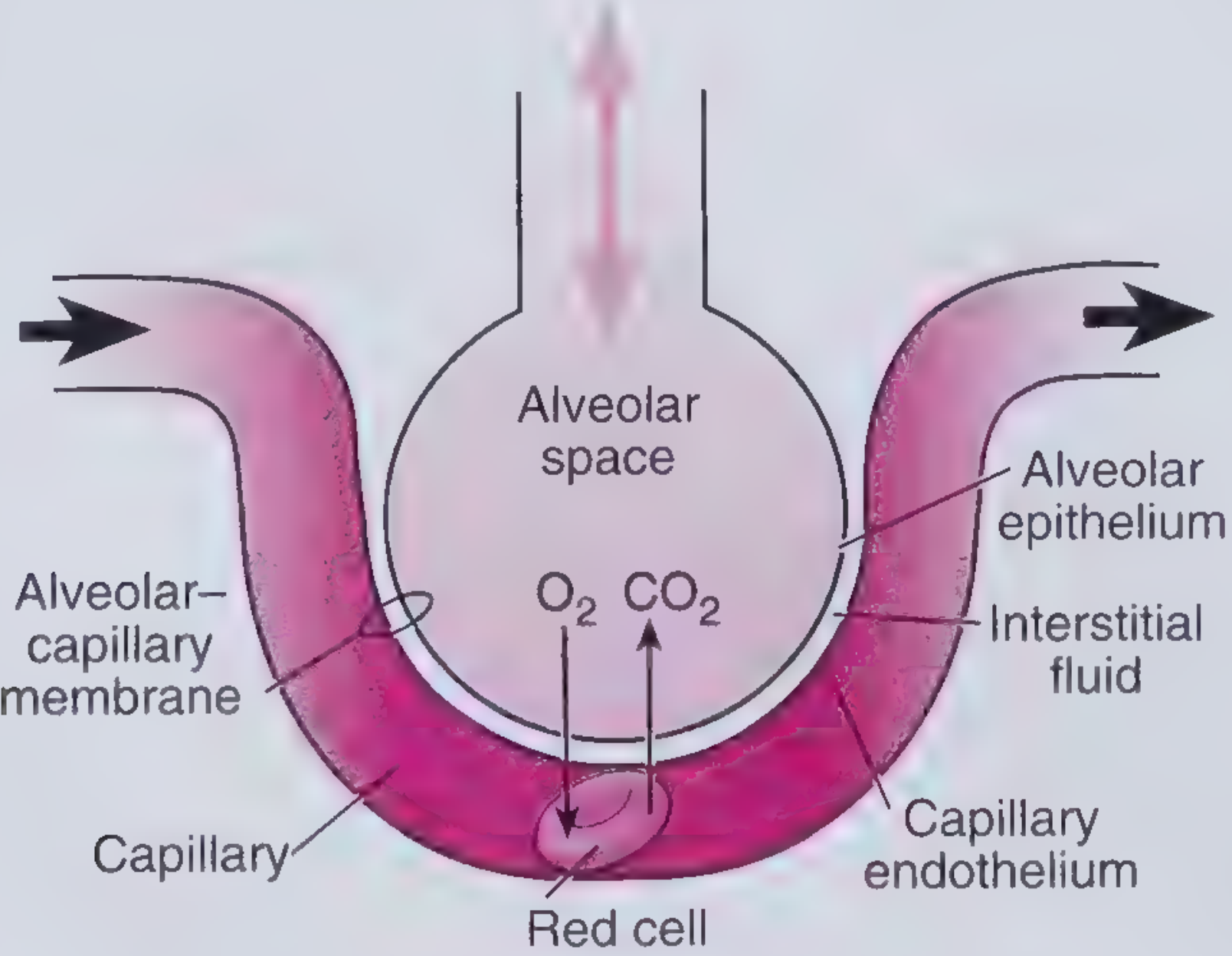
The Alveolar-Arterial (A-a) oxygen gradient is the difference between the partial pressure of oxygen in the alveolus (PAO2) and the partial pressure of oxygen in the systemic arterial blood (PaO2).
