Please teach me about the facial nerve, ENT, its pathophysiology, and also Ramsay Hunt disease, Bell's palsy, and other diseases related to ENT aspect of facial nerve.
Reading File
Finding Sources
Finding Sources
Finding Sources
Searching PubMed
"facial nerve" AND "Bell palsy" AND management
Reading File
Reading File
Reading File
Reading File
Reading File
Finding Sources
Finding Sources
Finding Sources
Reading File
Finding Sources
Searching Images
facial nerve anatomy segments temporal bone
Reading File
Finding Sources
Searching Images
Bell's palsy Ramsay Hunt syndrome herpes zoster oticus facial nerve
Reading File
Reading File
Loading Image
Loading Image
Reading File
I now have comprehensive information from Cummings to write a thorough response. Let me compile everything into a detailed, well-structured answer.
The Facial Nerve (CN VII): ENT Perspective
Primary source: Cummings Otolaryngology Head and Neck Surgery
1. Anatomy and Course
The facial nerve is a mixed nerve derived from the second branchial arch, carrying five functional fiber types:
| Fiber Type | Function |
|---|---|
| Special visceral efferent (SVE) | Motor to muscles of facial expression, stapedius, stylohyoid, posterior digastric |
| General visceral efferent (GVE) | Parasympathetic to lacrimal, nasal glands (via GSPN → pterygopalatine ganglion), and submandibular/sublingual glands (via chorda tympani → submandibular ganglion) |
| Special sensory (SVA) | Taste to anterior 2/3 of tongue (chorda tympani), palate and tonsil (GSPN) |
| General somatic afferent (GSA) | Touch sensation from EAC and conchal skin |
| Visceral afferent | Mucosa of nose, pharynx, palate |
Brainstem nuclei: motor nucleus (SVE), superior salivary nucleus (GVE), nucleus of the solitary tract (SVA/VA).
Intratemporal Course — Segments of the Fallopian Canal
The nerve traverses the fallopian canal from the fundus of the internal auditory canal (IAC) to the stylomastoid foramen. There are four segments:
| Segment | Description | Surgical Landmark |
|---|---|---|
| Labyrinthine | First, shortest (3–5 mm), narrowest; travels superior to cochlea toward geniculate fossa. No epineurium here (most vulnerable!). | Bill's bar (vertical crest) |
| Geniculate ganglion | Houses cell bodies of sensory neurons; GSPN exits anteriorly (first genu); covered by thin, often dehiscent bone (~25% of cases). | Retrograde dissection of GSPN |
| Tympanic (horizontal) | Courses along medial wall of middle ear, superior to oval window; most common site of congenital dehiscence. | Cochleariform process, oval window |
| Mastoid (vertical) | From pyramidal eminence to stylomastoid foramen; chorda tympani branches here; most variable path. | Pyramidal eminence, short process of incus, lateral SCC |
After exiting the stylomastoid foramen, the nerve receives blood supply from the posterior auricular artery and enters the parotid gland to divide into temporal, zygomatic, buccal, marginal mandibular, and cervical branches (the pes anserinus).
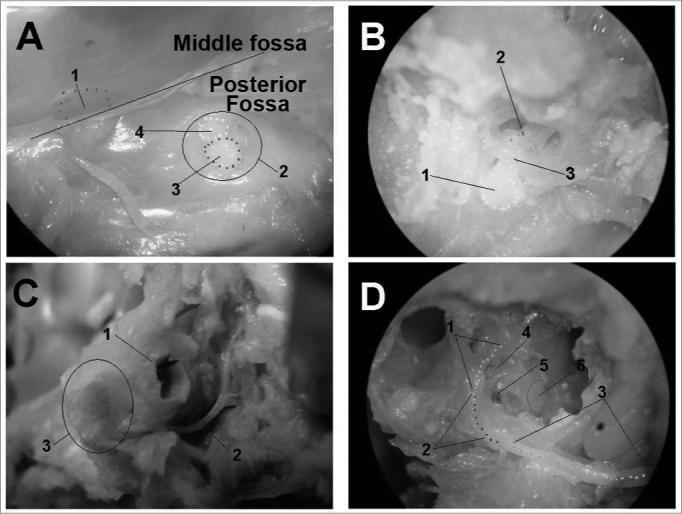
Cadaveric temporal bone dissection. Panel A: intracranial view; Panel B: internal acoustic meatus with labyrinthine segment; Panel C: extratemporal exit at stylomastoid foramen; Panel D: middle ear medial wall showing tympanic and mastoid segments, oval window, and promontory.
