Give me all possible mechanism of itching and drugs targeting
Reading File
Finding Sources
Finding Sources
Searching PubMed
pruritus mechanisms pathophysiology treatment
Reading File
Reading File
Reading File
Reading File
Reading File
Finding Sources
Reading File
Finding Sources
Reading File
Finding Sources
Reading File
Searching the Web
pruritus itch mechanisms JAK inhibitors biologic treatments 2024 2025
Loading Image
I now have all the information needed to deliver a comprehensive, well-organized answer. Here it is:
Mechanisms of Itching (Pruritus) and Drugs Targeting Each
Classification of Itch Mechanisms
Pruritus is broadly classified into four mechanistic categories, with each having distinct mediators and drug targets.
1. Pruritoceptive (Peripheral) Itch
Itch arising from peripheral sensory nerve activation in the skin by chemical mediators.
1a. Histaminergic Pathway
- Activated mast cells release histamine, which binds H1 and H4 receptors on histamine-sensitive C fibers
- Activates TRPV1 (transient receptor potential vanilloid 1) channels → membrane depolarization → itch signal
- These C fibers have slow conduction velocities (0.3-1.0 m/s) and wide innervation territories
- Co-responsive to heat, explaining why warmth worsens itch
| Drug | Mechanism |
|---|---|
| Cetirizine, loratadine, fexofenadine (2nd-gen H1 antagonists) | Block H1 receptor on C fibers |
| Diphenhydramine, hydroxyzine (1st-gen H1 antagonists) | Block H1 receptor + central sedation |
| Clemizole | H4 receptor antagonist (investigational) |
Note: H1 antihistamines only work well for histaminergic itch (urticaria, insect bites). They are largely ineffective for most other pruritus types because non-histaminergic C fibers dominate those conditions.
1b. Non-Histaminergic Pathway - Protease-Activated Receptors (PARs)
- Proteases (tryptase, elastase, cathepsin S, cowhage mucinase) cleave and self-activate PAR-2 and PAR-4 receptors on C fiber terminals
- PAR-2/4 activation sensitizes TRPV1 and TRPA1 channels
- Relevant in atopic dermatitis, psoriasis, prurigo nodularis
| Drug | Mechanism |
|---|---|
| Capsaicin (topical) | Initial TRPV1 activation → desensitization and neuropeptide depletion |
| Topical anesthetics (lidocaine, pramoxine, benzocaine) | Block Na+ channels → inhibit C fiber conduction |
1c. MAS-Related G Protein-Coupled Receptors (MRGPRs)
- C fibers in the epidermis express MRGPRX1 (triggered by chloroquine and BAM8-22) and MRGPRX2 (activated by cathepsin S, cationic drugs - causes pseudo-allergic reactions)
- TRPA1 is the downstream transducer for MRGPR activation
| Drug | Mechanism |
|---|---|
| MRGPRX4 antagonists (preclinical) | Target bilirubin-induced itch in cholestasis |
1d. Cytokine / Interleukin-Mediated
- IL-31 (from Th2 cells) binds IL-31RA/OSMR heterodimer on C fibers and keratinocytes → TRPV1 activation → itch + barrier dysfunction; strongly implicated in atopic dermatitis
- IL-4 and IL-13 sensitize peripheral neurons and promote Th2 inflammation
- IL-33 directly stimulates sensory neurons (relevant in xerotic skin)
| Drug | Mechanism |
|---|---|
| Nemolizumab | Monoclonal Ab blocking IL-31RA; reduces itch in AD and prurigo nodularis |
| Dupilumab | Blocks IL-4Rα subunit shared by IL-4R and IL-13R; reduces neuronal sensitization and inflammation |
| Tralokinumab, lebrikizumab | Block IL-13 directly |
1e. Nerve Growth Factor (NGF) and Neurotrophin Pathway
- NGF (released by mast cells and keratinocytes, stimulated by histamine) activates TrkA (NTRK1) on C fibers
- Induces C fiber sprouting, increased substance P release, mast cell sensitization - amplifying the itch-scratch cycle
- Neurotrophin 4 (NT-4) similarly involved
| Drug | Mechanism |
|---|---|
| Anti-NGF antibodies (tanezumab, fasinumab - investigational) | Block NGF-TrkA signaling |
1f. Opioid Receptor Pathway (Peripheral)
- μ-opioid receptors (MOR) on peripheral nerves enhance itch when activated (e.g. by morphine, endorphins)
- κ-opioid receptors (KOR) on peripheral nerves counterbalance and inhibit itch
- Ratio of μ:κ opioid tone in the skin modulates itch threshold
| Drug | Mechanism |
|---|---|
| Nalfurafine (κ-opioid agonist) | Activates peripheral κ-opioid receptors → inhibits itch; approved in Japan for uremic pruritus |
| Difelikefalin (peripheral κ-opioid agonist) | FDA-approved for CKD-associated pruritus in dialysis patients |
2. Neuropathic Itch
Itch arising from disease or damage to afferent nerve fibers (peripheral or central).