A-a gradient = PAO2 - PaO2
It is the single most useful index for evaluating the efficiency of oxygen transfer across the lung. A normal lung has minimal difference between alveolar and arterial PO2; when this gradient widens, it signals a defect in O2 equilibration between alveolar gas and pulmonary capillary blood.
- Medical Physiology (Boron & Boulpaep), p. 1776
- Costanzo Physiology 7th Ed., p. 246
The Alveolar Gas Equation (Essential for Calculating PAO2)
PAO2 cannot be measured directly - it is calculated using the Alveolar Gas Equation:
$$PAO_2 = FiO_2 \times (P_B - P_{H_2O}) - \frac{PaCO_2}{R}$$
Where:
- FiO2 = fraction of inspired oxygen (0.21 on room air)
- PB = barometric pressure (760 mm Hg at sea level)
- PH2O = water vapor pressure at body temperature (47 mm Hg)
- PaCO2 = arterial CO2 tension (assumed equal to alveolar CO2 = 40 mm Hg normally)
- R = respiratory quotient (0.8 on a mixed diet)
At sea level on room air (simplified form):
$$PAO_2 = 150 - \frac{PaCO_2}{0.8} \approx 150 - 1.25 \times PaCO_2$$
With normal PaCO2 of 40 mm Hg:
$$PAO_2 = (0.21 \times [760 - 47]) - (40 / 0.8) = \sim100 \text{ mm Hg}$$
Therefore:
$$A\text{-}a \ gradient = PAO_2 - PaO_2 = 100 - 95 = \sim 5 \text{ mm Hg (normal)}$$
- Frameworks for Internal Medicine, p. 632
- Comprehensive Clinical Nephrology 7th Ed., p. 226
Normal Values
| Age (years) | Upper limit of normal A-a gradient (mm Hg) |
|---|---|
| 20 | 17 |
| 30 | 20 |
| 40 | 23 |
| 50 | 26 |
| 60 | 30 |
| 70+ | ~35 |
General rule for upper limit of normal:
$$A\text{-}a \ gradient \ (normal) = \frac{Age + 10}{4}$$
Range at rest on room air: 5-15 mm Hg (young adults), up to 25 mm Hg (elderly).
Important: Normal A-a gradient increases with:
- Age - due to progressive V/Q mismatch from loss of lung elasticity
- Increasing FiO2 - breathing supplemental O2 widens the measurable gradient
