A 3-year-old boy is brought to the emergency department with a 3-day history of fever, cough, and difficulty breathing. His mother reports that the cough started as mild but has become more frequent and productive. The child has also been less active and is refusing to eat. Diagnosis and name of organism?
"community-acquired pneumonia" AND "children" AND "etiology"
Diagnosis: Community-Acquired Pneumonia (CAP)
Most Likely Causative Organisms (Age 2-5 Years)
"In children between 2 and 5 years of age, most community-acquired pneumonia is caused by respiratory viruses, notably respiratory syncytial virus, human rhinovirus, and human metapneumovirus. Other notable pathogens in this age group include Streptococcus pneumoniae, H. influenzae type b, and nontypeable H. influenzae. Mycoplasma pneumoniae and Chlamydophila pneumoniae are thought to be less common in children <5 years old."
- Tintinalli's Emergency Medicine, p. 853
| Priority | Organism | Type | Notes |
|---|---|---|---|
| #1 (if viral) | Respiratory syncytial virus (RSV), Human rhinovirus, Human metapneumovirus | Virus | Most common overall; >70% of hospitalized pediatric pneumonias |
| #1 (if bacterial) | Streptococcus pneumoniae | Gram-positive coccus | Most common bacterial CAP in this age group |
| #2 | Haemophilus influenzae (nontypeable or type b) | Gram-negative rod | More common in unvaccinated children |
| #3 | Staphylococcus aureus | Gram-positive coccus | Less common; associated with rapid progression, abscess formation |
| Less common | Mycoplasma pneumoniae | Atypical | More common >5 years; causes dry/hacking cough |
Clinical Features Explained
| Feature in This Child | Significance |
|---|---|
| Age 3 years | Peak risk for S. pneumoniae and RSV CAP |
| Fever (3 days) | Both viral and bacterial; higher/sustained fevers favor bacterial |
| Productive cough | More suggestive of bacterial origin (lobar/alveolar pneumonia) |
| Progressive worsening | Classic for bacterial "typical" CAP |
| Reduced activity + poor intake | Systemic illness/toxicity - raises concern for bacterial etiology |
| Respiratory distress | Lower respiratory tract involvement confirmed |
Pathophysiology
Workup
- Chest X-ray - lobar/segmental consolidation favors bacterial; bilateral interstitial infiltrates favor viral/atypical
- CBC - leukocytosis with neutrophilia suggests bacterial etiology
- Blood culture - in hospitalized children (yield ~3-7% but useful when positive)
- Nasopharyngeal swab for rapid viral panel (RSV, influenza, rhinovirus, metapneumovirus)
- Pulse oximetry and respiratory rate - key severity markers
- CRP / Procalcitonin - procalcitonin >0.25 ng/mL supports bacterial etiology
Treatment
Physical examination findings in consolidation
Physical Examination Findings in Pulmonary Consolidation
Summary Table (from Murray & Nadel's Respiratory Medicine)
| Examination Step | Normal Finding | Consolidation Finding |
|---|---|---|
| Inspection | Symmetric chest rise | Possible lag or splinting on affected side |
| Palpation | Normal tactile fremitus | Increased tactile fremitus |
| Percussion | Resonant | Dullness |
| Auscultation | Vesicular breath sounds | Bronchial breath sounds; bronchophony, pectoriloquy, crackles |
Murray & Nadel's Textbook of Respiratory Medicine, Table 18.4
Finding-by-Finding Breakdown
1. Inspection
- Chest wall lag / splinting on the affected side - the patient subconsciously limits expansion of the painful/consolidated side
- Tachypnea - increased respiratory rate is one of the most sensitive early signs
- Use of accessory muscles in severe disease
2. Palpation - Increased Tactile Fremitus
- Ask the patient to say "99" or "one, one, one" and feel chest wall vibrations with the ulnar edge of the hand
- Consolidated (solid) lung transmits low-frequency sound vibrations better than air-filled lung, so vibration is felt more strongly over the affected area
- Contrast: over a pleural effusion, fremitus is decreased (fluid insulates the chest wall from vibration)
"Tactile fremitus increases over an area of consolidation related to pneumonia." - Frameworks for Internal Medicine
3. Percussion - Dullness
- Consolidated lung is solid, not air-filled, so percussion produces a dull (not resonant) note over the affected area
- A very large effusion produces a "stony dull" or flat note
- Dullness to percussion is consistent with both consolidation and pleural effusion - differentiate by fremitus (increased in consolidation, decreased in effusion)
"Dullness to percussion is consistent with consolidation or a pleural effusion." - Goldman-Cecil Medicine
4. Auscultation - Multiple Signs
- Normally, vesicular (soft, rustling) breath sounds are heard over the lung periphery
- In consolidation, large-airway sounds (normally only heard over the trachea/mainstem bronchi) are transmitted through the solid lung to the chest wall - heard as loud, hollow, bronchial sounds with an audible expiratory phase equal to or longer than inspiration
- Late inspiratory crackles (fine crackles/crepitations) over the affected area
- Caused by the explosive reopening of small airways and alveoli that have collapsed due to fluid/exudate
- Heard classically at the end of inspiration
- Ask patient to say "99" - words are transmitted with abnormally increased clarity and volume over consolidated lung
- Normal aerated lung filters and muffles spoken words; solid lung transmits them sharply
- Ask patient to say "eee" - over consolidation, it is heard through the stethoscope as "ayyy"
- The word "egophony" means "goat sound" (Greek: ego = goat) - the bleating, nasal quality is characteristic
- Mechanism: consolidated lung selectively filters lower frequencies, causing the "ee" vowel to shift upward in pitch to sound like "ay"
- Most common when consolidation and pleural fluid coexist; also heard in uncomplicated lobar pneumonia and pulmonary infarction
"When bronchophony is extreme, spoken words assume a nasal or bleating quality (egophony) and the sound 'ee' is heard through the stethoscope as 'ay'." - Fishman's Pulmonary Diseases and Disorders
- Ask patient to whisper a phrase (e.g., "66 whiskeys, please")
- Normal aerated lung acts as a filter - whispered words are garbled and indecipherable
- Over consolidation, whispered words are heard clearly and distinctly
- Pectoriloquy = "chest speaking" (Latin: pectus = chest, loqui = to speak)
- Has the same significance as bronchophony; indicates non-aerated lung (consolidation, tumor, or compressed lung)
"Normal, aerated lung acts as a filter, making these whispered words garbled and undecipherable. If the words are clearly discernible, then pectoriloquy is present and indicative of underlying nonaerated lung." - Frameworks for Internal Medicine
Why These Signs Occur - The Unifying Mechanism
Important Caveat
"None of these findings on physical examination is sufficiently sensitive or specific to avoid the need for imaging for radiographic validation."
Radiology Correlation
- Goldman-Cecil Medicine, Figure 35-1
How do you differentiate consolidation from pleural effusion on exam?
Differentiating Consolidation from Pleural Effusion on Physical Examination
Head-to-Head Comparison Table
| Examination Step | Consolidation (Pneumonia) | Pleural Effusion | Why They Differ |
|---|---|---|---|
| Inspection | Possible lag/splinting | Lag + increased hemithorax size; trachea & mediastinum shift away from effusion (if large) | Mass effect of fluid pushes structures to opposite side |
| Tactile fremitus | Increased | Decreased or absent | Solid lung conducts vibration better; fluid between lung and wall blocks it |
| Percussion | Dull | Dull to stony flat | Both are dull, but effusion can be flatter/heavier-sounding |
| Breath sounds | Bronchial (loud, tubular) | Absent or markedly reduced | Consolidated lung transmits large-airway sounds; fluid insulates/silences |
| Crackles | Present (late inspiratory) | Absent | Fluid-filled alveoli popping open in consolidation; effusion has no alveolar interface |
| Egophony ("E to A") | Present over consolidation | Absent (except 1-2 cm band at the top edge of effusion) | Compressed lung at fluid's upper border briefly acts like consolidation |
| Whispered pectoriloquy | Present | Absent | Same mechanism as egophony |
| Bronchophony | Present | Absent | Fluid blocks sound transmission |
| Pleural rub | Absent | May be present (if inflamed pleura, before fluid accumulates) | Friction between inflamed pleural surfaces |
The Pivotal Finding: Tactile Fremitus
"Tactile fremitus is increased over an area of consolidation, whereas it is decreased (often absent) over an effusion. The area of compressed lung just above an effusion is sometimes associated with a thin band of increased tactile fremitus and other signs of consolidation."
- Frameworks for Internal Medicine
"Vocal fremitus and tactile fremitus are increased in lung consolidation but decreased in pleural effusion."
- Textbook of Family Medicine 9e
"Vocal fremitus is increased over regions of lungs where there is increased transmission of sound, for example, consolidation from pneumonia. Conversely, fremitus is decreased in conditions in which sound transmission is impaired, for example, pleural effusion."
