Solitary thyroid nodule
Reading File
Finding Sources
Finding Sources
Searching PubMed
"thyroid nodule" management evaluation
Reading File
Reading File
Reading File
Reading File
Reading File
Loading Image
Reading File
Reading File
Loading Image
Reading File
I now have comprehensive content from multiple authoritative surgical textbooks. Let me compile the complete, well-structured answer.
Solitary Thyroid Nodule
A solitary thyroid nodule (STN) is a discrete lesion within the thyroid gland that is radiologically distinct from the surrounding thyroid parenchyma. STNs are present in approximately 4% of individuals in the United States, yet thyroid cancer has a much lower incidence (~40 new cases per 1 million). The core clinical challenge is distinguishing the rare malignant nodule from the common benign one.
Differential Diagnosis
The vast majority (~95%) of STNs are benign. The differential is broad:
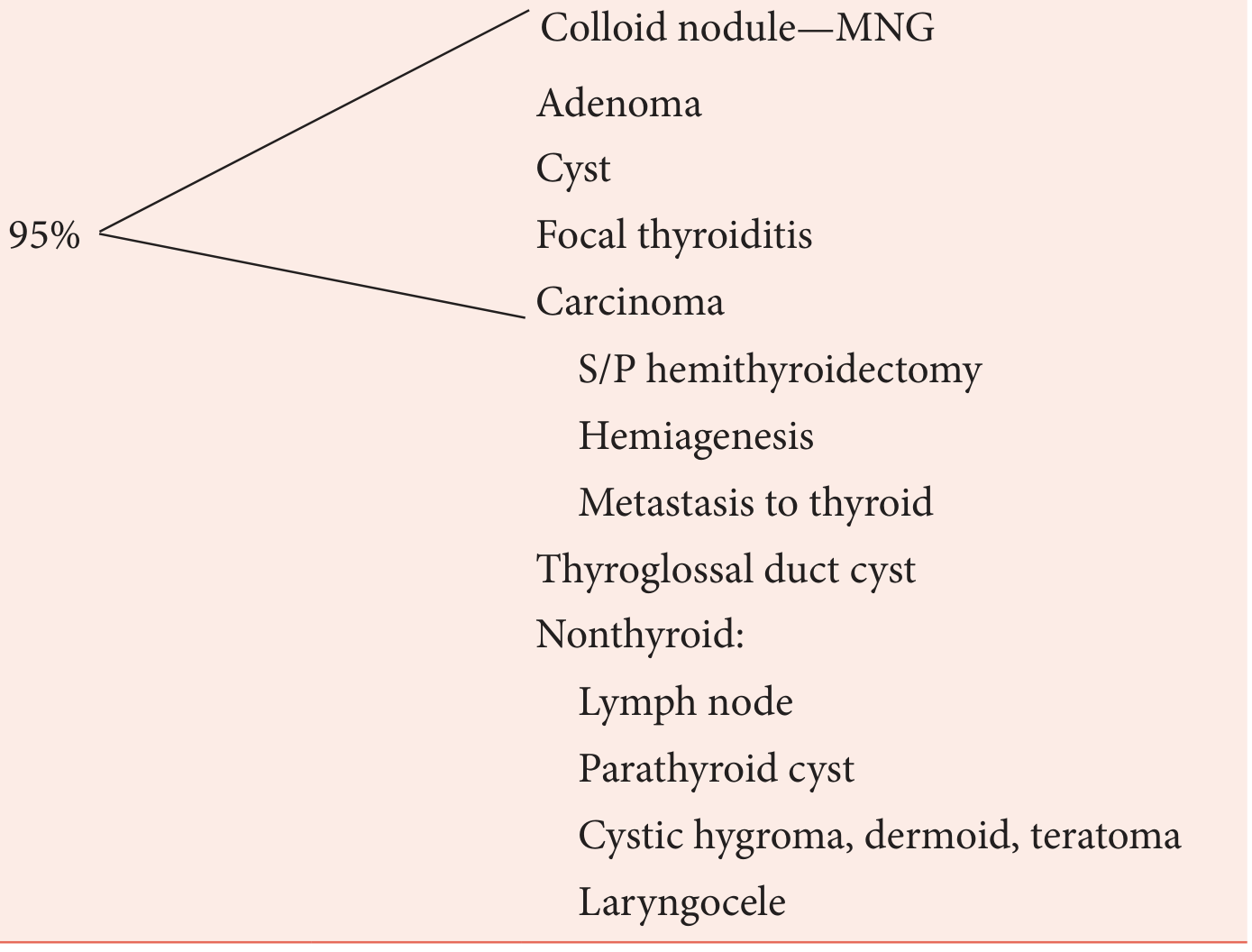
Thyroid origin (95%):
- Colloid nodule / multinodular goiter (MNG)
- Follicular adenoma
- Simple cyst
- Focal thyroiditis
- Carcinoma (papillary, follicular, medullary, anaplastic)
- Status post hemithyroidectomy
- Hemiagenesis
- Metastasis to thyroid
Non-thyroid origin:
- Thyroglossal duct cyst
- Lymph node
- Parathyroid cyst
- Cystic hygroma, dermoid, teratoma
- Laryngocele
(K.J. Lee's Essential Otolaryngology, Table 38-4)
History - Red Flags for Malignancy
| Less Concern | More Concern |
|---|---|
| Chronic stable examination | Age < 30 or > 60 years |
| Evidence of functional disorder (Hashimoto's, toxic nodule) | Male sex |
| Multinodular gland without dominant nodule | Rapid growth, pain |
| History of radiation exposure | |
| Family history of thyroid carcinoma | |
| Hard, fixed lesion | |
| Lymphadenopathy | |
| Vocal cord paralysis / hoarseness | |
| Size > 4 cm | |
| Aerodigestive tract compromise (stridor, dysphagia) |
(K.J. Lee's Essential Otolaryngology, Table 38-5)
Key history points:
- Radiation history: Low-dose therapeutic radiation (for tinea capitis, acne, tonsillar hypertrophy) confers ~40% risk of malignancy in any resulting nodule. Risk peaks 20-30 years after exposure. After Chernobyl, children showed a marked surge in papillary thyroid cancer within 4 years.
- Pain is usually hemorrhage into a benign nodule or thyroiditis; aching in the neck can also occur with medullary thyroid carcinoma (MTC).
- Hoarseness suggests possible recurrent laryngeal nerve (RLN) involvement by malignancy.