- Frameworks for Internal Medicine (Table 46-1), p. 632
Physiological Basis - Why Does a Normal A-a Gradient Exist?
Even in healthy lungs, a small A-a gradient of 5-15 mm Hg exists because of:
- Physiological V/Q mismatch - ventilation and perfusion are not perfectly matched throughout the lung (apex vs. base differences)
- Anatomic shunts - bronchial veins and Thebesian veins drain directly into the left side of the circulation, bypassing alveolar gas exchange (~2-3% of cardiac output)
- Diffusion limitation at rest is minimal but becomes relevant in disease
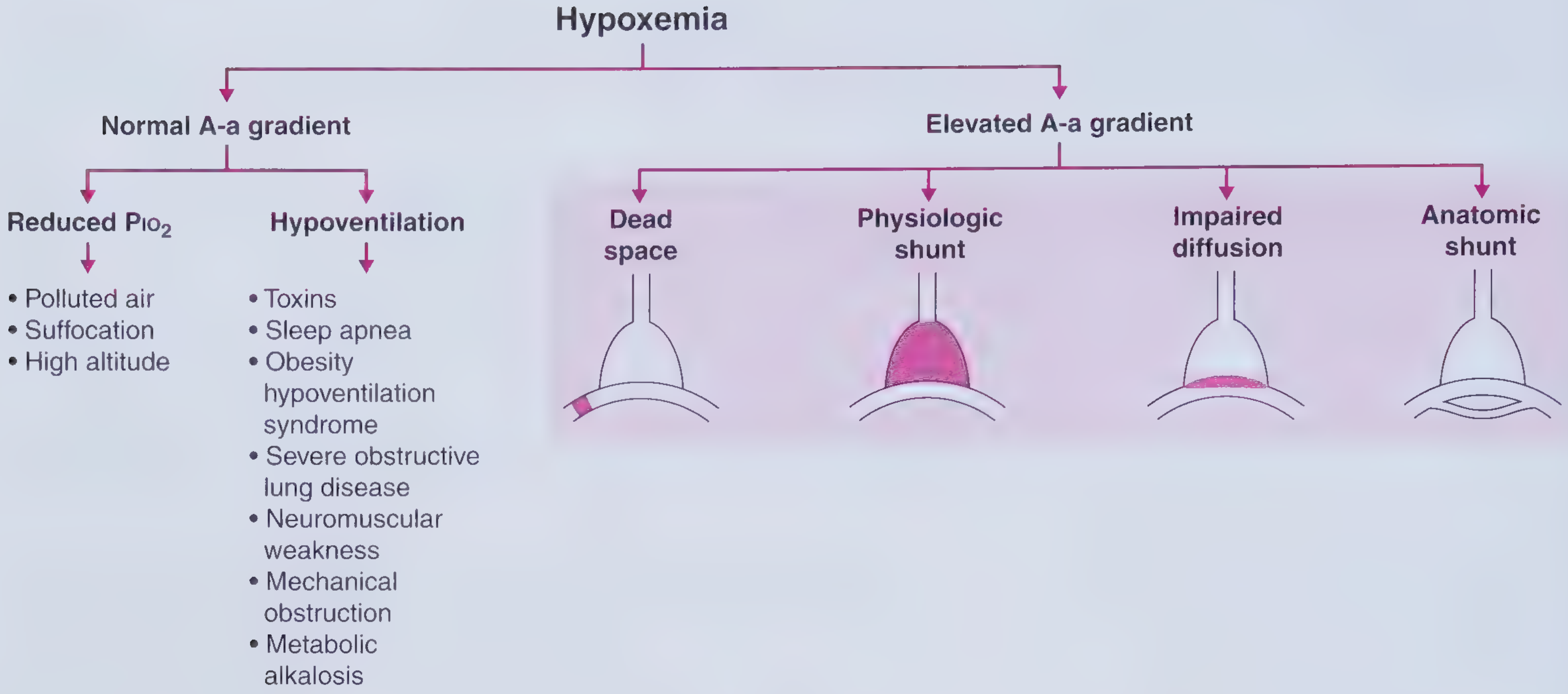
Classification of Hypoxemia by A-a Gradient
This is the most clinically important use of the A-a gradient:

A. Hypoxemia with NORMAL A-a Gradient
The lung is intrinsically normal - the problem is upstream (insufficient inspired O2 or reduced alveolar ventilation). O2 equilibrates normally across the alveolar-capillary membrane, so PAO2 and PaO2 fall together.
| Mechanism | Explanation | Examples |
|---|---|---|
| Reduced PiO2 | Decreased FiO2 or decreased barometric pressure reduces both alveolar and arterial PO2 equally | High altitude, smoke inhalation, suffocation |
| Hypoventilation | Less fresh air enters alveoli per breath; CO2 accumulates and displaces O2 (PAO2 falls). Equilibration is intact so PaO2 falls equally. PaCO2 is elevated | Opioid/sedative overdose, neuromuscular disease, sleep apnea, obesity hypoventilation syndrome, mechanical obstruction, metabolic alkalosis |
Key feature: Both conditions respond well to supplemental O2 (raising FiO2 raises PAO2, which raises PaO2).
Costanzo Physiology 7th Ed., p. 246
B. Hypoxemia with ELEVATED (Widened) A-a Gradient
The lung itself is diseased - O2 does not equilibrate fully across the alveolar-capillary barrier. PaO2 falls disproportionately compared to PAO2.