- Murray & Nadel's Textbook of Respiratory Medicine
- In consolidation, the lung is solid and directly contiguous with the chest wall - it conducts low-frequency vocal vibrations better than normal
- In pleural effusion, fluid sits between the visceral pleura and the chest wall - it acts as an acoustic insulator, blocking vibrational transmission to the examining hand
The Egophony Trap
"Localized egophony ('e-to-a' changes) indicates consolidation of that segment or lobe of the lung; it is NOT present in pleural effusion except in a small band just above the upper edge of the effusion."
- Textbook of Family Medicine 9e
Mediastinal Shift - An Extra Clue for Large Effusions
| Direction of Shift | Diagnosis |
|---|---|
| Trachea shifts away from dull side | Large pleural effusion (mass effect pushing structures away) |
| Trachea shifts toward dull side | Atelectasis (volume loss pulling structures toward it) |
| No tracheal shift | Consolidation (lung volume is maintained, just airless) |
"The distinction between pleural effusion and atelectasis can be made on physical examination by determining whether the heart and mediastinal contents shift toward or away from the abnormal side."
- Murray & Nadel's Textbook of Respiratory Medicine
Complete Differential: Three Dull Conditions Side by Side
| Finding | Consolidation | Pleural Effusion | Atelectasis |
|---|---|---|---|
| Fremitus | Increased | Decreased/absent | Decreased |
| Percussion | Dull | Dull/stony flat | Dull/flat |
| Breath sounds | Bronchial + crackles | Absent | Absent |
| Egophony | Present | Absent (thin band at top only) | Absent |
| Tracheal shift | None | Away from lesion | Toward lesion |
| Expansion | Slight lag | Lag + increased size | Lag + decreased size |
Practical Memory Aid
- Consolidation = solid lung = everything conducted/amplified (fremitus up, bronchial breathing, egophony, pectoriloquy)
- Pleural effusion = fluid barrier between lung and chest wall = everything blocked/silenced (fremitus down, no breath sounds, no voice signs)
A 6-month-old infant is brought to the clinic with a 3-day history of cough, runny nose, and low-grade fever. Over the last 24 hours, the baby has developed difficulty breathing and poor feeding. The mother also noticed fast breathing and wheezing. Diagnosis and organism causing this?
"bronchiolitis" AND "RSV" AND "management"
Diagnosis: Bronchiolitis
Causative Organism: Respiratory Syncytial Virus (RSV)
Why This Case = Bronchiolitis
| Feature | Significance |
|---|---|
| Age 6 months | Peak age for bronchiolitis (< 2 years, especially < 6 months) |
| 3-day URTI prodrome (cough, rhinorrhoea, low-grade fever) | Classic RSV starting as an upper respiratory infection |
| Progression to wheeze + tachypnea at day 3-4 | Virus tracking down to the small airways (bronchioles) |
| Poor feeding | Increased work of breathing makes coordinated suck-swallow-breathe impossible |
| Wheeze (not stridor) | Obstruction at the level of small airways, not the upper airway |
The Organism: Respiratory Syncytial Virus (RSV)
"RSV is the most common infectious agent [in bronchiolitis], although influenza virus, adenovirus, parainfluenza virus, human metapneumovirus, coronavirus, and human bocavirus also cause bronchiolitis."
- Swanson's Family Medicine Review
Other causative organisms (in decreasing order of frequency):
| Organism | Notes |
|---|---|
| RSV | #1 cause; peaks in winter/early spring |
| Human Metapneumovirus (hMPV) | #2 cause; similar clinical picture to RSV; tends to affect slightly older infants |
| Parainfluenza virus (types 1, 2, 3) | Also causes croup |
| Influenza virus | Seasonal |
| Adenovirus | Can cause more severe disease |
| Human bocavirus | Emerging pathogen |
| Rhinovirus | Common co-pathogen |
Pathophysiology
"Pathophysiologic features of bronchiolitis include inflammation, edema, and necrosis of the epithelial linings of the small airways. Increased production of mucus and bronchospasm are seen in conjunction with wheeze, cough, accessory muscle use, tachypnea, and rhinorrhoea."
- Swanson's Family Medicine Review
- RSV infects and destroys bronchiolar epithelium
- Inflammatory edema + increased mucus secretion narrow the small airways
- Partial airway obstruction creates air trapping (wheeze on expiration, hyperinflation on CXR)
- Complete obstruction of some bronchioles causes atelectasis (patchy collapse)
- Ventilation-perfusion mismatch leads to hypoxemia and, in severe cases, hypercapnia
Clinical Features in Detail
Symptoms
- Prodrome (days 1-3): rhinorrhoea, low-grade fever, mild cough - indistinguishable from a common cold
- Lower tract phase (days 3-5): worsening cough, rapid breathing, wheeze, feeding difficulty
- Peak severity: around day 3-5; total illness duration typically 10-14 days
Signs on Examination
- Tachypnea (RR > 50-60/min in infants) - most sensitive sign of severity
- Subcostal/intercostal retractions - increased work of breathing
- Nasal flaring
- Hyperinflation - barrel-shaped chest; liver pushed down (due to air trapping)
- Widespread fine end-expiratory crackles and wheeze (expiratory > inspiratory)
- Hypoxia (SpO2 < 92% in severe disease)
- Poor feeding / dehydration
- Fever is variable - often low-grade or absent
Chest X-Ray Findings
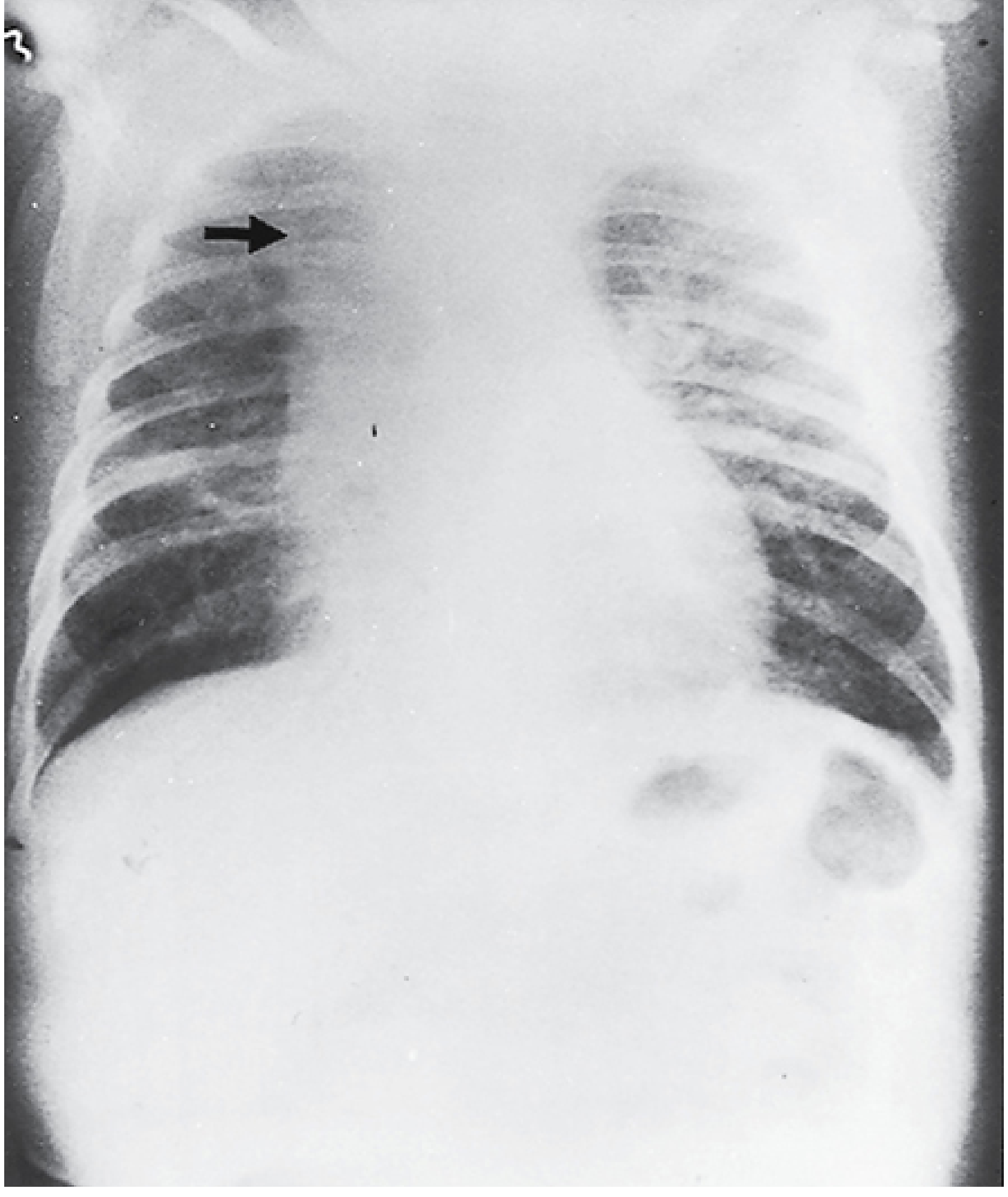
- Bilateral hyperinflation (flat diaphragms, increased AP diameter, >9 posterior ribs visible)
- Peribronchial cuffing (thickened bronchial walls)
- Patchy atelectasis (often right upper lobe - due to small right upper lobe bronchus easily blocked)
- Bilateral interstitial infiltrates
- Note: CXR is NOT routinely recommended - clinical diagnosis is sufficient in typical cases
Diagnosis
- Clinical diagnosis in most cases - no investigations routinely needed
- Rapid antigen test / RT-PCR nasopharyngeal swab can confirm RSV (useful for cohorting in hospital, not to change management)
- Multiplex respiratory panel (e.g., BioFire) detects RSV, hMPV, parainfluenza, and 14-19 other pathogens simultaneously
Management (Evidence-Based)
| Intervention | Recommendation |
|---|---|
| Oxygen (if SpO2 < 90-92%) | YES - mainstay |
| Nasal suctioning | YES - provides temporary benefit |
| Adequate hydration (IV/NG if feeding compromised) | YES |
| High-flow nasal cannula (HFNC) | Increasingly used in moderate-severe disease |
| Bronchodilators (salbutamol, epinephrine) | NOT routinely recommended (Cochrane review: no consistent benefit); trial appropriate in select moderate-severe cases |
| Corticosteroids | NOT recommended (no benefit in RCTs) |
| Antibiotics | NOT recommended (bacteremia risk only 0.2%; use only if confirmed bacterial co-infection) |
| Chest physiotherapy | NOT recommended |
| Ribavirin (aerosol) | Controversial; may be considered in very high-risk immunocompromised infants |
High-Risk Groups (Severe/Fatal Disease)
"The fatality rate among hospitalized infected infants is estimated to be 0.5%-1%; however, this rises higher in children receiving cancer chemotherapy, infants with congenital heart disease, and those with severe immunodeficiency."