Key Vulnerabilities
| Segment | Why Vulnerable |
|---|---|
| Labyrinthine | Narrowest canal, no epineurium, watershed blood supply → edema after viral infection is maximally compressive here |
| Geniculate ganglion | Thin/dehiscent bone; tethered by GSPN (fracture traction); adjacent to STR |
| Tympanic | Most common site of dehiscence → exposed to suppurative OM toxins; cholesteatoma erodes here |
| Mastoid | Variable path, especially in congenital malformations; stylomastoid foramen superficial in neonates → forceps injury |
2. Grading Facial Nerve Dysfunction
The House-Brackmann (HB) Scale (1985) is the most widely accepted grading system:
| Grade | Description |
|---|---|
| I | Normal function |
| II | Slight weakness, complete eye closure with effort, slight mouth asymmetry |
| III | Obvious asymmetry; complete eye closure with effort; HB "moderate dysfunction" |
| IV | Obvious disfiguring asymmetry; incomplete eye closure |
| V | Barely perceptible movement |
| VI | Complete paralysis |
3. Electrodiagnostic Testing
- Electroneurography (ENoG): Measures amplitude of compound action potential (CAP). Degeneration >90% = poor prognosis. Useful from day 3 onward (requires Wallerian degeneration to reach facial surface).
- Electromyography (EMG): Detects voluntary motor units; fibrillation potentials appear 10–14 days after complete degeneration. Maintains prognostic value when ENoG is severely depressed.
- Combined ENoG + EMG: Patients with preserved voluntary EMG potentials despite low CAP have excellent prognoses.
- Salivary flow test: Reduced flow (<25% contralateral) or abnormal scintigraphy by day 14 predicts incomplete recovery.
4. Bell's Palsy
Definition
Acute idiopathic lower motor neuron (LMN) facial paralysis — the most common cause of peripheral facial palsy (~60–75% of cases).
Pathophysiology
Herpes simplex virus type 1 (HSV-1) is the primary implicated pathogen. Viral DNA has been isolated from endoneurial fluid and muscle of Bell's palsy patients. The proposed mechanism:
- Latent HSV-1 reactivates in the geniculate ganglion
- Viral replication triggers perineural inflammation and edema
- Because the labyrinthine segment is the narrowest and has no epineurium, swelling in this confined bony canal leads to ischemic compression
- Wallerian degeneration of varying severity follows
Clinical Features
- Sudden-onset unilateral LMN facial weakness (forehead involved — distinguishes from UMN palsy)
- Prodrome: retroauricular/mastoid pain
- Taste disturbance (chorda tympani involvement)
- Hyperacusis (stapedius involvement)
- Reduced lacrimation (GSPN involvement)
- Eye: incomplete closure → exposure keratopathy risk
Prognosis
- 80–90% recover completely without treatment
- Incomplete paralysis: 95–100% full recovery
- Complete paralysis: higher risk of sequelae (synkinesis, contracture, hemifacial spasm)
- Poor prognostic factors: complete paralysis, hyperacusis, decreased tearing, age >60, diabetes mellitus, hypertension, severe pain at onset
- Recovery by 6 months; if not, reconsider the diagnosis
Management
First-line: Corticosteroids
- Prednisone 1 mg/kg/day (up to 60–80 mg/day) × 10 days, initiated within 48–72 hours
- Meta-analyses show ~17% better chance of complete recovery vs placebo
- Reduces synkinesis and contracture
Antivirals (acyclovir/valacyclovir)
- Role is controversial; the American Academy of Neurology (2012) found antivirals add at most a modest (≤7%) additional benefit
- Some guidelines still recommend combining them with steroids in severe (HB IV–VI) palsy, particularly given the risk of missing zoster sine herpete
Eye care (mandatory)
- Lubricating drops, nocturnal taping/ointment, moisture chamber
- Ophthalmology referral for lagophthalmos
Surgical decompression
- Transmastoid decompression of tympanic/mastoid segments: abandoned — randomized trials showed no benefit; the lesion is in the proximal labyrinthine segment, inaccessible via this route
- Middle fossa approach decompression of the meatal foramen and labyrinthine segment in patients with ENoG >90% degeneration within 14 days: some evidence of benefit but difficult to accumulate sufficient trial data
5. Ramsay Hunt Syndrome (Herpes Zoster Oticus)
Definition
VZV reactivation in the geniculate ganglion causing the classic triad:
- Peripheral facial palsy (LMN, CN VII)
- Otalgia (severe ear pain)
- Vesicular eruption — on the auricle (concha, EAC), retroauricular area, face, or oral mucosa

Pathophysiology
After primary VZV infection (chickenpox), the virus becomes latent in dorsal root/extramedullary cranial nerve ganglia. Reactivation occurs during decreased cell-mediated immunity (aging, malignancy, immunosuppression). The geniculate ganglion is particularly susceptible (CN VII carries sensory fibers). Annual incidence: ~130/100,000; increases sharply after age 60.
