Blood Brain barrier anatomy
Reading File
Finding Sources
Searching PubMed
"blood-brain barrier" anatomy structure
Reading File
Reading File
Reading File
Loading Image
Loading Image
Loading Image
Reading File
I now have rich, comprehensive content from multiple authoritative textbooks plus great diagrams. Let me compile the full answer.
Blood-Brain Barrier (BBB) - Anatomy
Historical Discovery
The BBB was first demonstrated by Paul Ehrlich in 1885 when he injected aniline dyes intravenously and found that virtually all body organs stained - except the brain. The dye-albumin complex passes freely across capillaries throughout the body but is excluded from the CNS. This selective exclusion defines the blood-brain barrier.
Structural Components
The BBB is not a single structure but a composite of several cellular elements forming the neurovascular unit:
1. Endothelial Cells (the primary barrier)
The BBB resides in the single layer of uninterrupted vascular endothelial cells lining the continuous (non-fenestrated) capillaries of the CNS. These cells differ fundamentally from systemic capillary endothelial cells:
| Feature | Systemic Capillaries | Brain Capillaries |
|---|---|---|
| Junctions | Fenestrations / clefts (leaky) | Tight junctions (sealed) |
| Permeability | High - free passage of fluids/solutes | Restricted - transcellular transport only |
| Pinocytosis | Active | Severely restricted |
| Solute passage | Paracellular | Transcellular only |
Tight junctions between brain endothelial cells are structurally more similar to epithelial tight junctions than to those found between ordinary endothelial cells. They eliminate gaps between cells and prevent simple diffusion of solutes and fluid into neural tissue. Substances with a molecular weight greater than 500 Da generally cannot cross the BBB.
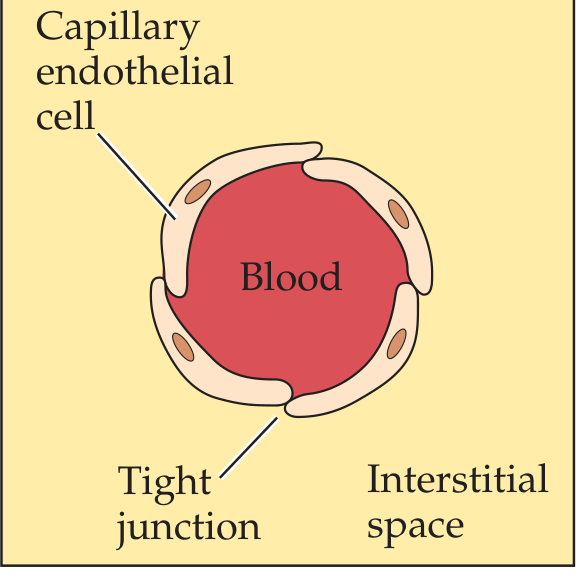
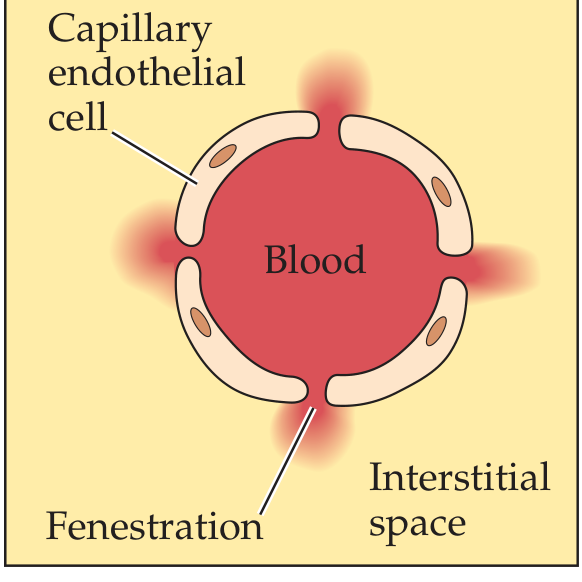
Brain capillary (right) vs. systemic fenestrated capillary (left) - note tight junctions vs. fenestrations
2. Basement Membrane
The endothelial cells rest on a continuous basal lamina (basement membrane). Astrocyte end-feet closely associate with this basal lamina, but do not themselves form the physical barrier.
3. Astrocyte End-Feet (Perivascular Feet)
Astrocytes extend end-foot processes that wrap around the outer surface of the capillary and contact the endothelial basal lamina. Although the end-feet do not physically block passage, they:
- Maintain the integrity of the tight junctions (the BBB depends on normal astrocyte function)
- Release soluble factors that increase barrier properties and tight junction protein content
- Regulate water homeostasis via aquaporin-4 (AQP4) water channels in the end-feet
- Buffer extracellular K+ concentration
Breakdown of the BBB in disease is associated with loss of tight junctions AND alterations in astrocyte morphology.
4. Pericytes
Pericytes are embedded within the basement membrane alongside the endothelium. They regulate capillary diameter, contribute to tight junction formation, and participate in immune surveillance.
