Highlight the contrast in parameters of PFT between obstructive and restrictive conditions for 10 marks
Reading File
Finding Sources
Finding Sources
Reading File
Reading File
Reading File
Reading File
Finding Sources
Finding Sources
Reading File
Reading File
Loading Image
Reading File
I now have all the information needed to write a thorough, exam-quality answer. Let me compose the full 10-mark response:
Pulmonary Function Tests (PFT): Obstructive vs. Restrictive Conditions
Introduction
Pulmonary function tests (PFTs) quantify ventilatory capacity and gas exchange and are essential to classify lung disease. The two principal patterns are obstructive (impaired airflow) and restrictive (reduced lung volumes). Understanding the contrast in each PFT parameter is critical for diagnosis and management.
Key PFT Parameters at a Glance
| Parameter | Obstructive | Restrictive |
|---|---|---|
| FEV1 | Decreased | Decreased |
| FVC | Normal or decreased | Decreased |
| FEV1/FVC ratio | Decreased (<0.70) | Normal or increased (>0.70) |
| TLC | Normal or increased | Decreased |
| RV | Increased (air trapping) | Decreased (parenchymal) or N/increased (NM) |
| FRC | Increased | Decreased |
| RV/TLC ratio | Increased | Normal or increased (NM disease) |
| FEF25-75% | Decreased (early small airway disease) | Normal or proportionally reduced |
| DLCO | Normal or decreased (emphysema ↓↓) | Decreased (parenchymal) or normal (extra-parenchymal) |
| Airway resistance (RAW) | Increased | Normal |
| Lung elastic recoil | Decreased (emphysema) | Increased (fibrosis) |
| Flow-volume curve shape | Concave upward (scooped) expiratory limb | Convex upward (steep, vertically oriented) expiratory limb; reduced total width |
| Bronchodilator response | Often positive (≥12% and 200 mL rise in FEV1/FVC) | Absent |
1. FEV1/FVC Ratio - The Pivotal Discriminator
This is the single most important distinguishing parameter.
- Obstructive: FEV1/FVC is reduced below 0.70 (ATS/ERS criterion). Airflow limitation means FEV1 falls disproportionately more than FVC.
- Restrictive: FEV1/FVC is normal or elevated (often >0.80). Both FEV1 and FVC are reduced, but FVC falls more (or proportionately), so the ratio is preserved or rises. In parenchymal restriction (e.g., pulmonary fibrosis), increased elastic recoil actually boosts expiratory flow, causing a disproportionately smaller drop in FEV1.
Murray & Nadel's Textbook of Respiratory Medicine notes: "In true parenchymal restriction, the high FEV1/FVC ratio arises from the reduction in FVC and the disproportionately lower decrease in FEV1 due to a high lung elastic recoil."
2. Lung Volumes (TLC, RV, FRC)
Obstructive
- TLC: Normal or increased due to air trapping and loss of elastic recoil (most marked in emphysema).
- RV: Markedly increased - the classic hallmark. Air trapping prevents full exhalation.
- FRC: Increased - resting lung volume shifts upward.
- RV/TLC ratio: Elevated, indicating a high proportion of the lung is occupied by trapped gas.
Restrictive
- TLC: Reduced - the defining criterion for true restriction. Confirmed by body plethysmography or gas dilution.
- RV: Reduced in parenchymal restriction (fibrosis, inflammation). Normal or even increased in neuromuscular disease or chest wall restriction (inability to fully exhale against a stiff chest wall).
- FRC: Reduced in parenchymal and most chest wall restriction.
Fishman's Pulmonary Diseases and Disorders states: "Typically, all three lung volumes - RV, FRC, and TLC - are increased" in obstruction; while restriction shows "reduced TLC and RV indicative of reduced compliance."
3. DLCO (Diffusing Capacity for Carbon Monoxide)
DLCO reflects the gas-transfer surface area and is a powerful differentiator within each pattern.
| Condition | DLCO |
|---|---|
| COPD - chronic bronchitis | Normal or mildly reduced |
| Emphysema | Markedly reduced (loss of alveolar-capillary surface) |
| Asthma | Normal (or even elevated) |
| Pulmonary fibrosis (restrictive) | Reduced (membrane thickening + volume loss) |
| Chest wall restriction (obesity, kyphoscoliosis) | Normal (gas transfer membrane intact) |
| Neuromuscular restriction | Normal or mildly reduced |
| Pulmonary embolism | Reduced (often with otherwise near-normal volumes) |
Symptom to Diagnosis summarizes: "DLCO ↓ in COPD (if emphysema); DLCO ↓ in interstitial restriction; DLCO WNL in chest wall restriction."