Examples: brachioradial pruritus, post-herpetic pruritus, post-burn itch, multiple sclerosis-related itch, trigeminal trophic syndrome.
Mechanism: Abnormal neuronal firing, ectopic discharges, deafferentation sensitization, and loss of inhibitory interneuron control.
| Drug | Mechanism |
|---|---|
| Gabapentin, pregabalin | Bind α2-δ subunit of voltage-gated Ca2+ channels → reduce aberrant neuronal transmission |
| Carbamazepine | Blocks use-dependent Na+ channels and synaptic transmission |
| Topical anesthetics (EMLA, pramoxine) | Inhibit nerve conduction via decreased membrane Na+ permeability |
| Ketamine (topical/systemic) | NMDA receptor antagonist |
| Botulinum toxin A (intradermal) | Inhibits release of acetylcholine, glutamate, substance P, CGRP from nerve terminals |
| Capsaicin (high-concentration patch) | TRPV1-mediated neuropeptide depletion and nerve fiber desensitization |
| Cannabinoids (topical/systemic) | Modulate peripheral and central neuronal activity via CB1/CB2 receptors |
3. Neurogenic Itch
Itch originating from the nervous system without structural nerve damage; mediated by central opioidergic or serotonergic dysregulation.
Examples: cholestatic pruritus, renal pruritus, paraneoplastic itch.
Mechanisms:
- Opioid imbalance: increased central μ-opioid tone (excess endorphins/dynorphins in cholestasis and renal failure) without corresponding κ-opioid balance
- Lysophosphatidic acid (LPA): produced by autotaxin (elevated in cholestasis); direct neuronal activator - serum autotaxin levels correlate with itch intensity
- Serotonin (5-HT3): central serotonergic pathways modulate itch perception; 5-HT3 likely mediates spinal itch transmission
- Bile acids: activate TGR5 (Gpbar1) and MRGPRX4 receptors; MRGPRX4 identified as itch receptor for bilirubin
| Drug | Mechanism |
|---|---|
| Naloxone, naltrexone (μ-opioid antagonists) | Reduce central opioidergic tone; controlled trials show efficacy for cholestatic and renal pruritus |
| Nalfurafine (κ-opioid agonist) | Counterbalances excessive μ-opioid activity centrally |
| Ondansetron (5-HT3 antagonist) | Blocks spinal serotonergic itch transmission; useful in opioid-induced pruritus |
| Rifampicin | Upregulates hepatic opioid degradation enzymes; used in cholestatic pruritus |
| Cholestyramine | Binds bile acids in the gut → reduces circulating pruritogens |
| UDCA (ursodeoxycholic acid) | Alters bile acid pool composition |
| Thalidomide | Central depressant; inhibits TNF-α synthesis |
| SSRIs (paroxetine, sertraline, fluvoxamine) | Alter central serotonin/norepinephrine; modulate neurogenic itch signaling |
4. Psychogenic Itch
Itch arising from psychological illness (depression, anxiety, OCD, delusions of parasitosis) without underlying dermatological or systemic cause.