- Sherris & Ryan's Medical Microbiology
- Premature infants (especially < 32 weeks gestation)
- Congenital heart disease (haemodynamically significant)
- Chronic lung disease (e.g., bronchopulmonary dysplasia)
- Immunodeficiency
- Age < 3 months
Prevention
Recent 2025 ALAT Consensus [PMID: 41714249] and 2025 Australasian Bronchiolitis Guideline [PMID: 40685806] confirm supportive care remains the cornerstone of management.
A 4-year-old girl is brought to the emergency department with a 2-day history of vomiting and diarrhea. Her mother reports that she has become very weak and has not passed urine since the morning. The child is also drowsy and refusing oral intake. Diagnosis and treatment?
Diagnosis: Severe Dehydration secondary to Acute Gastroenteritis
Clinical Reasoning
| Feature | Interpretation |
|---|---|
| 2-day vomiting + diarrhea | Acute gastroenteritis - fluid and electrolyte losses |
| No urine since morning | Oliguria/anuria = severe volume depletion, kidneys maximally conserving water |
| Drowsy, weak | CNS effects of severe dehydration/electrolyte imbalance - a red flag |
| Refusing oral intake | Cannot self-correct dehydration - IV access mandatory |
| Age 4 years | High surface-area-to-volume ratio makes children rapidly dehydrated |
- Abnormal mental status (drowsy)
- Oliguria/anuria
- Weakness
- Refusal of oral intake
Causative Organisms
"Rotavirus is a common etiology of gastroenteritis leading to hospitalization of children from dehydration and lethargy."
- Yamada's Textbook of Gastroenterology
| Organism | Type | Notes |
|---|---|---|
| Rotavirus | Virus | #1 cause of severe gastroenteritis with hospitalization in children <5 years; watery diarrhoea, vomiting, low-grade fever; peaks in winter |
| Norovirus | Virus | Most common overall gastroenteritis cause in all ages; highly contagious; 68-90% of outbreak gastroenteritis |
| Adenovirus (types 40/41) | Virus | Enteric adenovirus; prolonged diarrhoea |
| Salmonella spp. | Bacteria | Fever + bloody diarrhoea; food-borne |
| Campylobacter jejuni | Bacteria | Bloody diarrhoea, cramping |
| E. coli (ETEC, EPEC) | Bacteria | Traveller's diarrhoea, infants |
| Staphylococcus aureus | Bacteria | Rapid onset vomiting (toxin-mediated, within 1-6 hrs) |
| Bacillus cereus | Bacteria | Fried rice; emetic or diarrhoeal toxin |
Dehydration Assessment (Degree in This Child)
| Degree | Signs | Fluid Lost (Older Child) | Treatment |
|---|---|---|---|
| Mild | Thirst, slightly dry mucosae | 3-5% body weight | ORS 50-100 mL/kg over 2-4 hrs |
| Moderate | Tachycardia, CRT >2 sec, sunken eyes, absent tears, weak pulse | 6-9% body weight | ORS; IV if not tolerated |
| Severe | Abnormal mental status, lethargy, abnormal skin turgor, sunken fontanelle, hypotension | >9% body weight | 20-60 mL/kg NS IV bolus + labs |
Treatment
Step 1 - Immediate IV Resuscitation (Emergency)
"Standard therapy involves 20-mL/kg boluses of NS or lactated Ringer's solution infused over a 60-minute period each, until normalization of pulse, perfusion, and mental status occurs."
- Roberts & Hedges' Clinical Procedures in Emergency Medicine
- IV access - establish immediately (two large-bore cannulas or intraosseous if IV fails)
- Fluid bolus: 20 mL/kg of Normal Saline (0.9% NaCl) or Lactated Ringer's over 15-60 minutes
- Repeat boluses of 20 mL/kg as needed, reassessing after each bolus (pulse, CRT, mental status, urine output)
- A 4-year-old is typically ~16-18 kg, so first bolus = ~320-360 mL
Step 2 - Urgent Investigations
| Test | Rationale |
|---|---|
| Serum electrolytes (Na, K, Cl, HCO3) | Hyponatraemia / hypernatraemia; hypokalaemia from diarrhoea |
| Blood glucose (URGENT) | >9% of severely dehydrated children have hypoglycaemia - give dextrose if low |
| Urea and creatinine | Assess for prerenal AKI (elevated BUN:Cr ratio >20:1) |
| Venous blood gas / lactate | Assess metabolic acidosis severity |
| FBC | Haemoconcentration; rule out sepsis |
| Urine output monitoring | Key indicator of fluid resuscitation success |
| Stool culture | If bloody diarrhoea or features of bacterial infection |
Step 3 - Maintenance Fluids (After Stabilisation)
- 100 mL/kg for first 10 kg = 1000 mL
- 50 mL/kg for next 10 kg = 500 mL
- 20 mL/kg for remaining weight
Step 4 - Antiemetic
- Ondansetron 0.15 mg/kg IV - reduces vomiting, reduces need for IV hydration, NNT = 5
- For a ~17 kg child: 4 mg IV/oral
- Caution: prolongs QTc by 10-17 ms (generally safe in healthy children)
Step 5 - Transition to Oral Rehydration
- Transition to Oral Rehydration Solution (ORS) - WHO formula: 75 mEq/L sodium, 20 g/L glucose