1. V/Q Mismatch (Most Common Cause)
- Ventilation and perfusion are mismatched in different lung regions
- Low V/Q regions (perfusion > ventilation): blood passes alveoli with low O2 tension - poorly oxygenated blood enters systemic circulation
- High V/Q regions (dead space physiology): wasted ventilation
- The admixture of blood from low V/Q regions drags down overall PaO2
- Examples: COPD, asthma, pneumonia, pulmonary embolism
- Responds to supplemental O2 (raising FiO2 improves oxygenation in low V/Q units)
2. Right-to-Left Shunt
- Deoxygenated blood bypasses ventilated alveoli entirely (V/Q = 0)
- Anatomic shunt: ASD with reversed shunt, VSD, pulmonary AVM, hepatopulmonary syndrome
- Physiologic shunt: lobar pneumonia, complete atelectasis, ARDS (flooded/collapsed alveoli)
- Hallmark: PaO2 does NOT improve significantly with 100% O2 - this distinguishes shunt from other causes. Even breathing 100% O2, the shunted blood remains unoxygenated and mixes with oxygenated blood, limiting the PaO2 rise
- Medical Physiology (Boron & Boulpaep), p. 1783-1785
3. Diffusion Impairment
- Thickening of the alveolar-capillary membrane increases diffusion distance, reducing O2 transfer
- O2 does not fully equilibrate across the membrane before blood exits the capillary
- Examples: interstitial pulmonary fibrosis, pulmonary edema, sarcoidosis
- Responds to supplemental O2 (raising driving force for diffusion)
4. Increased Dead Space (as a V/Q mismatch subtype)
- Pulmonary embolism is the classic example: normal ventilation with no perfusion (V/Q = ∞)
- The embolized lung contributes to dead space; remaining vascular bed receives excess perfusion, creating V/Q mismatch in adjacent lung regions
- Results in widened A-a gradient plus often hypocapnia (hyperventilation is a compensatory response)
Goldman-Cecil Medicine (Table 89-1), p. 1040
Summary Table: A-a Gradient in Different Causes of Hypoxemia
| Mechanism | PaO2 | PaCO2 | A-a Gradient | Response to O2 |
|---|---|---|---|---|
| High altitude | ↓ | N or ↓ | Normal | Yes |
| Hypoventilation | ↓ | ↑ | Normal | Yes |
| V/Q mismatch | ↓ | N or ↓ | Increased | Yes |
| Diffusion defect | ↓ | N | Increased | Yes |
| Right-to-left shunt | ↓ | N or ↓ | Increased | Limited |
Costanzo Physiology 7th Ed., p. 246; Frameworks for Internal Medicine, p. 636
Clinical Uses of the A-a Gradient
1. Differentiating Causes of Hypoxemia
The primary clinical use - see table above. A normal A-a gradient immediately localizes the problem to hypoventilation or reduced inspired O2, sparing the need for extensive lung workup.
2. Diagnosing Pulmonary Embolism
- PE causes a widened A-a gradient from dead space V/Q mismatch and often hypocapnia
- ABG showing hypoxemia + respiratory alkalosis + widened A-a gradient raises suspicion for PE
- However, a normal A-a gradient does not exclude PE (can be normal in a minority of cases)
- Harrison's Principles of Internal Medicine 22E; Rosen's Emergency Medicine
3. Assessing Severity of Lung Disease
- The magnitude of gradient widening reflects the degree of V/Q mismatch
- Used in ICU for monitoring - serial A-a gradient values track progression or improvement in ARDS, pneumonia, respiratory failure
- In mild pulmonary disease: A-a gradient < 35 mm Hg; in severe disease: > 35 mm Hg (as in pneumocystis pneumonia severity grading)
- Fishman's Pulmonary Diseases and Disorders
4. Distinguishing Shunt from Other Causes
- 100% O2 test: if PaO2 rises to >400-500 mm Hg, there is no significant shunt; if it remains low despite 100% O2, an anatomic or physiologic shunt is present
- Medical Physiology (Boron & Boulpaep), p. 1783
5. Detecting Occult Lung Disease
