À 52 year old women have back pain
Reading File
Finding Sources
Finding Sources
Reading File
Reading File
Finding Sources
Reading File
Reading File
Finding Sources
Loading Image
Finding Sources
Finding Sources
Reading File
Finding Sources
I now have a solid foundation to give a comprehensive, structured clinical answer. Let me compile the response.
Back Pain in a 52-Year-Old Woman - Clinical Approach
Key Context: Why Age and Sex Matter
At 52, this woman is likely perimenopausal or early postmenopausal, which shifts the differential toward estrogen-deficient conditions (osteoporosis, compression fractures) alongside the usual mechanical causes. The evaluation must consider this biological context.
Differential Diagnosis
The vast majority of low back pain (97%) is mechanical. The diagram below from Goldman-Cecil Medicine illustrates the full differential:
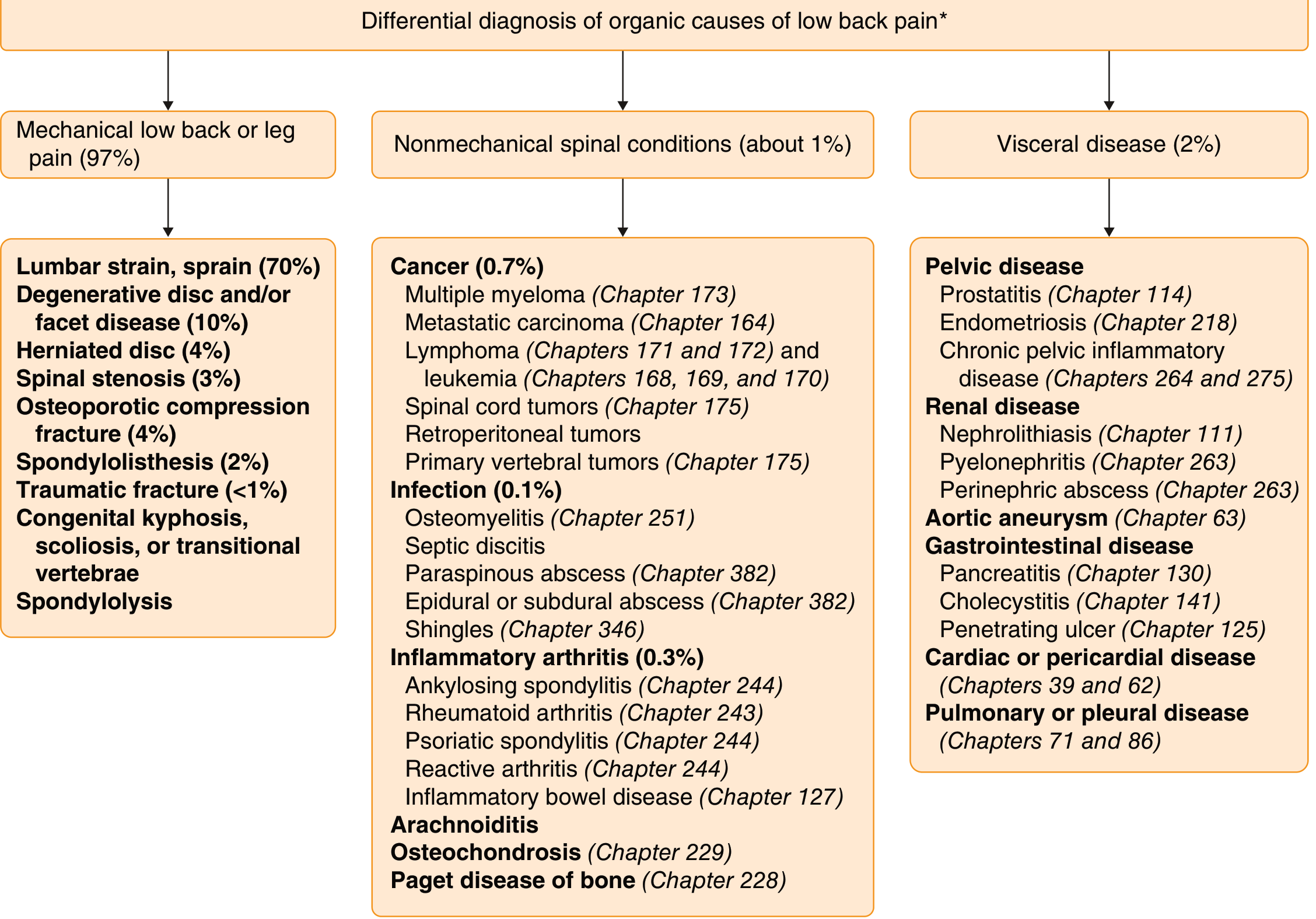
1. Mechanical Causes (97%)
| Cause | Notes |
|---|---|
| Lumbar strain/sprain (70%) | Most common; acute onset after activity |
| Degenerative disc/facet disease (10%) | Insidious onset, worse with activity |
| Herniated disc (4%) | May radiate to leg (sciatica) |
| Osteoporotic compression fracture (4%) | Very relevant at 52 - often triggered by minor trauma (cough, sneeze) |
| Spinal stenosis (3%) | Neurogenic claudication (pain with walking, relieved by sitting) |
| Spondylolisthesis (2%) |
2. Nonmechanical Spinal Conditions (~1%)
- Cancer: multiple myeloma, metastatic carcinoma, lymphoma, primary vertebral tumor
- Infection: vertebral osteomyelitis, septic discitis, epidural abscess
- Inflammatory arthritis: ankylosing spondylitis, psoriatic spondylitis, reactive arthritis
3. Visceral Referred Pain (~2%) - Especially Relevant in Women
- Pelvic disease: endometriosis, pelvic inflammatory disease, ovarian pathology
- Renal disease: nephrolithiasis (colicky flank pain), pyelonephritis
- Gastrointestinal: pancreatitis (L1 level), cholecystitis (mid-thoracic)
- Abdominal aortic aneurysm: mid/low back pain radiating to hips - do not miss!