- Start small volumes: 5-10 mL every 5 minutes, increasing slowly
- ORS is equivalent to IV therapy in mild-moderate dehydration (Cochrane evidence)
Step 6 - Specific Interventions
| Drug | Indication |
|---|---|
| Dextrose 10% 2 mL/kg IV | If blood glucose < 3.0 mmol/L (hypoglycaemia) |
| Potassium supplementation | If hypokalaemia confirmed on labs (do NOT give until urine output restored) |
| Antibiotics | NOT routinely indicated; only if confirmed bacterial cause (e.g., Salmonella with systemic features, Campylobacter, Shigella, C. difficile) |
| Zinc (WHO protocol) | 20 mg/day for 10-14 days in developing world settings; reduces diarrhoea duration |
| Loperamide / antidiarrhoeals | CONTRAINDICATED in children <5 years |
Admission Criteria
- Severe dehydration with altered mental status
- Oliguria/anuria
- Unable to tolerate oral fluids
- IV rehydration needed
Prevention (Rotavirus)
- Rotavirus oral vaccine (Rotarix or RotaTeq) - given at 6-10-14 weeks of age; reduces severe gastroenteritis hospitalisations by ~85%
- Hand hygiene, safe water, food hygiene
Immunological causes of glomerulonephritis and their mechanisms
Immunological Causes of Glomerulonephritis and Their Mechanisms
- Immune complex deposition (circulating or in situ)
- Anti-GBM antibody disease
- ANCA-mediated (pauci-immune) vasculitis
- Complement dysregulation (alternative pathway)
- Cell-mediated immunity (T-cell driven) - supporting role
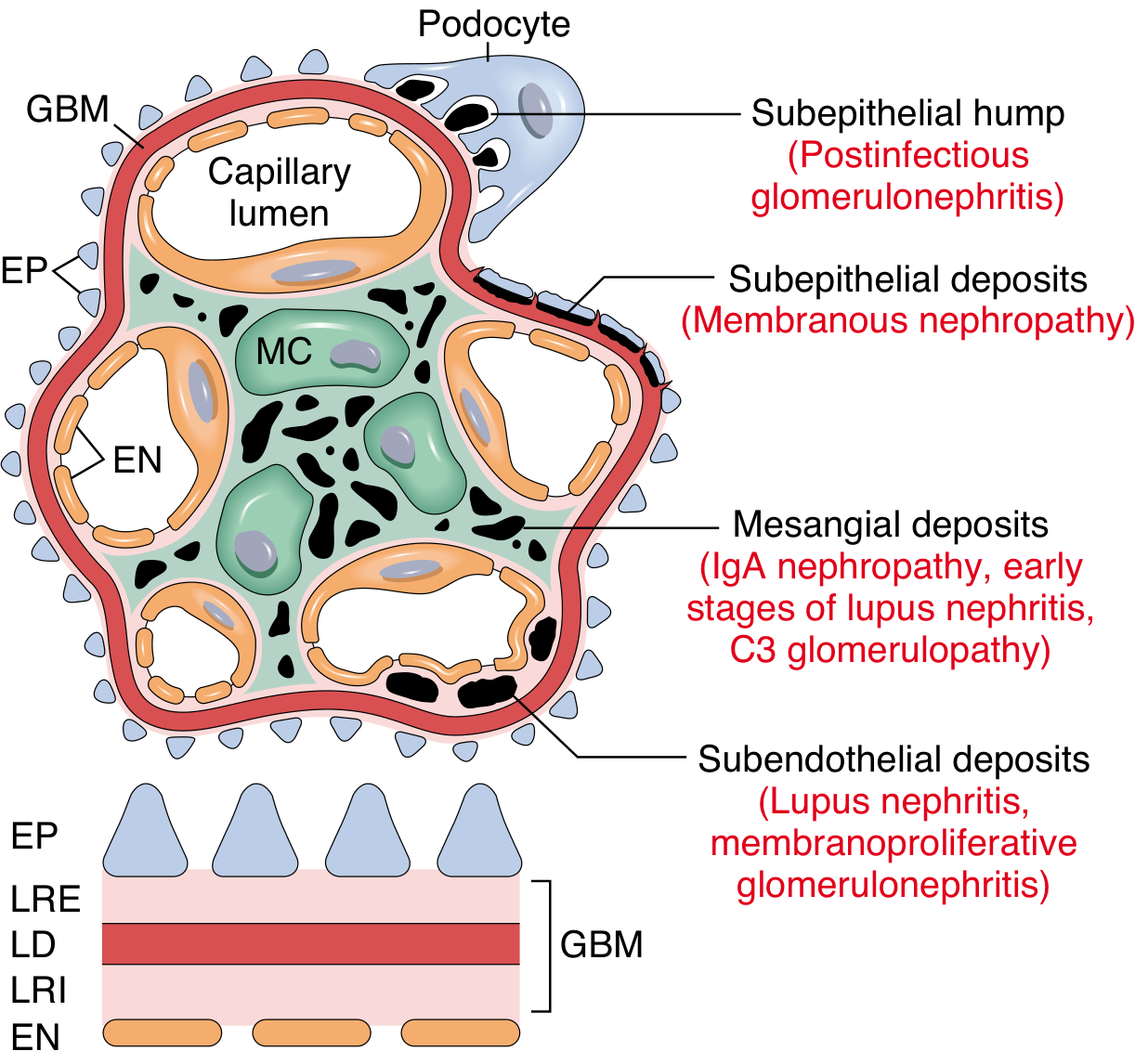
The Immunological Deposit Location Diagram
Mechanism 1: Immune Complex-Mediated GN
How immune complexes form in the glomerulus:
- Antigen-antibody complexes form in the bloodstream and become trapped in the glomerular filtration barrier
- Favored by: large amounts of antigen, low-avidity antibodies, impaired reticuloendothelial clearance
- Factors governing deposition site: charge, size of complexes, glomerular hemodynamics, mesangial function
- Circulating antigen "plants" in the glomerulus first; antibody then binds to it in situ
- Classic example: Heymann nephritis (experimental model of membranous nephropathy) - megalin/PLA2R antigen in the podocyte foot process is the target
Two root causes of immune complex accumulation:
"Two major mechanisms account for the presence of immune complexes in glomerular diseases. There may be ineffectual clearance of an antigen from an impaired immune response, as in chronic viral infections caused by hepatitis B or hepatitis C virus... More often, glomerular disease results from autoimmunity."
- Comprehensive Clinical Nephrology, 7th Edition
| Root Cause | Mechanism | Example Diseases |
|---|---|---|
| Persistent antigenemia | Chronic infection prevents antigen clearance; persistent humoral response creates circulating complexes | HBV nephropathy, HCV cryoglobulinaemia, post-streptococcal GN, malaria |
| Autoimmunity (loss of tolerance) | Self-reactive T and B cells escape deletion; molecular mimicry or danger signals trigger immune response to self-antigen | SLE (lupus nephritis), IgA nephropathy |
Location determines the inflammatory response:
"The presence of glomerular inflammation is largely determined by the site of immune deposits. Immune deposits with direct access to the circulation (subendothelial and intrabasement membrane locations) are usually associated with leukocyte accumulation. Mesangial deposits elicit an intermediate response, whereas immune deposits in the subepithelial space generally are not associated with inflammatory cells."
- Comprehensive Clinical Nephrology, 7th Edition
| Deposit Location | Access to Circulation | Inflammatory Response | Diseases | IF Pattern |
|---|---|---|---|---|
| Subendothelial | Direct | Intense - neutrophils, monocytes, complement activation | Lupus nephritis (class III/IV), MPGN type I | Granular, "wire-loop" |
| Mesangial | Intermediate | Moderate - mesangial proliferation | IgA nephropathy, early lupus (class II), C3 glomerulopathy | Mesangial granular |
| Subepithelial | Shielded by GBM | Minimal cellular inflammation; complement mediates podocyte damage | Membranous nephropathy, post-infectious GN ("humps") | Granular peripheral ("lumpy-bumpy") |
| Intrabasement membrane | Direct | Severe | Goodpasture disease (linear, not granular) | Linear (ribbon-like) |
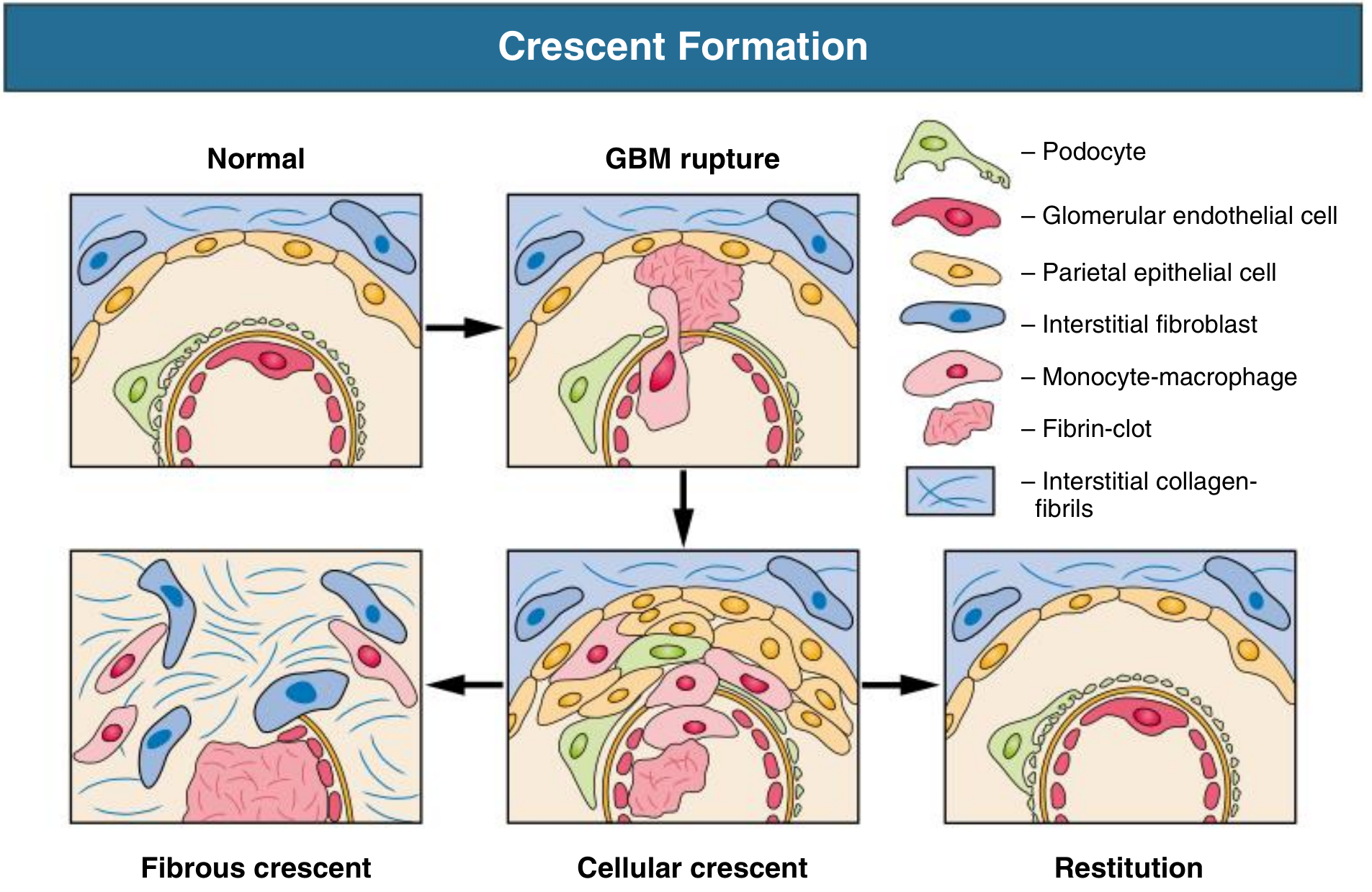
"Subendothelial immune complexes provoke leukocyte infiltration and glomerular crescent formation... In contrast, subepithelial immune complexes are shielded from the circulation by the GBM and do not induce inflammatory responses."