4. Flow Rates: FEF25-75% and Peak Flow
- Obstructive: FEF25-75% (mid-expiratory flow) is the most sensitive early indicator of small airway disease. It is disproportionately reduced before FEV1 falls. Peak expiratory flow (PEF) is also reduced.
- Restrictive: FEF25-75% is reduced proportionally with the overall reduction in lung volumes, not disproportionately. When corrected for lung volume (FVC), it is often normal or even supranormal in parenchymal fibrosis due to increased elastic recoil.
5. Flow-Volume Curve Shape
This is a visually powerful contrast:
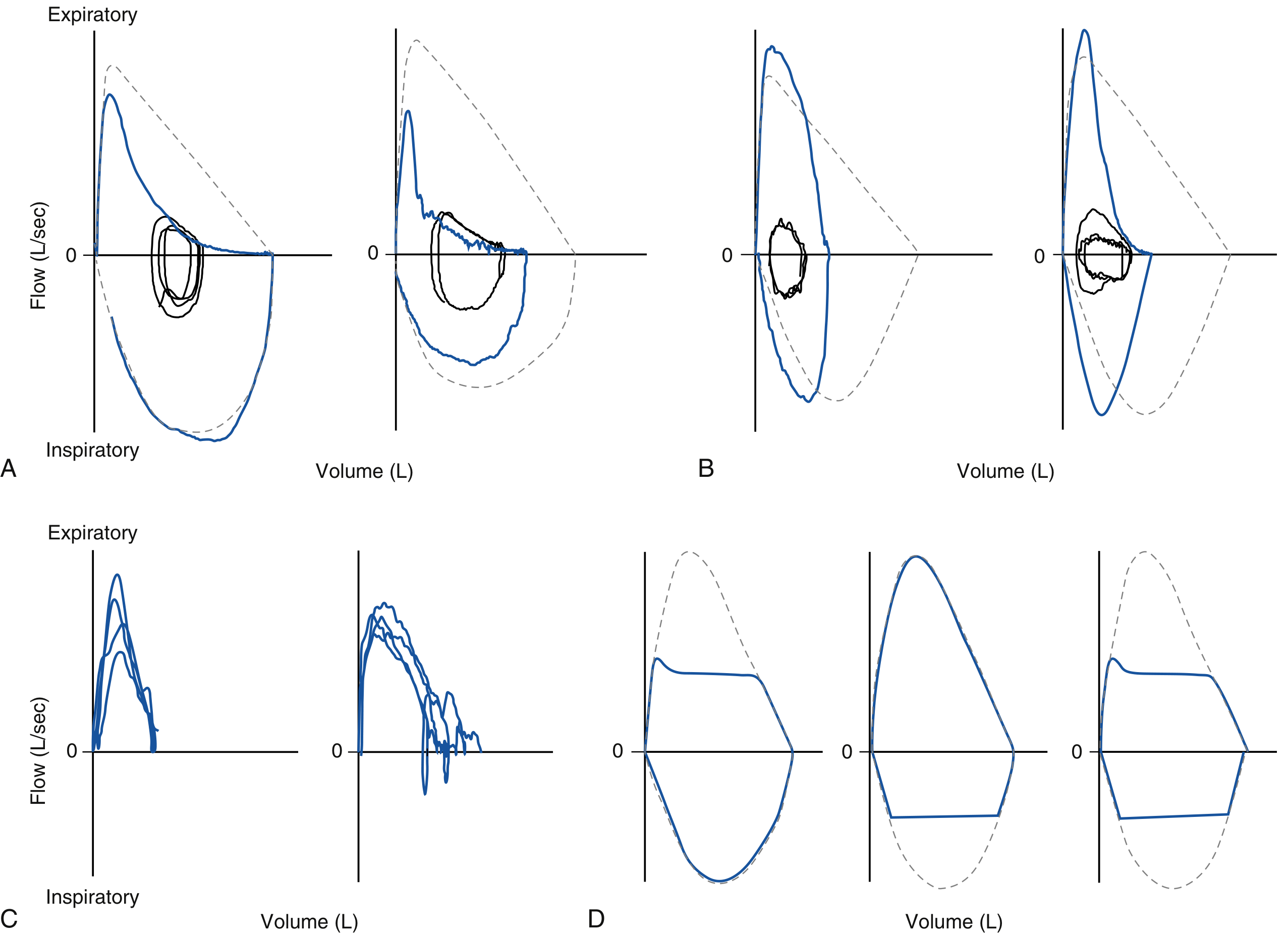
Figure: Typical flow-volume curves (Murray & Nadel's). A = COPD - scooped/concave-upward expiratory limb showing obstruction. B = ILD (restrictive) - convex-upward, steep expiratory limb with reduced total width.