- Family history: MEN2 syndromes (medullary carcinoma + pheochromocytoma + hyperparathyroidism), Cowden disease (PTEN mutation - follicular thyroid carcinoma), Gardner syndrome (polyposis coli + papillary thyroid carcinoma).
(Schwartz's Principles of Surgery, 11th ed.; Cummings Otolaryngology)
Physical Examination
- Nodules are palpable when ≥1 cm; smaller ones are found incidentally on imaging.
- Firmness of the nodule increases the risk of malignancy 2-3 fold.
- Nodules >2 cm and solid lesions have higher incidence of carcinoma.
- Fixation to surrounding structures is strongly suspicious.
- Cervical lymphadenopathy adjacent to the nodule raises suspicion; it can be the only presenting sign of thyroid carcinoma.
- Check if the nodule moves with swallowing (thyroid origin) vs. non-thyroid.
- Assess for substernal extension: inferior aspect below the clavicle; Pemberton's maneuver (arms raised above head eliciting facial flushing + venous engorgement = thoracic inlet obstruction).
(Cummings Otolaryngology; Schwartz's Principles of Surgery)
Investigations
1. Serum TSH (First-Line)
This determines the diagnostic pathway:
- Suppressed TSH (hyperthyroid): Perform radionuclide scan - risk of malignancy is only ~1% in hot nodules.
- Elevated TSH (hypothyroid): Treat appropriately, then perform FNAC.
- Normal TSH (euthyroid): Most patients - proceed directly to ultrasound + FNAC.
2. Ultrasound (US) - Most Important Imaging
- Differentiates solid vs. cystic nodules.
- Identifies sonographic features raising malignancy risk: microcalcifications, hypoechoic solid nodule, irregular margins, taller-than-wide shape, absent halo, abnormal regional nodes.
- Guides FNAC for difficult-to-palpate nodules.
- Preferred for surveillance of benign nodules.
- Elastography: malignant nodules are stiffer (less deformable) than benign; newer technique, still being validated.
- Contrast-enhanced ultrasound (CEUS): A 2026 meta-analysis (Huo et al., PMID 42262145) shows emerging diagnostic utility for nodule characterization.
3. Fine Needle Aspiration Biopsy (FNAB) - Gold Standard
The cornerstone of evaluation. US guidance is recommended for:
- Difficult-to-palpate nodules
- Cystic/solid-cystic nodules recurring after prior aspiration
- Multinodular goiters
Adequate specimen = ≥6 follicular groups, each with ≥10-15 cells from ≥2 aspirates.
4. Radionuclide Scanning (¹²³I or ⁹⁹ᵐTc)
- NOT routine - use only if TSH is suppressed (to confirm hot/warm nodule) or after indeterminate FNAC.
- Cold nodules: 95% of all nodules; malignancy rate 10-15%.
- Hot nodules: malignancy rate ~4% (benign autonomous nodule usually).