- Robbins & Cotran Pathologic Basis of Disease
Mechanism 2: Anti-GBM Antibody Disease (Goodpasture Disease)
- Autoantibodies (IgG, usually IgG1/IgG3) are produced against α3(IV)NC1
- These bind directly and uniformly along the entire GBM → linear IgG pattern on immunofluorescence (distinguishes this from all immune complex diseases, which show granular deposits)
- Complement activation (classical pathway via C1q binding to IgG)
- Neutrophil recruitment via Fc-receptor engagement and C5a generation
- Severe GBM disruption → crescentic (rapidly progressive) GN + alveolar haemorrhage (if lung BM also attacked)
- HLA-DR2 (DRB1*1501) is strongly associated with susceptibility
Mechanism 3: ANCA-Associated (Pauci-Immune) GN
- c-ANCA (cytoplasmic) → anti-PR3 (proteinase 3) → Granulomatosis with polyangiitis (GPA, Wegener's)
- p-ANCA (perinuclear) → anti-MPO (myeloperoxidase) → Microscopic polyangiitis, Eosinophilic GPA (Churg-Strauss)
- ANCAs (IgG) are produced against neutrophil granule proteins (PR3 or MPO)
- Primed neutrophils (by cytokines like TNF, IL-8 from infection/inflammation) surface-express PR3/MPO
- ANCAs bind surface-expressed antigen → neutrophil activation
- Activated neutrophils release proteases, reactive oxygen species (ROS), and extracellular traps (NETs)
- These directly damage the glomerular endothelium and GBM
- GBM rupture → fibrin leaks into Bowman's space → crescent formation
- Minimal/no immune deposits on IF (pauci-immune) because no antigen is planted in the glomerulus
Mechanism 4: Complement-Mediated GN (C3 Glomerulopathy)
- Normally, Factor H inhibits C3b amplification; Factor I cleaves and inactivates C3b
- In C3 glomerulopathy: mutations in Factor H, Factor I, CD46, or C3; or autoantibodies against Factor H or C3 convertase (C3 nephritic factor)
- C3 convertase (C3bBb) becomes hyperactive and continuously cleaves C3
- C3b fragments deposit massively in the mesangium and GBM
- C5a generated → neutrophil recruitment → glomerular injury
- Dense deposit disease (MPGN type II): extremely electron-dense intramembranous deposits (sausage-shaped)
- C3 glomerulonephritis: mesangial and subendothelial C3 deposits
- IF shows C3 alone (no IgG/IgM)
"Alternative complement pathway activation occurs in the clinicopathologic entity called C3 glomerulopathy, which encompasses the entities of dense deposit disease and C3 glomerulonephritis."
- Robbins & Cotran Pathologic Basis of Disease
The Complement System in GN
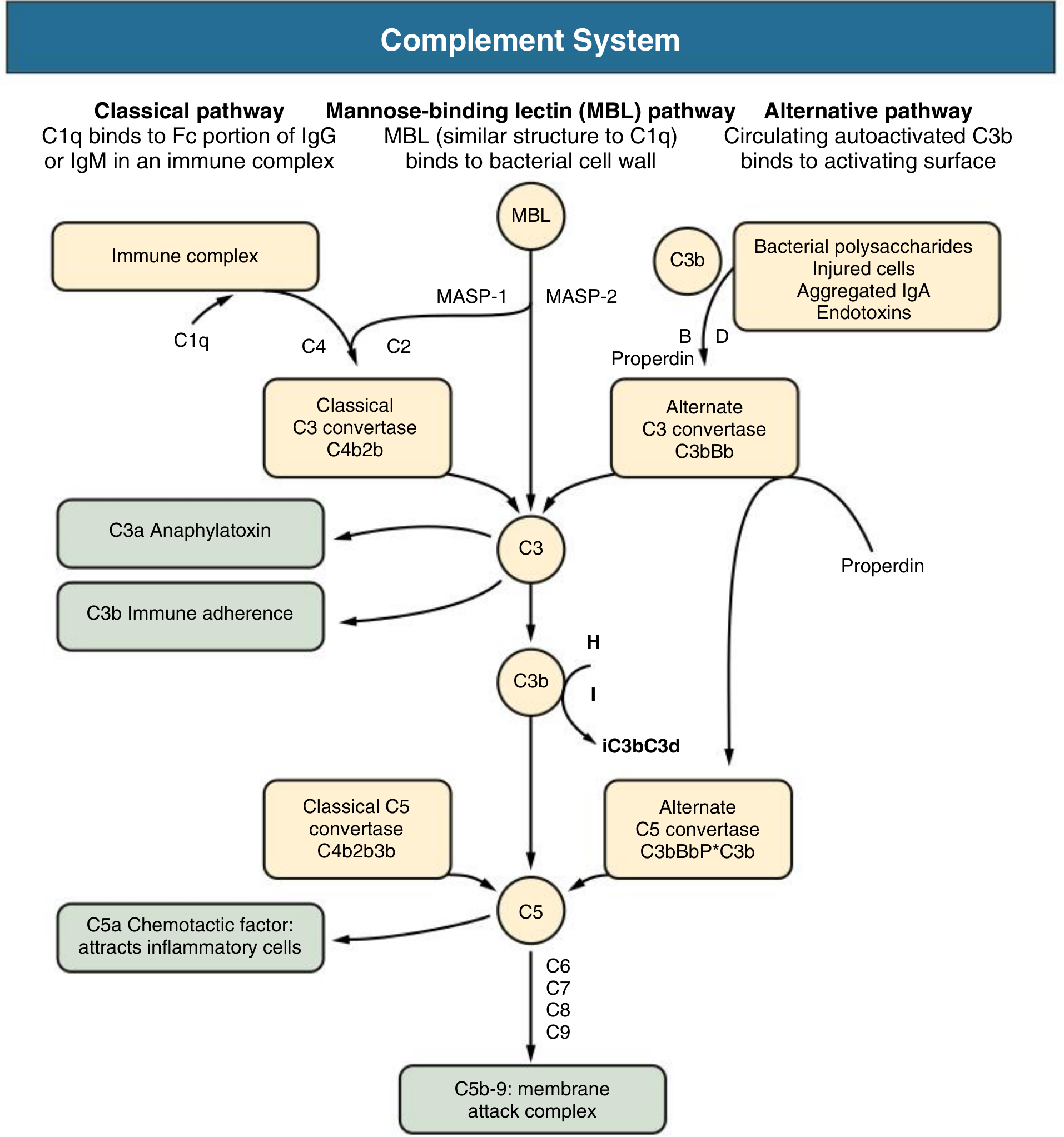
- C3a/C5a: anaphylatoxins - increase vascular permeability and recruit neutrophils/monocytes
- C5b-9 (MAC): directly lyses glomerular endothelial cells and podocytes
- C1q: bridges immune complexes to the classical pathway
- Loss of complement in serum (low C3, C4) is a diagnostic clue to immune complex disease (SLE, post-streptococcal GN, MPGN)
Mechanism 5: Cell-Mediated (T-Cell) Immunity
"T cells likely have a role in crescentic nephritis, becoming sensitized to endogenous or exogenous antigen and then recruiting macrophages that mediate crescent formation."