- Obstructive: Expiratory limb is concave upward (scooped). Flow at low lung volumes is disproportionately reduced. The curve is wide but depressed.
- Restrictive: Expiratory limb is convex upward (steep, tall, narrow). The entire curve is shifted to a smaller volume, but peak flow may be relatively preserved or even increased (especially in fibrosis where recoil is high).
6. Airway Resistance (RAW)
- Obstructive: RAW is increased due to narrowed airways (mucus, bronchoconstriction, loss of radial traction in emphysema).
- Restrictive: RAW is normal - the airways themselves are not narrowed.
7. Bronchodilator Reversibility
- Obstructive (asthma): Significant reversibility - FEV1 or FVC increases by ≥12% and ≥200 mL after a bronchodilator.
- Obstructive (COPD): Variable, often limited reversibility.
- Restrictive: No significant bronchodilator response - obstruction is not the mechanism.
8. Severity Grading
According to ATS/ERS guidelines, severity in both obstructive and restrictive patterns is graded by FEV1 % predicted:
| Severity | FEV1 % Predicted |
|---|---|
| Mild | >70% |
| Moderate | 60-69% |
| Moderately Severe | 50-59% |
| Severe | 35-49% |
| Very Severe | <35% |
9. Special Patterns Within Restrictive Disease
| Type | TLC | RV | DLCO | FEV1/FVC |
|---|---|---|---|---|
| Parenchymal (fibrosis) | ↓ | ↓ | ↓↓ | N/↑ |
| Chest wall (obesity, pleural) | ↓ | N | Normal | N |
| Neuromuscular | ↓ | N/↑ | Normal/↓ | N |
Neuromuscular restriction uniquely shows an elevated RV/TLC ratio (due to expiratory muscle weakness) and a reduced MVV and NIF (negative inspiratory force).
10. Mixed Pattern
When both FEV1/FVC is reduced AND TLC is reduced, a mixed obstructive-restrictive pattern is diagnosed. This occurs in diseases like bronchiectasis with fibrosis, or sarcoidosis.
Summary Table
| Parameter | Obstructive | Restrictive (Parenchymal) | Restrictive (Extra-parenchymal) |
|---|---|---|---|
| FEV1 | ↓ | ↓ | ↓ |
| FVC | N or ↓ | ↓ | ↓ |
| FEV1/FVC | ↓ (<0.70) | N/↑ | N/↑ |
| TLC | N/↑ | ↓↓ | ↓ |
| RV | ↑↑ | ↓ | N/↑ |
| FRC | ↑ | ↓ | ↓ |
| DLCO | N/↓ (↓↓ emphysema) | ↓↓ | N |
| RAW | ↑ | N | N |
| FEF25-75% | ↓↓ | Proportionally ↓ | Proportionally ↓ |
| Bronchodilator | +ve (asthma) | -ve | -ve |
| Flow-volume curve | Concave (scooped) | Convex (steep, narrow) | Narrow, near-normal shape |
Sources: Murray & Nadel's Textbook of Respiratory Medicine; Fishman's Pulmonary Diseases and Disorders; Symptom to Diagnosis (4th ed.); Swanson's Family Medicine Review.
This is a shared conversation. Sign in to Orris to start your own chat.