- A widened A-a gradient on ABG in a patient with normal spirometry suggests underlying parenchymal or vascular disease
Worked Numerical Example (High-Yield for Exams)
Case 1 - Hypoventilation (e.g., opioid overdose):
- PaO2 = 70, PaCO2 = 60 on room air
- PAO2 = 150 - (1.25 × 60) = 150 - 75 = 75 mm Hg
- A-a gradient = 75 - 70 = 5 mm Hg → Normal
- Interpretation: pure hypoventilation; lungs are intrinsically normal
Case 2 - V/Q Mismatch (e.g., pneumonia):
- PaO2 = 70, PaCO2 = 40 on room air
- PAO2 = 150 - (1.25 × 40) = 150 - 50 = 100 mm Hg
- A-a gradient = 100 - 70 = 30 mm Hg → Widened
- Interpretation: lung parenchymal/vascular disease
Comprehensive Clinical Nephrology 7th Ed. (Box 15.1), p. 226
Factors That Affect the A-a Gradient
| Factor | Effect on A-a Gradient |
|---|---|
| Age | Increases (V/Q mismatch worsens) |
| Increasing FiO2 | Increases (even in normal individuals) |
| Exercise | Slightly increases |
| Upright vs. supine position | Decreases supine (more uniform perfusion) |
| Obesity | Increases |
Key Points to Remember for MD Exams
- Formula: A-a gradient = PAO2 - PaO2; PAO2 is calculated, PaO2 is measured on ABG
- Normal: 5-15 mm Hg (young adult); formula = (Age + 10) / 4
- Normal A-a gradient + hypoxemia = hypoventilation or reduced PiO2 (lung is healthy)
- Widened A-a gradient + hypoxemia = V/Q mismatch, shunt, or diffusion defect (lung is diseased)
- Failure to correct with 100% O2 is pathognomonic of right-to-left shunt
- V/Q mismatch is the most common cause of widened A-a gradient in clinical practice
- In pure hypoventilation, PaCO2 is always elevated
- The A-a gradient is also widened in hepatopulmonary syndrome (intrapulmonary vasodilation creates diffusion-perfusion impairment)
Sources: Medical Physiology (Boron & Boulpaep); Costanzo Physiology 7th Ed.; Frameworks for Internal Medicine; Goldman-Cecil Medicine; Comprehensive Clinical Nephrology 7th Ed.; Fishman's Pulmonary Diseases and Disorders; Harrison's Principles of Internal Medicine 22E; Rosen's Emergency Medicine
Can u remove those dollar symbol and give answer
Alveolar-Arterial (A-a) Gradient - Complete Answer for MD Exams
Definition
The Alveolar-Arterial (A-a) oxygen gradient is the difference between the partial pressure of oxygen in the alveolus (PAO2) and the partial pressure of oxygen in the systemic arterial blood (PaO2).
A-a gradient = PAO2 - PaO2
It is the single most useful index for evaluating the efficiency of oxygen transfer across the lung. A normal lung has minimal difference between alveolar and arterial PO2; when this gradient widens, it signals a defect in O2 equilibration between alveolar gas and pulmonary capillary blood.
The Alveolar Gas Equation (Essential for Calculating PAO2)
PAO2 cannot be measured directly - it is calculated using the Alveolar Gas Equation:
PAO2 = FiO2 x (PB - PH2O) - (PaCO2 / R)
Where:
- FiO2 = fraction of inspired oxygen (0.21 on room air)
- PB = barometric pressure (760 mm Hg at sea level)
- PH2O = water vapor pressure at body temperature (47 mm Hg)
- PaCO2 = arterial CO2 tension (assumed equal to alveolar CO2 = 40 mm Hg normally)
- R = respiratory quotient (0.8 on a mixed diet)
At sea level on room air - simplified form:
PAO2 = 150 - (PaCO2 / 0.8) = 150 - (1.25 x PaCO2)
With normal PaCO2 of 40 mm Hg:
PAO2 = (0.21 x [760 - 47]) - (40 / 0.8) = ~100 mm Hg
Therefore:
A-a gradient = PAO2 - PaO2 = 100 - 95 = ~5 mm Hg (normal)
Normal Values
| Age (years) | Upper limit of normal A-a gradient (mm Hg) |
|---|---|
| 20 | 17 |
| 30 | 20 |
| 40 | 23 |
| 50 | 26 |
| 60 | 30 |
| 70+ | ~35 |
General rule for upper limit of normal:
Normal A-a gradient = (Age + 10) / 4
Range at rest on room air: 5-15 mm Hg (young adults), up to 25 mm Hg (elderly).