- ⁹⁹ᵐTc: tests iodine transport only, faster (1 day), less radiation; cannot penetrate sternum.
- ¹²³I: tests transport AND organification; 2 days; preferred for substernal extension.
5. CT / MRI
- Not routine for thyroid nodule evaluation.
- Indicated for: substernal lesions, large/fixed tumors, suspected visceral compartment invasion, mediastinal adenopathy.
- Caution: iodinated CT contrast delays postoperative RAI therapy by 2-3 months.
- MRI superior to CT for distinguishing recurrent tumor vs. postoperative fibrosis.
6. Laboratory Tests
- Serum TSH - always
- Serum calcitonin - if MTC or MEN2 suspected (family history, FNAB suspicious for MTC)
- Serum thyroglobulin (Tg) - cannot differentiate benign from malignant preoperatively; used for post-thyroidectomy surveillance
- RET oncogene mutation testing - all patients with confirmed MTC; 24-hr urine VMA/metanephrines to rule out pheochromocytoma
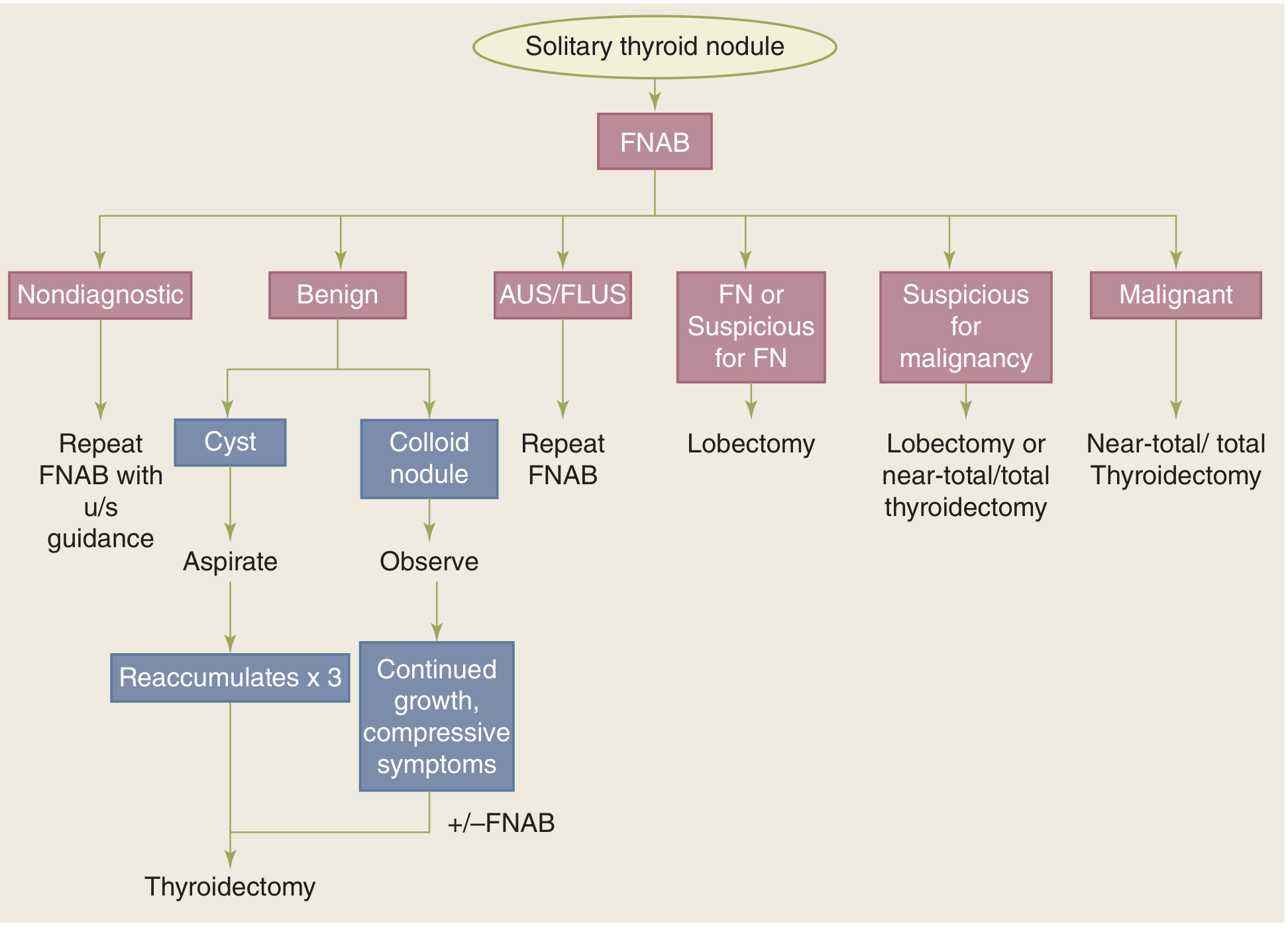
Bethesda Classification of FNAB Results + Management
| Bethesda Category | Frequency | Malignancy Risk | Management |
|---|---|---|---|
| I - Nondiagnostic/Unsatisfactory | 2-20% | 1-4% | Repeat FNAB with US guidance |
| II - Benign | 60-70% | ~3% (false-negative) | Observe; surgery if growth/compressive symptoms |
| III - AUS/FLUS | 3-6% | 5-15% | Repeat FNAB; consider molecular testing |
| IV - Follicular Neoplasm (FN) | - | 15-35% | Diagnostic lobectomy |
| V - Suspicious for Malignancy | - | 60-75% | Lobectomy or near-total/total thyroidectomy |
| VI - Malignant | - | 97-99% | Near-total/total thyroidectomy |
(Schwartz's Principles of Surgery, 11th ed.; Cummings Otolaryngology)
Key details:
- Benign (II): Most common result. Includes colloid nodule, follicular adenoma, Hashimoto's, granulomatous thyroiditis. Cysts are aspirated; if they reaccumulate 3 times, thyroidectomy is recommended. Colloid nodules are observed; thyroidectomy if continued growth or compressive symptoms.
- FN/Suspicious for FN (IV): Up to 35% of Bethesda IV lesions are actually hyperplastic follicular proliferations, not true neoplasms. Lobectomy is preferred as it is both diagnostic and potentially therapeutic.
- Malignant (VI): Near-total or total thyroidectomy.
Molecular Marker Testing (for Indeterminate FNAB)
For Bethesda III/IV results, molecular testing helps avoid unnecessary surgery:
| Test | Role | Key Performance |
|---|---|---|
| Afirma Gene Expression Classifier | Rule-OUT malignancy | Sensitivity 92%, NPV 93% |