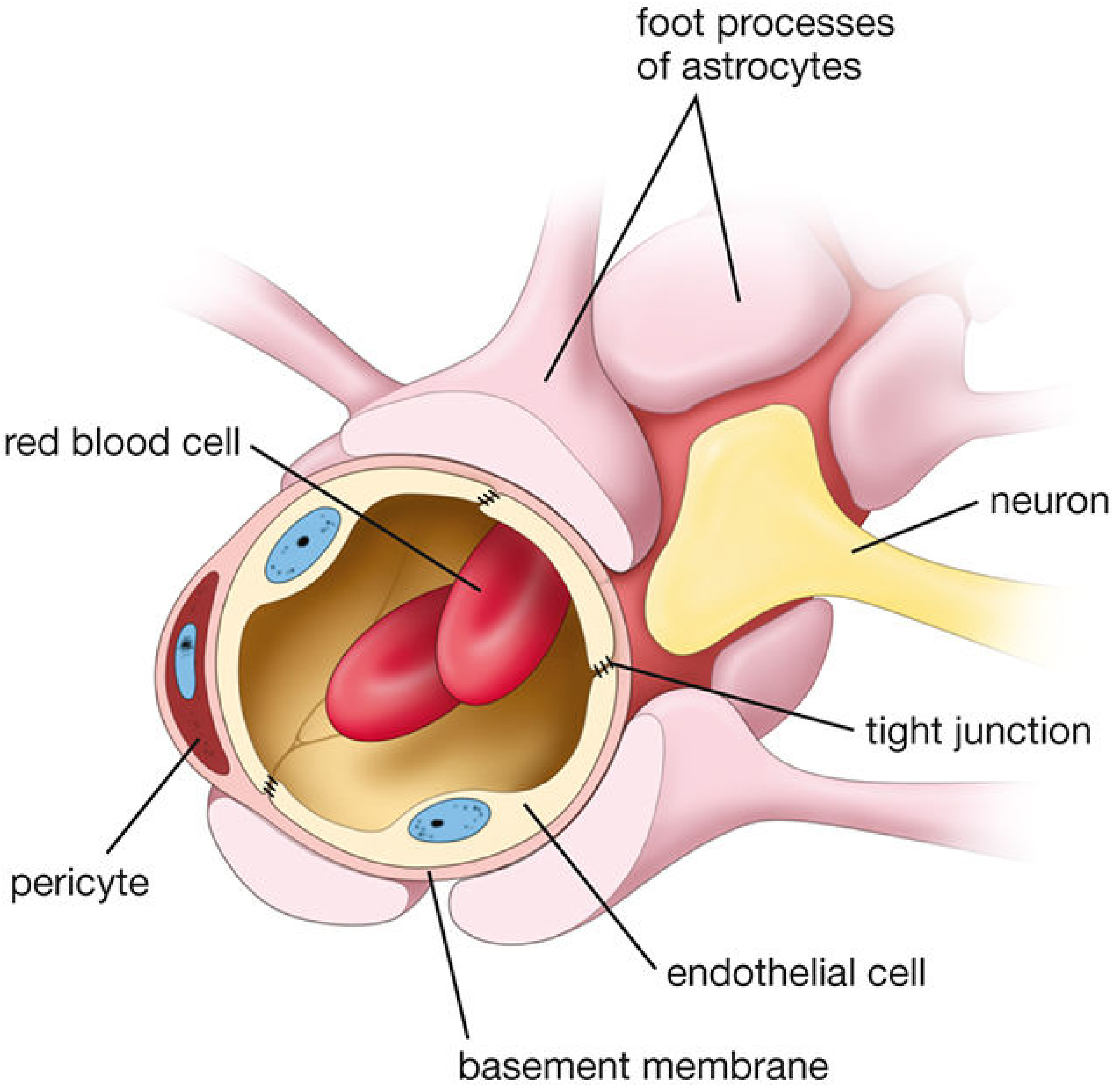
The neurovascular unit: endothelial cells with tight junctions, basement membrane, pericytes, astrocyte foot processes, and adjacent neuron.
Development
The BBB develops early in the embryo through an interaction between glial astrocytes and capillary endothelial cells. The astrocyte-endothelial signaling relationship is essential both for establishment and maintenance of barrier properties.