Mechanism: Altered descending inhibitory pathways, abnormal limbic processing of itch stimuli, comorbid psychiatric disorders amplify perception.
| Drug | Mechanism |
|---|---|
| Benzodiazepines (lorazepam, diazepam) | Relieve stress-reactive pruritus via anxiolysis |
| Antipsychotics (olanzapine, chlorpromazine, thioridazine, thiothixene) | Relieve pruritus with impulsive/delusional qualities |
| Tricyclic antidepressants (doxepin, amitriptyline) | Relieve depression + insomnia; doxepin has potent H1/H2 antihistamine action |
| SSRIs (paroxetine, fluvoxamine) | Reduce compulsive scratching and obsessive itch perception |
5. Spinal / Central Sensitization Mechanisms
Relevant in chronic pruritus of any origin - itch is amplified at the spinal cord and brain levels.
5a. Spinal Cord Neurotransmitters
- Gastrin-releasing peptide (GRP) / GRP receptor (GRPR) neurons: itch-specific interneurons in the spinal dorsal horn; GRP transmits itch but not pain
- B-type natriuretic peptide (BNP/NPPB): released by sensory neurons → activates GRPR+ neurons in spinal cord → itch signal
- Substance P / NK-1 receptor: released by primary afferents → activates dorsal horn neurons; also activates mast cells peripherally
- Glutamate / NMDA receptors: mediates spinal itch sensitization
- Inhibitory interneurons (Bhlhb5+): normally release GABA, glycine, and dynorphins to inhibit itch; loss of these neurons (disinhibition) leads to alloknesis and chronic itch
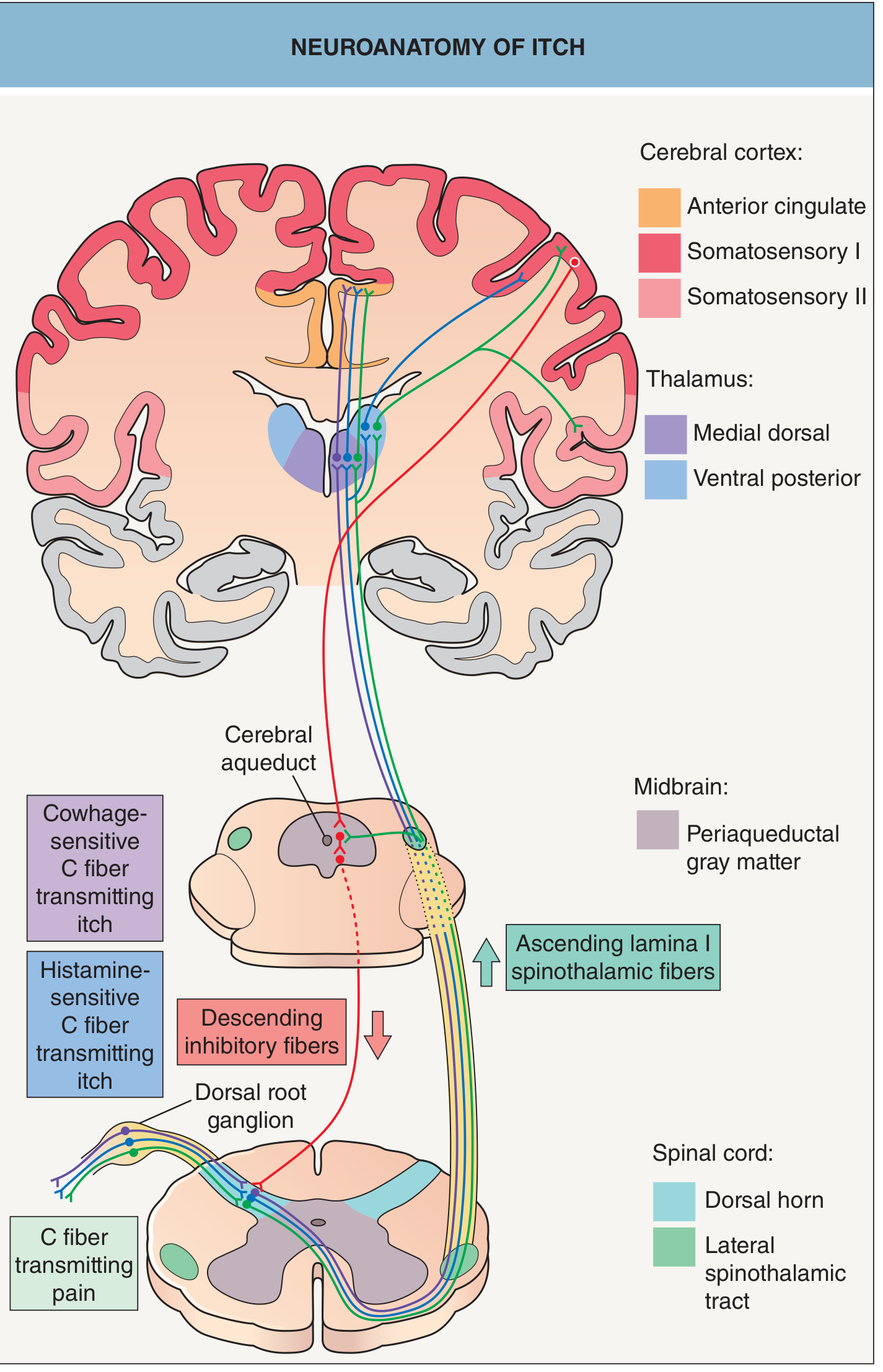
5b. Brain Processing
- Itch signals ascend via lateral spinothalamic tract to thalamus (medial dorsal + ventral posterior nuclei), then to anterior cingulate cortex, somatosensory areas I/II, insula, supramarginal gyrus
- Scratching activates the striatum and substantia nigra (reward/pleasure circuitry)
- The suprachiasmatic nucleus mediates contagious scratching behavior
| Drug | Mechanism |
|---|---|
| NK-1 antagonists (aprepitant, serlopitant, tradipitant) | Block substance P signaling on NK-1 receptors on dorsal horn neurons and dermal mast cells |
| Ketamine | NMDA receptor antagonist; blocks spinal sensitization |
| Gabapentin/pregabalin | Inhibit central itch signal amplification via Ca2+ channel modulation |
6. JAK-STAT Pathway (Cytokine Signaling)
IL-4, IL-13, IL-31, IL-33, TSLP all signal through JAK-STAT pathways to sensitize peripheral neurons and drive Th2 inflammation.
| Drug | Mechanism |
|---|---|
| Abrocitinib (JAK1-selective) | Blocks JAK1 downstream of IL-4R and IL-13R; rapid itch relief in AD |
| Upadacitinib (JAK1-selective) | Same; rapid onset itch relief (fastest among approved biologics/JAKi) |
| Baricitinib (JAK1/JAK2) | Reduces Th2 cytokine signaling |
| Ruxolitinib (topical JAK1/2) | Topical; approved for atopic dermatitis |