Important: Normal A-a gradient increases with:
- Age - due to progressive V/Q mismatch from loss of lung elasticity
- Increasing FiO2 - breathing supplemental O2 widens the measurable gradient
Physiological Basis - Why Does a Normal A-a Gradient Exist?
Even in healthy lungs, a small A-a gradient of 5-15 mm Hg exists because of:
- Physiological V/Q mismatch - ventilation and perfusion are not perfectly matched throughout the lung (apex vs. base differences)
- Anatomic shunts - bronchial veins and Thebesian veins drain directly into the left side of the circulation, bypassing alveolar gas exchange (~2-3% of cardiac output)
- Diffusion limitation - minimal at rest but becomes relevant in disease
Classification of Hypoxemia by A-a Gradient
A. Hypoxemia with NORMAL A-a Gradient
The lung is intrinsically normal - the problem is insufficient inspired O2 or reduced alveolar ventilation. O2 equilibrates normally across the alveolar-capillary membrane, so PAO2 and PaO2 fall together.
| Mechanism | Explanation | Examples |
|---|---|---|
| Reduced PiO2 | Decreased FiO2 or decreased barometric pressure reduces both alveolar and arterial PO2 equally | High altitude, smoke inhalation, suffocation |
| Hypoventilation | Less fresh air enters alveoli per breath; CO2 accumulates and displaces O2. Equilibration is intact so PaO2 falls equally. PaCO2 is elevated | Opioid/sedative overdose, neuromuscular disease, sleep apnea, obesity hypoventilation syndrome, mechanical obstruction, metabolic alkalosis |
Key feature: Both conditions respond well to supplemental O2.
B. Hypoxemia with ELEVATED (Widened) A-a Gradient
The lung itself is diseased - O2 does not equilibrate fully across the alveolar-capillary barrier. PaO2 falls disproportionately compared to PAO2.
1. V/Q Mismatch (Most Common Cause)
- Ventilation and perfusion are mismatched in different lung regions
- Low V/Q regions (perfusion > ventilation): blood passes alveoli with low O2 tension - poorly oxygenated blood enters systemic circulation
- High V/Q regions (dead space physiology): wasted ventilation
- The admixture of blood from low V/Q regions drags down overall PaO2
- Examples: COPD, asthma, pneumonia, pulmonary embolism
- Responds to supplemental O2
2. Right-to-Left Shunt
- Deoxygenated blood bypasses ventilated alveoli entirely (V/Q = 0)
- Anatomic shunt: ASD with reversed shunt, VSD, pulmonary AVM, hepatopulmonary syndrome
- Physiologic shunt: lobar pneumonia, complete atelectasis, ARDS (flooded/collapsed alveoli)
- Hallmark: PaO2 does NOT improve significantly with 100% O2 - this distinguishes shunt from all other causes. Even breathing 100% O2, shunted blood remains unoxygenated and mixes with oxygenated blood, limiting the PaO2 rise
3. Diffusion Impairment
- Thickening of the alveolar-capillary membrane increases diffusion distance, reducing O2 transfer
- O2 does not fully equilibrate across the membrane before blood exits the capillary
- Examples: interstitial pulmonary fibrosis, pulmonary edema, sarcoidosis
- Responds to supplemental O2 (raising driving force for diffusion)
4. Increased Dead Space (V/Q mismatch subtype)
- Pulmonary embolism is the classic example: normal ventilation with no perfusion (V/Q = infinity)
- Embolized lung contributes to dead space; remaining vascular bed receives excess perfusion, creating V/Q mismatch in adjacent lung regions
- Results in widened A-a gradient plus hypocapnia (compensatory hyperventilation)
Summary Table: A-a Gradient in Different Causes of Hypoxemia
| Mechanism | PaO2 | PaCO2 | A-a Gradient | Response to O2 |
|---|---|---|---|---|
| High altitude | Low | Normal or low | Normal | Yes |
| Hypoventilation | Low | High | Normal | Yes |
| V/Q mismatch | Low | Normal or low | Increased | Yes |
| Diffusion defect | Low | Normal | Increased | Yes |
| Right-to-left shunt | Low | Normal or low | Increased | Limited |
Clinical Uses of the A-a Gradient
1. Differentiating Causes of Hypoxemia
The primary clinical use. A normal A-a gradient immediately localizes the problem to hypoventilation or reduced inspired O2, sparing the need for extensive lung workup.