Functions
The BBB serves three main roles:
- Protection - excludes blood-borne toxins, pathogens, immune mediators, and fluctuating levels of hormones/amino acids (e.g., dietary amino acids that act as neurotransmitters would cause chaos if freely entering the brain)
- Metabolic supply - active transport of glucose, amino acids, ions, nucleotides, and vitamins into the CNS
- Homeostasis - maintains the optimal ionic microenvironment for neuronal function (e.g., controlling K+ and H+ levels that would otherwise alter membrane potentials)
Transport Across the BBB
Passage across the BBB is tightly controlled:
| Mechanism | Substances |
|---|---|
| Free diffusion | O2, CO2, lipid-soluble molecules (ethanol, steroid hormones) |
| Facilitated transport (SLC superfamily) | Glucose via GLUT1, cationic amino acids via SLC7A1 |
| Active efflux (ABC transporters) | Drugs, toxins, metabolic waste - transported OUT against concentration gradient |
| Receptor-mediated transcytosis | Insulin, transferrin, large proteins |
| Enzymatic metabolism | Drugs and foreign proteins metabolized within endothelial cell membrane |
Clinical example: Dopamine cannot cross the BBB, so dopamine deficiency (Parkinson's disease) is treated with its precursor L-DOPA, which does cross via amino acid transporters. L-DOPA is then converted to dopamine within the brain.
Blood-CSF Barrier (a related but distinct barrier)
The choroid plexus presents a separate but related barrier:
- Choroid plexus capillaries are fenestrated (leaky), unlike brain capillaries
- The barrier here is formed by the choroid plexus epithelial cells linked by tight junctions (not the capillary wall)
- This blood-CSF barrier regulates CSF composition
Similarly, arachnoid villi allow one-way bulk flow of CSF into venous sinuses via giant vacuoles.
Circumventricular Organs - Areas Lacking a BBB
Several midline structures bordering the 3rd and 4th ventricles are outside the BBB. These are supplied by fenestrated (leaky) capillaries:
| Circumventricular Organ | Function |
|---|---|
| Area postrema | Chemoreceptor trigger zone (vomiting) |
| Posterior pituitary | Hormone release (ADH, oxytocin) |
| Median eminence | Hypothalamic-pituitary portal signaling |
| Organum vasculosum of lamina terminalis (OVLT) | Osmoreception, fluid balance |
| Subfornical organ | Angiotensin sensing, fluid balance |
| Subcommissural organ | CSF composition |
| Pineal gland | Melatonin secretion |
At these sites, ependymal cells overlying the leaky capillaries (especially at the choroid plexus, median eminence, and area postrema) are joined by tight junctions that form a local BECF-CSF barrier, preventing the variability of blood composition from reaching the CSF.
BBB Breakdown in Disease
Loss of tight junctions and astrocyte dysfunction characterize BBB disruption in:
- Stroke / ischemia
- Multiple sclerosis
- Meningitis / encephalitis
- Brain tumors
- Alzheimer's disease
- Traumatic brain injury
Sources: Neuroanatomy through Clinical Cases, 3rd Ed. | Histology: A Text and Atlas, 9th Ed. | Medical Physiology (Boron & Boulpaep)
Recent review: A 2025 review in Brain (PMID 39969549) covers current understanding of the BBB as both a protective barrier and a hindrance to CNS drug delivery, reinforcing the anatomical principles above.
Csf Anatomy
Finding Sources
Finding Sources
Finding Sources
Finding Sources
Finding Sources
Reading File
Reading File
Reading File
Loading Image
Loading Image
Loading Image
Reading File
Loading Image
Loading Image
Reading File
Reading File
I now have everything needed for a comprehensive, well-illustrated answer. Let me compile it.
Cerebrospinal Fluid (CSF) - Anatomy
Overview
CSF is a colorless, watery liquid that fills the ventricles of the brain and forms a thin layer around the outside of the brain and spinal cord in the subarachnoid space. The choroid plexus can be thought of as the brain's "kidney" - it stabilizes the composition of CSF just as the kidney stabilizes blood plasma. The normal total CSF volume in an adult is about 150 mL, produced at a rate of ~500 mL/day (20 mL/hour).