7. Immune-Mediated / Inflammatory Mechanisms
Skin inflammation from mast cells, eosinophils, Th2 cells releases multiple pruritogens.
| Drug | Mechanism |
|---|---|
| Topical corticosteroids | Direct antipruritic + anti-inflammatory; reduce mast cell reactivity |
| Topical calcineurin inhibitors (tacrolimus, pimecrolimus) | Block T cell activation and cytokine release |
| Topical PDE4 inhibitors (crisaborole, roflumilast) | Anti-inflammatory; increase intracellular cAMP |
| Phototherapy (NB-UVB) | Reduces mast cell reactivity, depletes epidermal nerve fibers, induces T cell apoptosis |
| Cyclosporine | Calcineurin inhibitor; suppresses T cell-mediated inflammation |
| Methotrexate, azathioprine | Suppress immune-mediated pruritus |
| Omalizumab (anti-IgE) | Reduces mast cell degranulation; effective for chronic urticaria |
Quick Reference Summary Table
| Mechanism | Key Mediators | Drug Class | Example Drugs |
|---|---|---|---|
| Histaminergic | H1/H4 receptors | H1 antihistamines | Cetirizine, hydroxyzine |
| PAR/protease | PAR-2, PAR-4, TRPV1 | TRPV1 desensitizers | Capsaicin |
| MRGPR | MRGPRX1/X2/X4 | Na+ channel blockers | Topical anesthetics |
| IL-31 / Th2 cytokines | IL-31RA, IL-4Rα | Biologics | Nemolizumab, dupilumab |
| JAK-STAT | JAK1/2 | JAK inhibitors | Abrocitinib, upadacitinib |
| Opioid peripheral | κ/μ opioid receptors | κ agonists | Difelikefalin, nalfurafine |
| Opioid central (neurogenic) | μ central excess | μ antagonists | Naltrexone, naloxone |
| Serotonin | 5-HT3 | 5-HT3 antagonists | Ondansetron |
| Neuropathic | Na+/Ca2+ channels | Gabapentinoids, Na+ blockers | Gabapentin, pregabalin, carbamazepine |
| Spinal (NK-1) | Substance P / NK-1 | NK-1 antagonists | Aprepitant, serlopitant |
| Psychogenic | Limbic/serotonin | Antidepressants, anxiolytics | SSRIs, benzodiazepines, doxepin |
| Spinal NMDA | Glutamate/NMDA | NMDA antagonists | Ketamine |
| Neurotransmitter release | ACh, SP, CGRP | Toxin | Botulinum toxin A |
| IgE/mast cell | IgE-FcεRI | Anti-IgE | Omalizumab |
Sources:
- Dermatology 2-Volume Set 5e, Ch. 5 (Cutaneous Neurophysiology)
- Goodman & Gilman's Pharmacological Basis of Therapeutics, Table 75-12
- Miller's Anesthesia 10e, Pruritus section
- Recent reviews: Chronic Pruritus Pathophysiology and Treatments (PMID 40214004, 2025) and Immune Biomarkers in Human Itch (PMID 40067363, 2025)
Give detail about urticaria, angioedema and anaphylaxis and how to differentiate, how are they related, how can they be approached and treated
Reading File
Finding Sources
Finding Sources
Searching PubMed
urticaria angioedema anaphylaxis guidelines management
Reading File
Reading File
Finding Sources
Reading File
Reading File
Reading File
Reading File
Reading File