- Comprehensive Clinical Nephrology, 7th Edition
- Regulatory T cells (Tregs, CD4+/CD25+) normally suppress autoreactive responses; their failure allows GN to develop
- Activated T cells and macrophages release cytokines (IL-1, TNF-α, IFN-γ) and TGF-β that drive proliferation and fibrosis
- Minimal change disease (MCD): thought to be a T-cell disorder - a soluble factor (possibly CD80 or a suPAR-like molecule) produced by T cells damages podocyte foot processes directly, without immune deposits
Effector Cells and Mediators - Downstream Injury
| Cell/Mediator | Role |
|---|---|
| Neutrophils | Release proteases (degrade GBM), ROS (cell damage), arachidonic acid metabolites (reduce GFR) |
| Macrophages | Release IL-1, TNF, MMP, TGF-β; main effectors in crescent formation |
| Platelets | Aggregate in injured glomeruli; release eicosanoids and growth factors |
| Mesangial cells | Become myofibroblast-like; proliferate; produce excess ECM |
| Podocytes | Foot process effacement when injured; lose slit diaphragm → massive proteinuria |
| C5a | Key chemotactic signal attracting neutrophils/monocytes |
| TGF-β | Drives matrix deposition and glomerulosclerosis |
| PDGF | Drives mesangial cell proliferation |
Crescent Formation - The Final Common Pathway in Severe GN
Summary Table: Immunological Mechanisms by Disease
| GN Type | Immunological Mechanism | IF Pattern | Complement | Specific Marker |
|---|---|---|---|---|
| Post-streptococcal GN | Circulating immune complexes (streptococcal antigens) | Granular IgG + C3 ("starry sky") | Low C3 | ASO titre ↑ |
| Lupus nephritis | Immune complexes (DNA-anti-dsDNA); all Ig classes | Granular "full house" (IgG, IgA, IgM, C1q, C3) | Low C3, C4 | ANA, anti-dsDNA |
| IgA nephropathy | Mesangial IgA immune complexes (galactose-deficient IgA1) | Mesangial IgA dominant | Normal C3 | Serum galactose-deficient IgA1 ↑ |
| Membranous nephropathy | In situ subepithelial complexes (anti-PLA2R) | Granular IgG subepithelial | Normal or low C3 | Anti-PLA2R antibody |
| MPGN (type I) | Subendothelial immune complexes | Granular C3 ± IgG | Low C3 (and C4) | HCV, cryoglobulins |
| C3 glomerulopathy | Alternative complement pathway dysregulation | C3 only (no Ig) | Very low C3; normal C4 | C3 nephritic factor, Factor H mutation |
| Goodpasture disease | Anti-GBM IgG (anti-α3 type IV collagen) | Linear IgG | Normal | Anti-GBM antibody |
| ANCA-associated GN | ANCA-activated neutrophil injury | Pauci-immune (negative/trace) | Normal | PR3-ANCA or MPO-ANCA |
| Minimal change disease | T-cell-derived circulating factor (podocyte injury) | Negative (no deposits) | Normal | None (diagnosis of exclusion) |
Investigations required before starting hemodialysis
investigations required before starting hemodialysis pre-dialysis workup KDOQI guidelines
Investigations Required Before Starting Hemodialysis
1. Confirm & Quantify Renal Failure
| Investigation | Purpose | Expected Finding in ESRD |
|---|---|---|
| Serum creatinine | Estimate GFR | Markedly elevated; GFR < 15 mL/min/1.73m² (CKD stage 5) |
| Blood urea nitrogen (BUN) / Urea | Uraemic load; pre-dialysis BUN needed to calculate Kt/V and URR | Elevated (BUN > 80-100 mg/dL typically) |
| eGFR (CKD-EPI or MDRD) | KDOQI: decision to initiate dialysis based primarily on symptoms + metabolic status, not a fixed GFR threshold | < 15 mL/min; clinical symptoms guide timing |
| 24-hour urine creatinine clearance | Confirms GFR, assesses residual renal function | Reduced |
| Serum cystatin C | More accurate GFR estimate in low muscle-mass patients | Elevated |
KDOQI (2015) recommends: "The decision to initiate maintenance dialysis should be based primarily on an assessment of attributable complications of kidney failure, including signs/symptoms of uremia, protein-energy wasting, and development of metabolic or volume disturbances refractory to medical therapy - rather than a specific GFR level."
2. Identify the Underlying Cause of CKD
| Investigation | Purpose |
|---|---|
| Urinalysis + microscopy | Proteinuria, haematuria, casts (RBC casts = GN; waxy casts = CKD); protein:creatinine ratio |
| 24-hr urine protein | Quantify proteinuria |
| Urine electrolytes (Na, K, urea) | Distinguish prerenal vs intrinsic renal failure |
| Renal biopsy (if cause unknown and kidneys not shrunken) | Histological diagnosis |
| Renal ultrasound | Kidney size, corticomedullary differentiation, obstruction, cysts - small shrunken kidneys = chronic irreversible disease |
| Anti-dsDNA, ANA | Lupus nephritis |
| ANCA (anti-PR3, anti-MPO) | Vasculitis-associated GN |
| Anti-GBM antibody | Goodpasture disease |
| C3, C4 complement | Low in immune complex disease (SLE, MPGN, post-strep) |
| Serum protein electrophoresis / serum free light chains | Myeloma-related kidney disease |
| HbA1c, fasting glucose | Diabetic nephropathy (most common cause of ESRD worldwide) |
| Blood pressure history / echocardiogram | Hypertensive nephropathy |
3. Haematological Investigations
| Investigation | Purpose |
|---|---|
| Full blood count (FBC/CBC) | Anaemia of CKD (normochromic, normocytic); thrombocytopaenia in TTP/HUS; leucocytosis in infection |
| Peripheral blood smear | Microangiopathic haemolytic anaemia in HUS/TTP |
| Reticulocyte count | Assess erythropoietic response |
| Serum iron, ferritin, TIBC, transferrin saturation | Iron status before starting ESAs (erythropoiesis-stimulating agents); ferritin > 200 ng/mL and TSAT > 20% required before ESA therapy |
| Serum B12 and folate | Exclude nutritional anaemia |
| PTH (parathyroid hormone - intact) | Secondary hyperparathyroidism of CKD; drives renal osteodystrophy |
| Coagulation profile (PT, APTT, INR, bleeding time) | Uraemic platelet dysfunction; needed before vascular access surgery |
| Blood group and Rh typing | For potential transfusions; also important if kidney transplant is anticipated (sensitisation risk) |
| Crossmatch | If transfusion anticipated |
4. Metabolic / Biochemical Panel
| Investigation | Target/Significance |
|---|---|
| Serum electrolytes (Na, K, Cl, HCO3) | Hyperkalaemia (life-threatening); metabolic acidosis (bicarb < 22 mEq/L) |
| Serum calcium | Hypocalcaemia (from reduced 1,25-OH2 Vit D synthesis) |
| Serum phosphate | Hyperphosphataemia (phosphate retention in CKD) |
| Serum magnesium | Hypermagnesaemia in CKD |
| Serum albumin | Marker of nutritional status and inflammation; hypoalbuminaemia = poor prognosis |
| Serum uric acid | Elevated in CKD; gout risk |
| Serum glucose / HbA1c | Diabetes management; HbA1c may be unreliable in severe anaemia |
| Lipid profile (cholesterol, TG, HDL, LDL) | Cardiovascular risk assessment; dyslipidaemia common in CKD |
| LFTs (ALT, AST, ALP, GGT, bilirubin) | Baseline before dialysis; hepatitis co-infection common in dialysis units |
| Serum alkaline phosphatase | Bone disease/renal osteodystrophy |
| Serum 25-OH Vitamin D | Vitamin D deficiency; drives secondary hyperparathyroidism |
| Thyroid function tests (TSH, free T4) | Hypothyroidism common in CKD; affects dialysis tolerance |
5. Infection Screening (MANDATORY - for safe unit cohorting)
| Serology | Purpose |
|---|---|
| Hepatitis B surface antigen (HBsAg) | Active HBV infection - must dialyse in segregated area |
| Hepatitis B surface antibody (anti-HBs) | Immune status - if < 10 IU/L, vaccinate BEFORE starting dialysis (vaccine response is better with residual renal function) |
| Hepatitis B core antibody (anti-HBc IgG) | Past HBV exposure; inactive carrier status |
| Hepatitis C antibody (anti-HCV) | HCV seropositivity - segregate; treat with DAAs before/during dialysis |
| HCV RNA (PCR) | Confirm active HCV replication, especially if antibody positive |
| HIV antibody (anti-HIV 1 & 2) | Patients on dialysis require special precautions if positive |
| VDRL/RPR (syphilis screening) | Standard blood-borne infection screen |
| Tuberculosis screening (Mantoux / IGRA) | Immunosuppressed patients; prior to renal transplant listing |
| CMV IgG / IgM | Baseline; critical if transplant is anticipated |
| EBV serology | Transplant baseline |
| Varicella zoster antibody | Vaccinate seronegative patients before immunosuppression |
6. Cardiovascular Assessment
| Investigation | Purpose |
|---|---|
| ECG (12-lead) | Baseline rhythm; LVH (from longstanding hypertension); hyperkalaemia changes (peaked T waves, wide QRS) |
| Echocardiogram (2D + Doppler) | Left ventricular hypertrophy (present in >75% of ESRD patients); ejection fraction; pericardial effusion; valvular calcification |
| Chest X-ray | Cardiomegaly; pulmonary oedema; pleural effusions; pericardial effusion |
| Blood pressure (bilateral) | Hypertension management; bilateral BP for AVF planning (use arm with higher BP) |
| Peripheral pulse assessment + ABI | Peripheral vascular disease - impacts AVF placement success |
| Troponin I/T (baseline) | Often chronically elevated in CKD; need baseline to interpret future acute elevations |
| NT-proBNP / BNP | Cardiac function; volume status |
7. Vascular Access Investigations
| Investigation | Purpose |
|---|---|
| Venous duplex ultrasound (forearm + upper arm veins) | Map veins for AVF creation; vein diameter ≥ 2 mm and depth ≤ 6 mm needed for successful AVF; identify stenoses from previous cannulation |
| Arterial duplex ultrasound / Allen's test | Assess radial/brachial artery diameter and flow; Allen's test rules out hand ischaemia |
| CT venography / MR venography | If central venous stenosis suspected (prior central lines); assess subclavian/SVC patency for tunnelled catheter placement |
| Chest X-ray | Central venous anatomy; prior catheter-related stenosis |
Per KDOQI: An AV fistula should ideally be placed at least 6 months before anticipated start of hemodialysis to allow adequate time for maturation. Patients who reach CKD stage 4 (GFR < 30 mL/min) should begin access planning.