Features Distinguishing from Bell's Palsy
| Feature | Bell's Palsy | Ramsay Hunt |
|---|---|---|
| Pathogen | HSV-1 | VZV |
| Vesicular rash | Absent | Present (ear, mouth) — may lag palsy by days |
| Severity | Milder | More severe |
| Complete recovery rate | 80–90% | Only 16–22% |
| Associated cranial nerve symptoms | Less common | More common (CN VIII: hearing loss, tinnitus, vertigo; hyperacusis) |
| Postherpetic neuralgia risk | Low | High — major complication |
Zoster Sine Herpete
~10% of Ramsay Hunt cases never develop visible vesicles ("zoster without rash") — diagnosed by rising VZV antibody titers. Important not to misclassify as Bell's palsy.
Ophthalmic Complications
Herpes zoster ophthalmicus (HZO) can co-occur: uveitis, keratoconjunctivitis, optic neuritis, glaucoma — associated with ophthalmic division of CN V involvement. Differentiate from HSV keratitis (topical steroids are used in HZO but contraindicated in HSV).
Management
- Corticosteroids (prednisone): relieve acute pain, reduce vertigo, decrease postherpetic neuralgia
- Acyclovir/valacyclovir: DNA polymerase inhibition, preferentially taken up by VZV-infected cells; started early (within 72 hours of rash onset)
- Combination therapy is standard
- Eye care mandatory (lagophthalmos risk)
- Vaccine (Shingrix) — highly recommended for prevention in >50 years old
6. Other ENT-Related Causes of Facial Nerve Palsy
Otitis Media — Acute (AOM)
- Facial palsy via congenital dehiscence of the fallopian canal adjacent to the stapes
- Management: systemic antibiotics + myringotomy; complete paralysis in AOM children rarely lasts >3 weeks
- AOM palsy is often incomplete
Chronic Otitis Media (COM) — Without Cholesteatoma
- Affects horizontal tympanic segment near stapes
- Gradual progression from mild weakness to full palsy
- Management: control the infection; surgical decompression if needed
Cholesteatoma
- Most common COM-related cause of facial palsy
- Erodes the horizontal fallopian canal (especially proximal to 2nd genu); can expose the nerve anywhere in the temporal bone
- Onset is typically gradual (slow progressive palsy over months)
- Management: mastoidectomy + careful dissection of cholesteatoma matrix from the nerve; outcomes depend on whether complete nerve degeneration has occurred before surgery (decompression within 1 week of onset significantly improves outcome)
Facial Nerve Tumors
Schwannoma (neuroma)
- Gradual-onset facial paresis + hearing loss (most common presentation)
- Expansile, smooth, enhancing mass along any segment of the fallopian canal on MRI
- HRCT shows enlargement of the bony facial canal
- Slowly progressive facial paralysis is NOT Bell's palsy — always suspect tumor
Hemangioma
- Usually at geniculate ganglion; honeycomb calcification on CT; early surgical intervention recommended to preserve nerve function
Perineural invasion of parotid malignancies
- Adenoid cystic carcinoma most notorious; facial weakness with parotid mass mandates imaging from parotid to brainstem
Traumatic Facial Paralysis
- Temporal bone fractures (most common intratemporal cause)
- Longitudinal fractures: often incomplete palsy, delayed onset → neurapraxia → good prognosis
- Transverse fractures: complete palsy, immediate onset → high risk of degeneration
- Penetrating injuries (gunshot)
- Iatrogenic: parotidectomy, mastoidectomy, middle fossa surgery
Lyme Disease (Borrelia burgdorferi)
- Most common infectious cause of bilateral facial palsy in endemic areas
- Can be unilateral; tested with serology; treated with doxycycline or amoxicillin
- Part of the workup for bilateral facial palsy
Malignancy/Neoplastic
- Parotid malignancies, squamous cell carcinoma of the temporal bone, metastases (breast, lung, kidney, prostate, melanoma)
- Progressive facial paralysis is the red flag for neoplasm
Bilateral Facial Palsy — Differential Diagnosis
Includes: Guillain-Barré syndrome, sarcoidosis (Heerfordt syndrome: parotid enlargement + iridocyclitis + CN palsy), Lyme disease, Bell's palsy, leukemia, syphilis, brainstem encephalitis, bacterial meningitis.