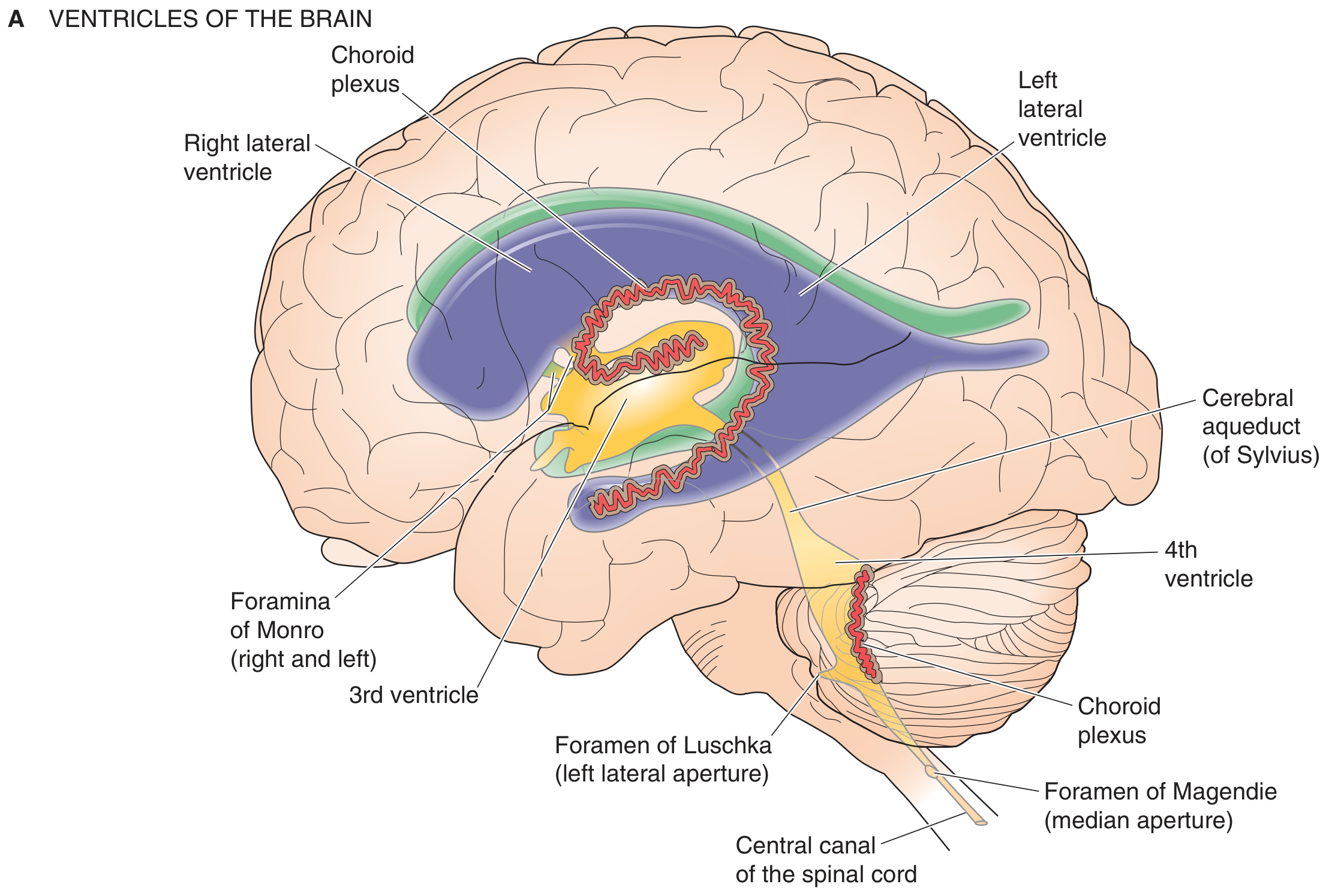
1. Ventricular System (Sites of CSF Production)
The brain contains four ventricles, each containing a choroid plexus and filled with CSF. They are connected by channels (foramina) allowing CSF to move between them.
| Ventricle | Location | Connection |
|---|---|---|
| Lateral ventricles (x2) | Within cerebral hemispheres (C-shaped) | To 3rd ventricle via foramina of Monro |
| 3rd ventricle | Midline; walls formed by thalamus & hypothalamus | To 4th ventricle via cerebral aqueduct of Sylvius |
| 4th ventricle | Roof = cerebellum; floor = pons & medulla | To subarachnoid space via foramina of Luschka (x2, lateral) and Magendie (x1, midline) |
Each lateral ventricle has:
- An anterior (frontal) horn
- A body
- An atrium (trigone) - where body, occipital horn, and temporal horn converge
- A posterior (occipital) horn
- An inferior (temporal) horn
2. Choroid Plexus - CSF Production
The choroid plexus is a highly vascularized epithelial structure found in all four ventricles. It produces CSF by active secretion.