2. Diagnosing Pulmonary Embolism
- PE causes a widened A-a gradient from dead space V/Q mismatch and often hypocapnia
- ABG showing hypoxemia + respiratory alkalosis + widened A-a gradient raises suspicion for PE
- However, a normal A-a gradient does not exclude PE (can be normal in a minority of cases)
3. Assessing Severity of Lung Disease
- The magnitude of gradient widening reflects the degree of V/Q mismatch
- Used in ICU for serial monitoring - tracks progression or improvement in ARDS, pneumonia, respiratory failure
- In mild pulmonary disease: A-a gradient < 35 mm Hg; in severe disease: > 35 mm Hg (e.g., Pneumocystis pneumonia severity grading)
4. Distinguishing Shunt from Other Causes (100% O2 Test)
- If PaO2 rises to >400-500 mm Hg on 100% O2, there is no significant shunt
- If PaO2 remains low despite 100% O2, an anatomic or physiologic shunt is present
5. Detecting Occult Lung Disease
- A widened A-a gradient on ABG in a patient with normal spirometry suggests underlying parenchymal or vascular disease
Worked Numerical Examples (High-Yield for Exams)
Case 1 - Hypoventilation (e.g., opioid overdose):
- PaO2 = 70, PaCO2 = 60 on room air
- PAO2 = 150 - (1.25 x 60) = 150 - 75 = 75 mm Hg
- A-a gradient = 75 - 70 = 5 mm Hg → Normal
- Interpretation: pure hypoventilation; lungs are intrinsically normal
Case 2 - V/Q Mismatch (e.g., pneumonia):
- PaO2 = 70, PaCO2 = 40 on room air
- PAO2 = 150 - (1.25 x 40) = 150 - 50 = 100 mm Hg
- A-a gradient = 100 - 70 = 30 mm Hg → Widened
- Interpretation: lung parenchymal/vascular disease
Factors That Affect the A-a Gradient
| Factor | Effect on A-a Gradient |
|---|---|
| Increasing age | Increases |
| Increasing FiO2 | Increases |
| Exercise | Slightly increases |
| Supine position | Decreases (more uniform perfusion) |
| Obesity | Increases |
Key Points to Remember for MD Exams
- Formula: A-a gradient = PAO2 - PaO2; PAO2 is calculated, PaO2 is measured on ABG
- Normal: 5-15 mm Hg (young adult); upper limit = (Age + 10) / 4
- Normal A-a gradient + hypoxemia = hypoventilation or reduced PiO2 (lung is healthy)
- Widened A-a gradient + hypoxemia = V/Q mismatch, shunt, or diffusion defect (lung is diseased)
- Failure to correct with 100% O2 is pathognomonic of right-to-left shunt
- V/Q mismatch is the most common cause of widened A-a gradient in clinical practice
- In pure hypoventilation, PaCO2 is always elevated
- Hepatopulmonary syndrome widens the A-a gradient via intrapulmonary vasodilation (diffusion-perfusion impairment)
Sources: Medical Physiology (Boron & Boulpaep); Costanzo Physiology 7th Ed.; Frameworks for Internal Medicine; Goldman-Cecil Medicine; Comprehensive Clinical Nephrology 7th Ed.; Fishman's Pulmonary Diseases and Disorders; Harrison's Principles of Internal Medicine 22E
This is a shared conversation. Sign in to Orris to start your own chat.