Melkersson-Rosenthal Syndrome
- Rare; triad of recurrent facial palsy + facial edema + fissured tongue (lingua plicata)
- Cause unknown; may respond to steroids
Möbius Syndrome
- Congenital bilateral CN VI and VII palsy; spectrum ranges to multiple CN palsies
- Evidence suggests rhombencephalon developmental disorder, not primary muscle defect
- Lower face often more spared than upper face
7. Localization of the Lesion by Clinical Findings
A fundamental ENT skill — the anatomical level of the lesion can be inferred from which branches are affected:
| Finding | Level of Lesion |
|---|---|
| Decreased lacrimation | Proximal to GSPN takeoff (geniculate ganglion or above) |
| Hyperacusis (stapedius affected) | Proximal to nerve to stapedius (mid-mastoid or above) |
| Taste loss (chorda tympani) | Proximal to chorda tympani origin (mastoid segment) |
| Facial palsy only (pure motor) | At/below stylomastoid foramen (e.g., parotid surgery) |
| UMN pattern (forehead spared) | Supranuclear — not a peripheral/ENT lesion |
8. Imaging
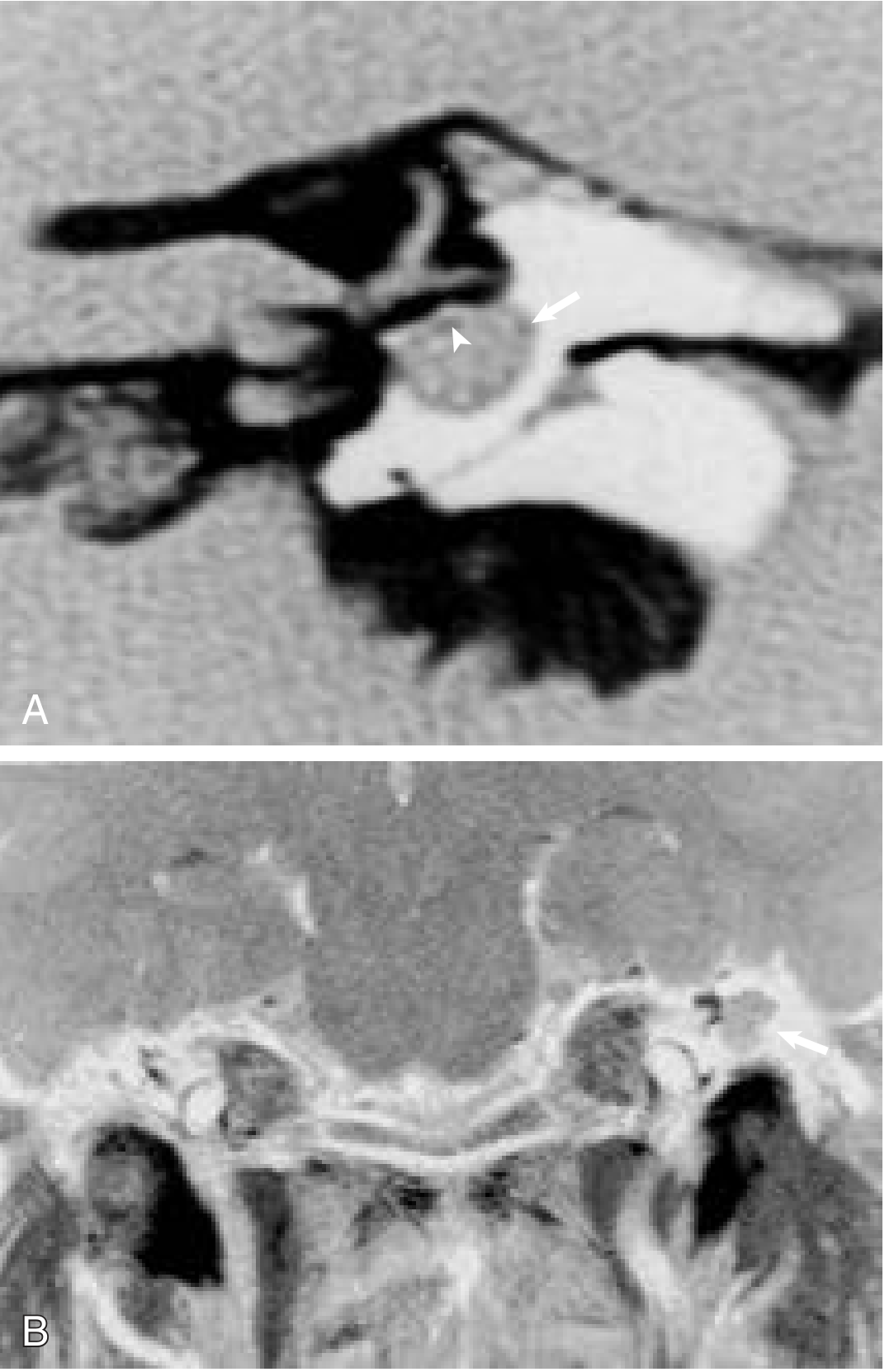
- MRI with gadolinium: Enhancement of the facial nerve is normal in healthy people; most consistent abnormal enhancement in Bell's/herpetic palsy is at the distal IAC and labyrinthine segment. MRI not routinely required for typical Bell's palsy — reserve for atypical presentations (recurrent ipsilateral palsy, twitching, no recovery by 6 months).
- HRCT temporal bone: Evaluates bony fallopian canal, cholesteatoma erosion, fracture lines, tumor-related canal expansion.
- Both modalities are complementary when evaluating facial nerve tumors — MRI from brainstem to parotid gland is required.