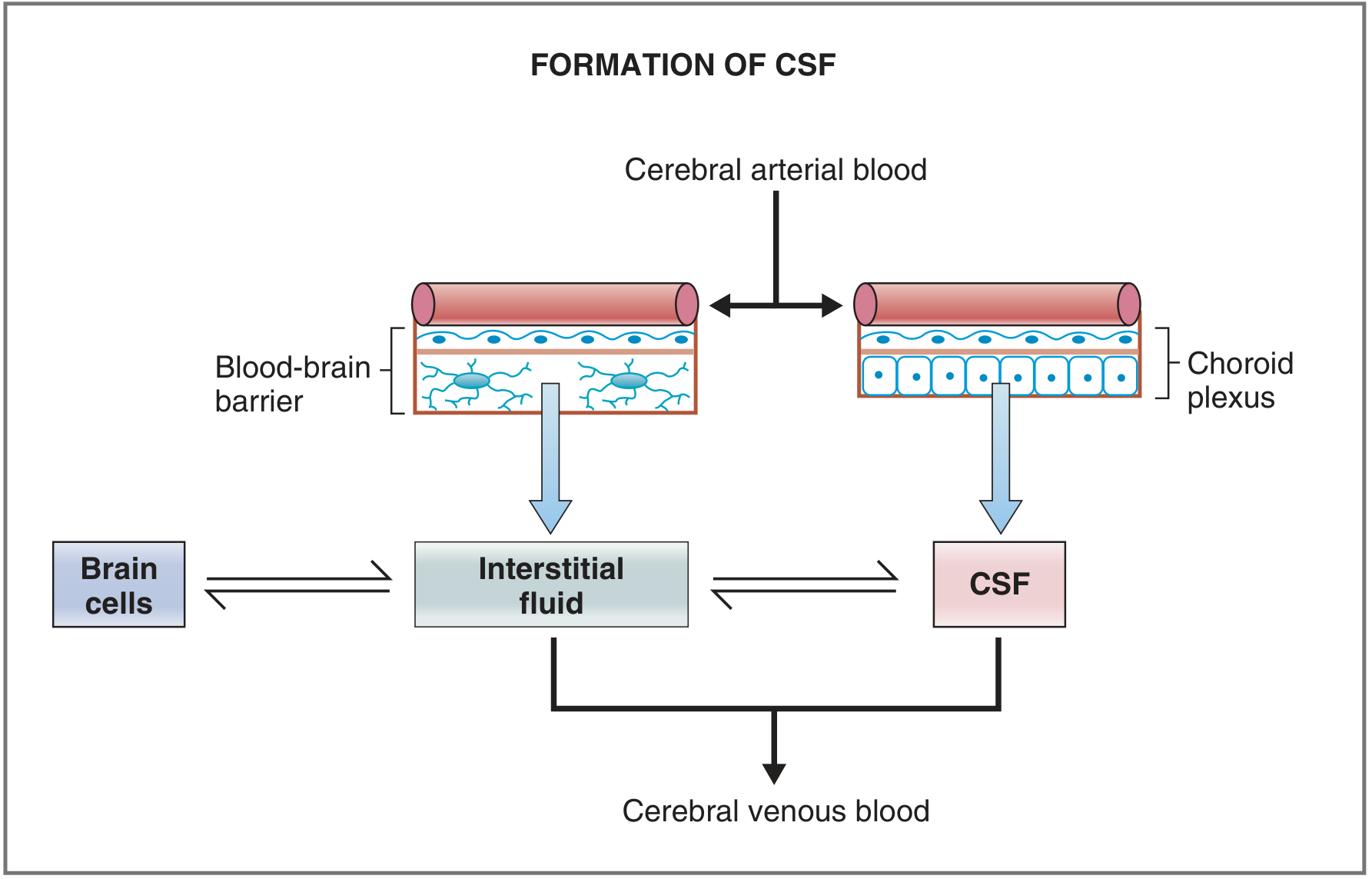
The blood-CSF barrier at the choroid plexus consists of three layers:
- Capillary endothelial cells + basement membrane (fenestrated - leaky capillaries here)
- Neuroglial membrane
- Choroid plexus epithelial cells linked by tight junctions (this is where the barrier actually resides)
The epithelial cells resemble renal distal tubule cells and actively transport:
- Into CSF (secretion): Na+, Cl-, HCO3-, water
- Out of CSF (absorption): K+
- Excluded from CSF: Protein, cholesterol (too large)
3. CSF Composition
| [CSF] = [Blood] | [CSF] < [Blood] | [CSF] > [Blood] |
|---|---|---|
| Na+ | K+ | Mg2+ |
| Cl- | Ca2+ | Creatinine |
| HCO3- | Glucose | |
| Osmolarity | Amino acids | |
| pH | ||
| Cholesterol (negligible) | ||
| Protein (negligible) |
Lipid-soluble substances (O2, CO2, ethanol, steroid hormones) cross freely between blood and CSF. Brain interstitial fluid and CSF have similar compositions to each other, but both differ from blood.