Finding Sources
Reading File
Reading File
Finding Sources
Reading File
Reading File
Reading File
Loading Image
Reading File
Here are the key clinical takeaways organized by what makes each condition unique, how they connect, and what you must not miss:
The 5 Most Critical Points to Remember
-
Epinephrine is the ONLY first-line drug for anaphylaxis - antihistamines and steroids are adjuncts only. Delaying epinephrine to give antihistamines first is a fatal error.
-
Bradykinin angioedema does NOT respond to epinephrine/antihistamines/steroids - recognizing HAE vs allergic angioedema changes the entire treatment. The clue: no urticaria + family history + recurrent attacks + low C4.
-
Anaphylaxis can occur without skin signs (10-20%) - cardiovascular collapse or bronchospasm alone, especially after known allergen exposure, is anaphylaxis until proven otherwise.
-
ACE inhibitors can cause angioedema more than a year after starting - always review the full medication list for any patient with isolated facial/lingual/laryngeal swelling.
-
Biphasic anaphylaxis - reactions can recur 1-72 hours after apparent resolution. All anaphylaxis patients need observation for at least 4-6 hours and must be discharged with an EpiPen + action plan.
Give detail about urticaria, angioedema and anaphylaxis and how to differentiate, how are they related, how can they be approached and treated
I just answered this question in detail in our previous exchange — the full guide is right above this message. It covers:
- Definitions of all three conditions with morphology and key features
- Pathophysiology - mast cell/IgE signaling, mediators, bradykinin cascade
- Classification - acute vs chronic urticaria, histaminergic vs bradykinin angioedema, IgE-dependent vs independent anaphylaxis
- How they are related - the shared mast cell mechanism, the spectrum from localized to systemic
- Differentiation table - comparing all three side-by-side (pruritus, duration, tryptase, C4, response to epinephrine)
- Diagnostic criteria for anaphylaxis (the 3-criterion rule)
- Clinical approach - triage algorithm, history, investigations (tryptase, C4, C1-INH)
- Treatment for each: urticaria stepwise (antihistamines → omalizumab → cyclosporine), anaphylaxis algorithm (epinephrine doses, adjuncts, airway, biphasic precautions), HAE-specific drugs (icatibant, ecallantide, C1-INH replacement, lanadelumab)
- 5 critical clinical pearls not to miss
Scroll up to review it - it is all there. Let me know if you want me to expand on any specific section (e.g., HAE management in pregnancy, pediatric anaphylaxis dosing, chronic urticaria workup, or the newer biologics like remibrutinib).
This is a shared conversation. Sign in to Orris to start your own chat.