Summary Table: ENT Causes of Facial Palsy
| Cause | Key Feature | Onset | Treatment |
|---|---|---|---|
| Bell's palsy | Idiopathic, HSV-1 | Acute (<48h) | Steroids ± antivirals |
| Ramsay Hunt | VZV, auricular vesicles, severe | Acute | Steroids + acyclovir |
| AOM | Children, dehiscent canal | Acute | Antibiotics + myringotomy |
| COM/cholesteatoma | Gradual, chronic ear disease | Gradual | Mastoidectomy |
| Schwannoma | Gradual palsy + hearing loss | Insidious | Surgery |
| Trauma | Temporal bone fracture | Immediate/delayed | Observation/decompression |
| Lyme disease | Endemic area, bilateral possible | Subacute | Doxycycline |
| Malignancy (parotid/metastasis) | Progressive, parotid mass | Progressive | Per malignancy |
| Melkersson-Rosenthal | Recurrent, facial edema, fissured tongue | Recurrent | Steroids |
Sources: Cummings Otolaryngology Head and Neck Surgery (Chapters 126, 135, 141, 172) · Gray's Anatomy for Students · Bailey & Love's Short Practice of Surgery 28e
Recent evidence note (PMID 39627559, Sys Rev 2024): A systematic review of photobiomodulation therapy for Bell's palsy suggests potential benefit in symptom recovery, though the evidence base remains limited and this is not yet standard of care.
Teach me about evaluation of a deaf child from standard textbook for a 10 mark question in my final year university exam
Reading File
Finding Sources
Finding Sources
Finding Sources
Finding Sources
Finding Sources
Finding Sources
Finding Sources
Finding Sources
Finding Sources
Reading File
Reading File
You've run out of free credits. Sign up for a free account to continue using Orris.
This is a shared conversation. Sign in to Orris to start your own chat.