4. CSF Circulation Pathway
CSF flows in a directed, pressure-driven circuit:
Choroid plexus (lateral ventricles) → Foramina of Monro → 3rd ventricle → Cerebral aqueduct of Sylvius → 4th ventricle → Foramina of Luschka (x2) + Foramen of Magendie (x1) → Subarachnoid space → Arachnoid granulations → Superior sagittal sinus → venous blood
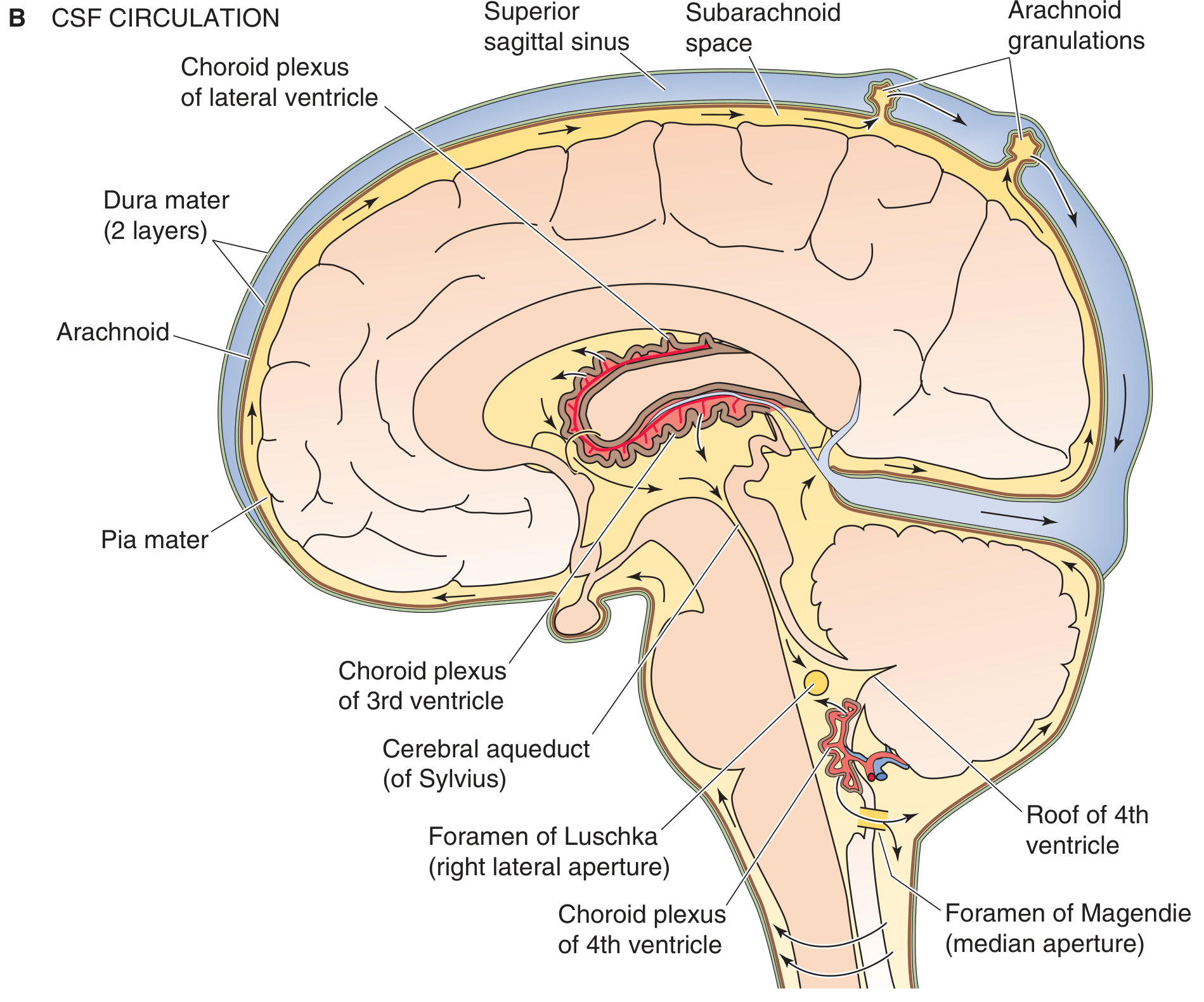
5. Subarachnoid Space and Cisterns
The subarachnoid space lies between the arachnoid mater and pia mater (together called the leptomeninges). It is traversed by trabeculae (collagen strands) and contains CSF, blood vessels, and cranial nerve roots.
The space widens at several locations to form cisterns (larger CSF pools):
| Cistern | Location | Clinical Relevance |
|---|---|---|
| Ambient cistern (cisterna ambiens) | Lateral to midbrain | |
| Quadrigeminal cistern | Posterior to midbrain, below splenium of corpus callosum | Named for 4 colliculi |
| Interpeduncular cistern | Ventral midbrain, between cerebral peduncles | CN III exits here |
| Prepontine cistern | Ventral to pons | Contains basilar artery, CN VI |