8. Nutritional Assessment
| Investigation | Purpose |
|---|---|
| Serum albumin | Malnutrition marker; target > 4.0 g/dL |
| Serum pre-albumin (transthyretin) | Sensitive nutritional marker; short half-life (2 days) |
| Serum transferrin | Nutritional iron-binding protein |
| Normalised protein catabolic rate (nPCR) | Dietary protein intake; calculated from pre-dialysis BUN; target 1.0-1.2 g/kg/day |
| Anthropometrics (BMI, mid-arm circumference) | Sarcopaenia assessment |
9. Immunological / Transplant-Related (If Transplant Anticipated)
| Investigation | Purpose |
|---|---|
| HLA typing (A, B, DR) | Required for transplant matching; place on waiting list |
| Panel reactive antibody (PRA) | Degree of sensitisation from prior transfusions/pregnancies/transplants |
| Blood group (ABO) | Transplant compatibility |
Summary Checklist
| Domain | Key Tests |
|---|---|
| Renal function | Creatinine, BUN/urea, eGFR, 24-hr urine |
| Cause of CKD | Urinalysis, USS kidneys, autoimmune serology |
| Haematology | FBC, iron studies, coagulation, blood group |
| Electrolytes/metabolic | Na, K, HCO3, Ca, PO4, glucose, lipids, albumin, PTH |
| Infection screen | HBsAg, anti-HBs, anti-HCV + HCV PCR, HIV, VDRL |
| Cardiac | ECG, echo, CXR, BP, troponin baseline |
| Vascular access | Venous and arterial duplex USS |
| Nutrition | Albumin, pre-albumin, nPCR |
| Transplant work-up | HLA typing, PRA (if candidate) |
Management of acute atypical pneumonia
"atypical pneumonia" AND "macrolide" AND "treatment guidelines"
"community acquired pneumonia" AND "guidelines" AND "azithromycin"
IDSA ATS 2019 community acquired pneumonia guidelines atypical pneumonia treatment macrolide doxycycline
Management of Acute Atypical Pneumonia
What is "Atypical" Pneumonia?
- Cannot be cultured on standard blood/chocolate agar
- Do not respond to beta-lactam antibiotics (penicillins, cephalosporins) - they either lack a cell wall or have intracellular survival
- Produce a clinical picture of gradual onset, dry/hacking cough, low-grade fever, and extrapulmonary features disproportionate to the chest findings ("walking pneumonia")
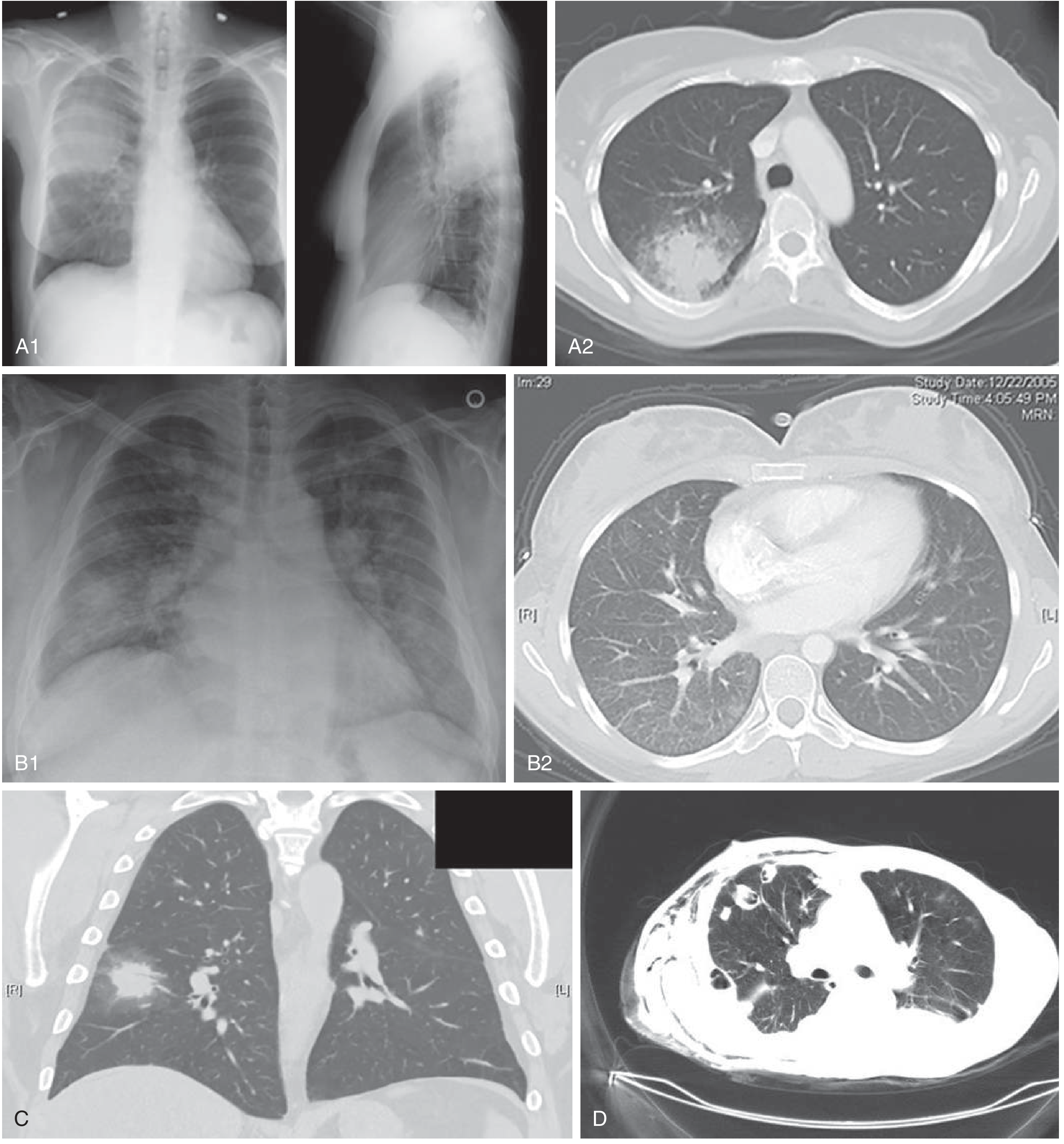
- Show interstitial (rather than lobar) infiltrates on CXR
Causative Organisms
| Organism | Key Features |
|---|---|
| Mycoplasma pneumoniae | Most common atypical; young adults; gradual onset; dry cough; extrapulmonary manifestations (rash, haemolytic anaemia, CNS) |
| Chlamydophila (Chlamydia) pneumoniae | Gradual onset; sore throat + hoarseness before cough (biphasic illness); elderly |
| Legionella pneumophila | Severe; Pontiac fever or Legionnaires' disease; water source; diarrhoea, hyponatraemia, high LDH, high ferritin |
| Coxiella burnetii | Q fever; occupational (abattoir, farm); systemic illness, hepatitis, culture-negative endocarditis |
| Chlamydia trachomatis | Neonates; staccato cough, afebrile pneumonitis |
| Francisella tularensis | Tularaemia pneumonia; rare; bioterrorism concern |
"Levofloxacin or azithromycin are preferred for treatment [of Legionella]."