- Goldman-Cecil Medicine, p. 3841
Red Flags - Must Not Miss
Ask about and assess for "red flags" that signal a serious underlying cause:
| Red Flag | Suggests |
|---|---|
| Age >50 + no trauma + osteoporosis risk | Vertebral compression fracture |
| History of cancer | Metastatic disease |
| Unexplained weight loss, night sweats, fever | Malignancy or infection |
| Pain worse at night / not relieved lying down | Cancer, infection |
| Bowel/bladder dysfunction, saddle anesthesia | Cauda equina syndrome (emergency) |
| Bilateral leg weakness or numbness | Spinal cord compression |
| IV drug use, immunocompromise | Epidural abscess, osteomyelitis |
| Pulsatile abdominal mass | Abdominal aortic aneurysm |
- Tintinalli's Emergency Medicine; Goldman-Cecil Medicine
Osteoporosis/Vertebral Compression Fracture - Priority at Age 52
At 52 with potential perimenopause, osteoporotic vertebral compression fracture (VCF) deserves special attention:
- Most are asymptomatic and found incidentally; only ~30% present with sudden-onset pain
- Pain can be triggered by a minor event (cough, sneeze, mild lift)
- Most common site: thoracolumbar junction
- Physical exam may show localized vertebral tenderness and increased kyphosis
- Neurologic exam should be normal in uncomplicated VCF
Fractures above T7 in a patient without known osteoporosis should prompt workup for systemic disease (malignancy, hyperparathyroidism, osteomalacia, TB).
- Textbook of Family Medicine 9e, p. 858-859
Initial Evaluation
History
- Duration, onset (acute vs. insidious), character, radiation
- Aggravating/relieving factors (worse with movement? worse lying down at night?)
- Menstrual status, steroid use, prior fractures (osteoporosis risk factors)
- History of cancer, IV drug use, recent infection
- Bowel/bladder changes
Physical Exam
- Straight leg raise (nerve root compression)
- Neurologic: motor strength, reflexes, sensation
- Palpation for midline vertebral tenderness
- Abdominal exam (AAA)
- Costovertebral angle tenderness (renal)
Imaging
- Plain X-ray: first-line if fracture or structural cause suspected
- MRI: preferred for neurologic symptoms, suspected infection, malignancy, or failed conservative therapy after 4-6 weeks
- DEXA scan: bone mineral density in perimenopausal women with VCF risk
Labs (if red flags present)
- CBC, ESR, CRP (infection/malignancy)
- Serum calcium, PTH, vitamin D (metabolic bone disease)
- Urinalysis (renal cause)
- PSA not applicable here; consider tumor markers if cancer is suspected
Management Overview
Without red flags (mechanical LBP - the majority):
- Reassurance: most acute LBP resolves within 4-6 weeks
- NSAIDs (first-line): ibuprofen, naproxen - use with caution if GI/renal history
- Acetaminophen: second-line analgesic
- Early mobilization: bed rest is not recommended; stay active
- Physical therapy: especially for subacute/chronic pain
- Muscle relaxants: short-term for acute spasm
- Avoid opioids: first-line only if other measures fail; carry addiction risk
For osteoporotic VCF:
- Pain control (NSAIDs ± short-term opioids)
- Bisphosphonates or other bone-protective therapy to prevent future fractures
- Calcium + Vitamin D supplementation
- Fall prevention
- Kyphoplasty/vertebroplasty for refractory severe pain
Refer urgently if any red flags are present, especially cauda equina symptoms (emergency surgery).