| Cisterna magna (cerebellomedullary) | Between cerebellum and medulla | Site for cisternal tap |
| Lumbar cistern | L2-S2; spinal cord ends at L1-L2 | Site for lumbar puncture |
6. Meningeal Layers (Surrounding CSF)
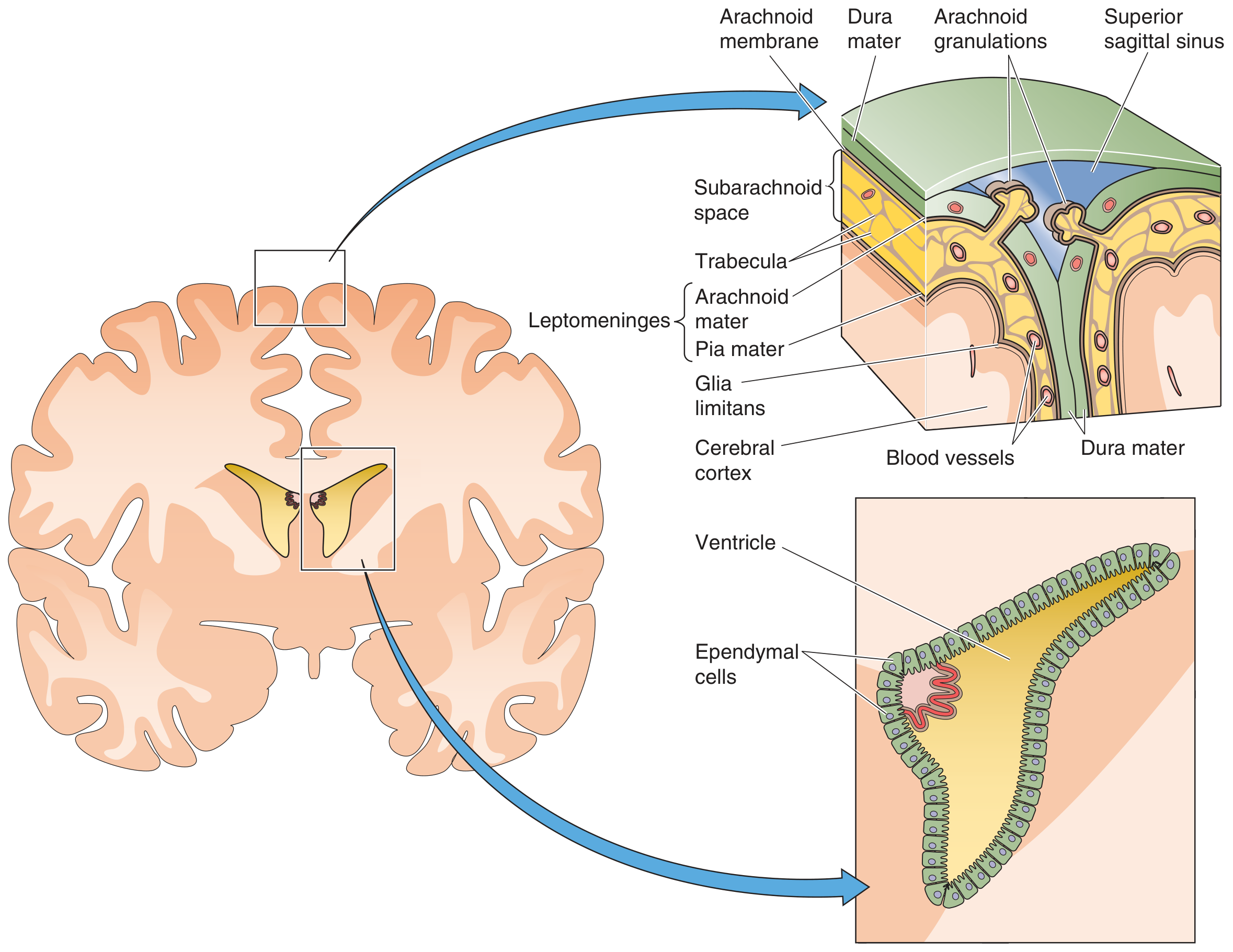
| Layer | Key Features |
|---|---|
| Dura mater | Outermost, tough; 2 layers in cranium (periosteal + meningeal); 1 layer in spine; contains dural venous sinuses |
| Arachnoid mater | Middle; cells joined by tight junctions; avascular; separated from dura by potential subdural space |
| Subarachnoid space | Contains CSF, trabecular strands, arteries, veins |
| Pia mater | Innermost; closely adheres to brain surface (glia limitans); follows every sulcus and gyrus |
Ependymal cells line the interior surfaces of the ventricles. They have cilia that help propel CSF flow.
7. CSF Absorption
CSF is absorbed at arachnoid villi (microscopic) and arachnoid granulations (macroscopic, up to 1 cm, also called Pacchionian granulations) - specialized evaginations of the arachnoid membrane through the dura mater into the venous sinuses.