| ThyroSeq | Rule-OUT malignancy | NPV ~95% |
| ThyGenX/ThyraMIR | Rule-IN malignancy | Highest PPV ~66% |
(Cummings Otolaryngology)
Management Algorithm Summary
- History + Physical Exam - identify high-risk features
- Serum TSH
- Suppressed → Radionuclide scan → hot nodule = treat medically; cold nodule = FNAB
- Normal/elevated → Ultrasound + FNAB
- FNAB result guides surgical vs. conservative management (Bethesda criteria)
- Surgery for: malignant/suspicious cytology, follicular neoplasm, cyst reaccumulating ×3, symptomatic growth, history of radiation exposure, high-risk clinical features
Special Situations
- Radiation-exposed patients: Even a nodule showing benign FNAB cytology may harbor cancer in a separate nodule in 40% of cases - near-total thyroidectomy may be warranted.
- Children (<20 years): 20-50% malignancy rate with STN - aggressive workup mandatory.
- Elderly males: Higher incidence of nodular disease; malignancy if found has worse prognosis.
- MEN2 / Medullary thyroid carcinoma: Confirm RET mutation, rule out pheochromocytoma before surgery.
Recent evidence update: A 2025 systematic review (Lim et al., PMID 40658618) confirms efficacy and safety of thermal ablation (radiofrequency, microwave, laser) as a non-surgical option for indeterminate benign thyroid nodules, offering volume reduction while preserving thyroid function.
Sources: Schwartz's Principles of Surgery 11th ed. | K.J. Lee's Essential Otolaryngology | Cummings Otolaryngology Head and Neck Surgery
Answer to my last question?
Your last question was "Solitary thyroid nodule" — and I already answered it in full detail just above.
The response covered:
- Definition & epidemiology - present in ~4% of the US population
- Differential diagnosis - 95% benign (colloid nodule, adenoma, cyst, focal thyroiditis, carcinoma)
- History & red flags for malignancy (age <30/>60, male sex, radiation exposure, rapid growth, hoarseness, lymphadenopathy, fixation)
- Physical examination findings
- Investigations - TSH, ultrasound, FNAB (gold standard), radionuclide scan, CT/MRI, lab tests
- Bethesda classification (I-VI) with malignancy risk and management per category
- Molecular marker testing (Afirma, ThyroSeq, ThyGenX) for indeterminate FNAC
- Management algorithm flowchart
- Special situations (radiation exposure, children, MEN2)
Scroll up to read the full answer. Let me know if you'd like me to expand on any specific aspect.
This is a shared conversation. Sign in to Orris to start your own chat.