- Goldman-Cecil Medicine; Textbook of Family Medicine 9e; Bradley and Daroff's Neurology
Summary
A structured approach for this 52-year-old woman with back pain:
- Screen for red flags first - rule out emergency (cauda equina, AAA, malignancy, infection)
- Consider osteoporotic VCF given her age and likely perimenopausal status
- Think about referred pelvic/renal pain unique to women
- Most likely diagnosis is still mechanical LBP - manage conservatively
- Image and investigate if red flags present or pain persists beyond 4-6 weeks without improvement
Enzoflam should i give
Reading File
Searching the Web
Enzoflam tablet composition diclofenac paracetamol serratiopeptidase uses dosage
Finding Sources
Finding Sources
Reading Web Page
https://www.1mg.com/drugs/enzoflam-tablet-64343
Finding Sources
Finding Sources
Finding Sources
Finding Sources
Finding Sources
Reading File
Finding Sources
Here is a complete clinical breakdown of Enzoflam for this patient:
Enzoflam for Back Pain in a 52-Year-Old Woman
What is Enzoflam?
Enzoflam is a combination tablet containing three drugs:
| Component | Dose | Role |
|---|---|---|
| Diclofenac Sodium | 50 mg | NSAID - reduces pain and inflammation |
| Paracetamol (Acetaminophen) | 325 mg | Analgesic/antipyretic |
| Serratiopeptidase | 15 mg | Proteolytic enzyme - reduces swelling and edema |
Is it Appropriate for This Patient?
Yes, Enzoflam is a reasonable choice for mechanical back pain (musculoskeletal strain, disc disease, facet arthritis) in this 52-year-old - but only after screening for contraindications.
NSAIDs like diclofenac are first-line for acute back pain. As stated in Adams and Victor's Principles of Neurology: "Nonsteroidal anti-inflammatory drugs (NSAIDs) may be given liberally during the first few days unless there are contraindications to these agents."
Before Prescribing - Screen for Contraindications
Absolute contraindications (do NOT give):
- Active peptic ulcer disease or GI bleeding
- Known allergy to diclofenac or any NSAID
- Severe renal impairment (eGFR < 30)
- Severe hepatic failure
- Post-CABG surgery (within 10-14 days)
- Severe uncontrolled heart failure
- Known hypersensitivity to aspirin (aspirin-exacerbated respiratory disease)
- Use of another NSAID simultaneously
Relative cautions (use with care):
- Hypertension - NSAIDs can raise BP and reduce antihypertensive efficacy
- Cardiovascular disease - diclofenac has a higher cardiovascular risk among NSAIDs (raises MI risk at higher doses/longer use)
- Renal impairment - even mild CKD warrants caution
- Asthma - aspirin-sensitive asthma
- Elderly/frail - start low, short course
- Concurrent anticoagulants (warfarin, heparin) - increased bleeding risk
Dosage
- 1 tablet, 2-3 times daily with food
- Maximum duration: 5-7 days for acute pain; avoid prolonged use
- Always take after meals - diclofenac is highly gastrotoxic on an empty stomach
Key Points for a 52-Year-Old Woman
- Add a gastric protector: Given her age, a PPI (e.g., omeprazole 20 mg OD) or at least misoprostol should be co-prescribed to protect against NSAID-induced gastric ulcers
- Check BP: NSAIDs can elevate blood pressure, especially if she has pre-existing hypertension
- Osteoporosis suspicion: If a vertebral compression fracture is the cause, NSAIDs help pain but she also needs bone protective therapy (bisphosphonate, calcium, Vitamin D)
- Short course only: 5-7 days maximum; long-term NSAID use is hazardous
- No double-dosing: Do not combine with other NSAIDs or high-dose aspirin
Side Effects to Warn About
| System | Side Effect |
|---|---|
| GI | Nausea, vomiting, heartburn, epigastric pain, peptic ulcer, GI bleed |
| Renal | Fluid retention, worsening of renal function |
| Cardiovascular | Edema, BP elevation, increased MI/stroke risk (long-term) |
| Hepatic | Elevated liver enzymes (rare) |
| CNS | Headache, dizziness |
| Skin | Rash, rarely Stevens-Johnson syndrome |
Bottom Line
Yes, give Enzoflam if no contraindications are present - it is appropriate for acute mechanical back pain in this patient. Give it:
- With food (after meals)
- With a PPI (omeprazole 20 mg) as GI protection
- For a short course (5-7 days)
- Reassess at follow-up - if pain persists beyond 4-6 weeks or red flags develop, image the spine (X-ray/MRI) and do not continue NSAIDs long-term
This is a shared conversation. Sign in to Orris to start your own chat.