- Sherris & Ryan's Medical Microbiology 8th Edition
Clinical Features of Atypical Pneumonia (vs. Typical)
| Feature | Typical (e.g., S. pneumoniae) | Atypical (Mycoplasma, Chlamydophila, Legionella) |
|---|---|---|
| Onset | Acute (hours) | Gradual (days to weeks) |
| Cough | Productive, purulent | Dry, hacking, nonproductive |
| Fever | High, with rigors | Low-grade (except Legionella) |
| Pleuritic pain | Common | Uncommon |
| Appearance | Toxic | "Walking pneumonia" - not toxic |
| CXR | Lobar/segmental consolidation | Bilateral interstitial/patchy infiltrates |
| WBC | Leukocytosis (neutrophilia) | Normal or mildly elevated |
| Extrapulmonary | Rare | Common - see below |
| Response to β-lactams | Good | None |
Extrapulmonary Manifestations of Mycoplasma Pneumoniae:
- Haemolytic anaemia (cold agglutinins)
- Stevens-Johnson syndrome
- Erythema multiforme
- Meningoencephalitis, Guillain-Barré syndrome, transverse myelitis
- Myopericarditis
- Arthritis, rhabdomyolysis
Diagnosis
| Investigation | Notes |
|---|---|
| Clinical diagnosis (empirical) | Mainstay in ED and outpatient settings; specific testing rarely changes acute management |
| CXR | Bilateral interstitial or lower lobe patchy infiltrates; may be worse than clinical examination suggests |
| CT chest | More sensitive; ground-glass opacities, tree-in-bud pattern |
| Multiplex PCR (nasopharyngeal swab / BAL) | BioFire and similar panels detect Mycoplasma, Chlamydophila, Legionella, influenza simultaneously - increasingly the preferred rapid diagnostic |
| Legionella urinary antigen | Detects serogroup 1 (accounts for ~80% of cases); highly sensitive and specific; rapid result; essential for suspected Legionella |
| Pneumococcal urinary antigen | Distinguishes from typical pneumonia |
| Serology (acute + convalescent titres, 4-fold rise) | Mycoplasma IgM/IgG; Chlamydophila IgM/IgG; Legionella IFA; Coxiella CF - takes 4-6 weeks; not useful for acute management |
| Cold agglutinins (IgM) | >1:64 suggests Mycoplasma; non-specific; rarely used now |
| Sputum culture | Atypicals do not grow on standard media; requires special conditions |
| Blood cultures | Mandatory in hospitalised patients (low yield for atypicals but rules out bacteraemia) |
| FBC, CRP, procalcitonin | WBC often normal in atypical; procalcitonin typically lower than bacterial typical pneumonia |
| LFTs, Na, LDH, ferritin | Legionella: hyponatraemia, elevated LDH, elevated ferritin, deranged LFTs are classic |
| ABG / pulse oximetry | Severity assessment |
Antibiotic Treatment
Treatment by Clinical Setting
A. Outpatient - Mild Atypical Pneumonia (no comorbidities)
| Drug | Dose | Duration |
|---|---|---|
| Amoxicillin 1 g TDS | First choice (covers typical + some atypical cross-coverage) | 5 days |
| Doxycycline 100 mg BD | Excellent atypical coverage; preferred if atypical suspected; well tolerated | 5 days |
| Azithromycin 500 mg day 1, then 250 mg od | Covers all atypicals; use only if pneumococcal macrolide resistance <25% locally | 5 days |
| Clarithromycin 500 mg BD | Alternative macrolide | 5 days |
Per IDSA 2019: "For healthy outpatient adults without comorbidities, we recommend amoxicillin 1 g TDS, or doxycycline 100 mg BD, or a macrolide (only in areas with pneumococcal resistance <25%)."
B. Outpatient - With Comorbidities (diabetes, CKD, cardiac/lung disease, smoker)
| Regimen | Drugs |
|---|---|
| β-lactam + macrolide | Amoxicillin-clavulanate OR cefuroxime + azithromycin/clarithromycin |
| β-lactam + doxycycline | Amoxicillin-clavulanate + doxycycline |
| Respiratory fluoroquinolone monotherapy | Levofloxacin 750 mg od OR moxifloxacin 400 mg od |
C. Inpatient - Non-Severe (ward admission)
| Regimen | Drugs | Notes |
|---|---|---|
| β-lactam + macrolide | IV/PO ceftriaxone 1-2 g od + azithromycin 500 mg od | Standard first-line |
| β-lactam + doxycycline | Ceftriaxone + doxycycline 100 mg BD | When macrolide intolerant or QTc prolonged |
| Respiratory fluoroquinolone monotherapy | IV/PO levofloxacin 750 mg od OR moxifloxacin 400 mg od | Equivalent efficacy to combination |
Recent meta-analysis [PMID: 37385561, 2023]: Respiratory fluoroquinolone monotherapy vs β-lactam + macrolide combination showed comparable outcomes in hospitalised CAP - supports guideline flexibility.
D. Inpatient - Severe CAP / ICU Admission (at least 1 major criterion: septic shock OR mechanical ventilation)
| Regimen | Drugs |
|---|---|
| Standard severe CAP | IV β-lactam (ceftriaxone or ampicillin-sulbactam) + IV azithromycin 500 mg od |
| Alternative severe CAP | IV β-lactam + IV levofloxacin 750 mg od (if macrolide contraindicated) |
| + MRSA suspected | Add vancomycin or linezolid |
| + Pseudomonas suspected | Switch to antipseudomonal β-lactam (piperacillin-tazobactam or cefepime) |
Organism-Specific Treatment
Mycoplasma pneumoniae
| Drug | Dose | Duration |
|---|---|---|
| Azithromycin (first-line) | 500 mg day 1, 250 mg od | 5 days |
| Doxycycline (first-line) | 100 mg BD | 5-7 days |
| Levofloxacin | 750 mg od | 5 days |
| Moxifloxacin | 400 mg od | 5 days |
| No cell wall - completely ineffective | - | |
| Emerging in Asia/Europe; use doxycycline or fluoroquinolone | - |
Chlamydophila (Chlamydia) pneumoniae
| Drug | Dose | Duration |
|---|---|---|
| Doxycycline (first-line) | 100 mg BD | 10-14 days (longer - intracellular organism) |
| Azithromycin | 500 mg od | 5-7 days |
| Levofloxacin | 750 mg od | 7-14 days |
Legionella pneumophila (Legionnaires' Disease)
| Drug | Dose | Duration | Notes |
|---|---|---|---|
| Levofloxacin (preferred) | 750 mg IV/PO od | 5-14 days | Fluoroquinolones achieve highest intracellular concentrations; clinical cure faster |
| Azithromycin (preferred) | 500 mg IV/PO od | 5-10 days | Good intracellular penetration; IV initially for severe cases |
| Moxifloxacin | 400 mg od | 10-14 days | Alternative |
| Less preferred for Legionella | - | Lower intracellular activity vs fluoroquinolones | |
| Ineffective (intracellular organism) | - | - |
"Levofloxacin or azithromycin are preferred for treatment [of Legionella]."
- Sherris & Ryan's Medical Microbiology 8th Edition
Coxiella burnetii (Q Fever)
| Drug | Dose | Duration |
|---|---|---|
| Doxycycline (drug of choice) | 100 mg BD | 14 days (acute Q fever) |
| Doxycycline + hydroxychloroquine | Long-term | 18+ months (Q fever endocarditis) |
Supportive Management
| Measure | Details |
|---|---|
| Oxygen therapy | Maintain SpO2 > 94% (>88% in COPD); high-flow nasal cannula or NIV for hypoxic respiratory failure |
| Antipyretics | Paracetamol/ibuprofen for fever and pleuritic pain |
| IV fluids | If tachycardic, hypotensive, or not tolerating oral intake |
| Adequate hydration | Promotes mucociliary clearance |
| Chest physiotherapy | In severe cases with mucus retention |
| Antitussives | For severe, distressing dry cough (dextromethorphan, codeine); use cautiously |
| Corticosteroids | Not routinely recommended; IDSA 2019 suggests consideration in severe CAP with refractory septic shock (prednisolone 40-50 mg/day for 5-7 days) |
| Bronchodilators | If wheeze/bronchospasm (common with Mycoplasma) |
Duration of Treatment and Step-Down
- Minimum 5 days for non-severe CAP (IDSA/ATS 2019)
- Patient must be afebrile for ≥48 hours and clinically stable before stopping
- IV to oral switch when: haemodynamically stable + tolerating oral intake + improving clinically (same-day switching is now endorsed in guidelines)
- Macrolide-resistant Mycoplasma (increasing in Asia): switch to doxycycline or respiratory fluoroquinolone
Severity Assessment (PSI / CURB-65)
- Confusion
- Urea > 7 mmol/L
- Respiratory rate ≥ 30/min
- BP systolic < 90 or diastolic ≤ 60 mmHg
- 65 years or older
| Score | Mortality | Management |
|---|---|---|
| 0-1 | < 3% | Outpatient |
| 2 | 9% | Short inpatient stay or supervised outpatient |
| 3-5 | 15-40% | Hospital admission; consider ICU if ≥ 4 |
Summary Antibiotic Algorithm
Atypical CAP suspected
│
▼
Severity assessment
(CURB-65 / PSI)
│
┌─────┴──────┐
│ │
Outpatient Inpatient
│ │
▼ ┌───┴────────┐
Doxycycline │ │
100mg BD Non-severe Severe/ICU
OR │ │
Azithromycin│ β-lactam + │ β-lactam +
500/250mg Azithromycin │ IV azithromycin
OR OR β-lactam +│ OR
Respiratory │ doxycycline│ β-lactam +
FQL OR FQL mono │ IV levofloxacin
5 days 5 days 5-14 days