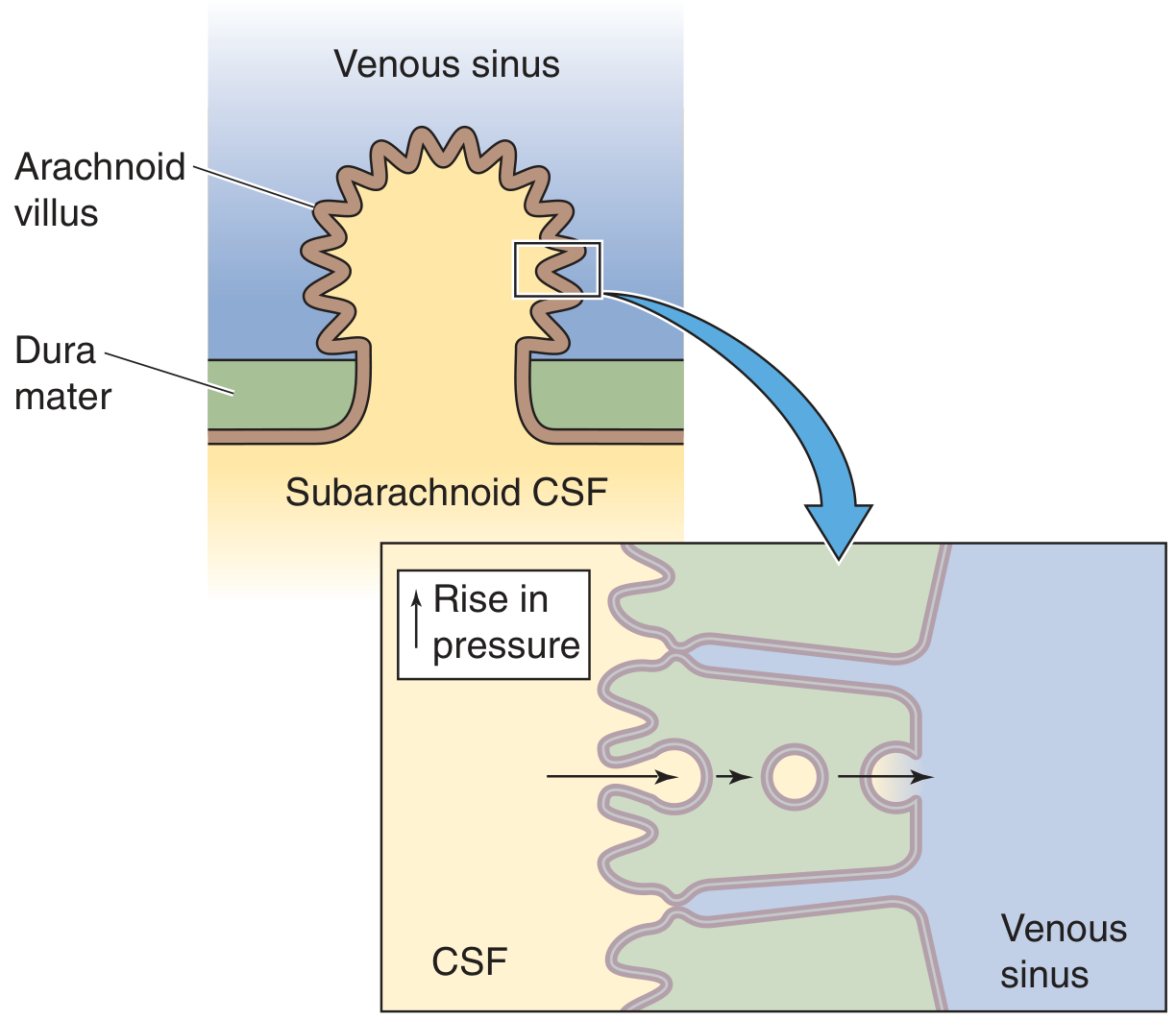
Key features of absorption:
- One-way valve - CSF can enter venous blood, but venous blood cannot enter CSF
- Mechanism involves transcytosis or giant fluid-containing vacuoles crossing arachnoid epithelial cells
- Absorption begins when CSF pressure exceeds ~70 mm H2O and increases proportionally with further pressure rise
- CSF formation rate is insensitive to pressure changes; only absorption changes - this is the pressure-stabilizing mechanism
- Minor absorption also occurs via spinal veins and along cranial nerve sheaths
8. Functions of CSF
- Mechanical cushioning - protects the brain from trauma (buoyant support reduces effective brain weight from ~1400 g to ~50 g)
- Chemical homeostasis - provides a controlled ionic environment separate from fluctuating blood composition
- Waste removal - clears metabolic byproducts and neurotransmitters from the CNS
- Intracranial pressure regulation - adjustable volume buffer (Monro-Kellie doctrine)
- Neurohumoral signaling - transports hormones and neuropeptides within the CNS
9. Clinical Correlates
| Condition | Mechanism | Key Point |
|---|---|---|
| Obstructive hydrocephalus | Block at cerebral aqueduct (most common site) | CSF cannot exit ventricles |
| Communicating hydrocephalus | Impaired absorption at arachnoid villi (e.g., after SAH, meningitis) | All ventricles dilate |
| Normal-pressure hydrocephalus | Damaged arachnoid villi; intermittently elevated pressure | Triad: dementia, incontinence, gait disturbance; treat with VP shunt |
| Lumbar puncture | L2-S2 lumbar cistern; spinal cord ends at L1-L2 in adults | CT/MRI first to exclude raised ICP (risk of herniation) |
| Herniation | Expanding mass forces brain through foramen magnum | Lumbar puncture contraindicated with mass lesion |
Sources: Medical Physiology (Boron & Boulpaep), p. 423-427 | Costanzo Physiology, 7th Ed. | Neuroanatomy through Clinical Cases, 3rd Ed., p. 162
This is a shared conversation. Sign in to Orris to start your own chat.