Give me a description on meconium aspiration syndrome
Reading File
Finding Sources
Searching PubMed
"meconium aspiration syndrome"[MeSH Terms]
Finding Sources
Reading File
Reading File
Reading File
Loading Image
I now have comprehensive content from three authoritative textbooks plus a chest X-ray. Here is the full description:
Meconium Aspiration Syndrome (MAS)
Definition
Meconium aspiration syndrome is a clinical diagnosis defined by three criteria occurring together: delivery through meconium-stained amniotic fluid (MSAF), the presence of respiratory distress in the newborn, and a characteristic chest X-ray appearance. Confirmation requires demonstrating meconium below the level of the vocal cords. - Creasy & Resnik's Maternal-Fetal Medicine, p. 1789; Grainger & Allison's Diagnostic Radiology, p. 1780
Meconium-Stained Amniotic Fluid (MSAF)
Meconium is present in the fetal intestine from the second trimester. Maturation of the intestinal smooth muscle and myenteric plexus progresses through the third trimester, which is why intrauterine passage of meconium is unusual before 36 weeks. The physiologic stimuli for meconium passage are not fully understood, but clinical and epidemiologic data strongly suggest that a stressed fetus may pass meconium before birth.
- MSAF complicates 4%-22% of all deliveries
- More frequent in post-term pregnancies
- Infants born through MSAF tend to have lower umbilical artery pH values and are associated with non-reassuring fetal heart rate tracings
MAS proper, however, occurs in only 1%-2% of all MSAF deliveries, though reported incidence varies widely. - Creasy & Resnik's, p. 1789
Pathophysiology
MAS involves multiple simultaneous mechanisms rather than a single process:
1. Airway Obstruction
Meconium is a thick, viscous substance. When aspirated, it migrates to the distal airways and may cause:
- Complete obstruction - leading to segmental atelectasis
- Partial obstruction ("ball-valve" effect) - leading to air trapping and overinflation
- Alternating zones of atelectasis and hyperinflation throughout the lungs
2. Chemical Pneumonitis
Meconium triggers a direct inflammatory reaction in the lung parenchyma, causing chemical pneumonitis. This inflammatory component is independent of the mechanical obstruction.
3. Surfactant Inactivation
Meconium inactivates surfactant, compounding respiratory failure and reducing lung compliance.
4. Pulmonary Arterial Hypertension (PPHN)
This is a major complication and a primary driver of severity. Chronic fetal hypoxia in the third trimester increases the amount of muscle in the blood vessels of the distal respiratory units. This pulmonary vascular remodeling leads to persistently elevated pulmonary vascular resistance after birth - persistent pulmonary hypertension of the newborn (PPHN). In infants who die from MAS with PPHN, muscle extends into the most peripheral intra-acinar arteries, which are normally non-muscular in term newborns. - Barash Clinical Anesthesia, p. 3580; Creasy & Resnik's, p. 1789
Clinical Features
- Respiratory distress at birth (tachypnea, grunting, retractions, cyanosis)
- Barrel-shaped chest from air trapping
- Low Apgar scores common in severe cases
- Non-reassuring fetal heart rate tracing before delivery
- Severity ranges from mild respiratory distress to catastrophic respiratory failure
Hallmarks of severe disease include:
- Need for positive-pressure ventilation
- Presence of pulmonary hypertension (PPHN)
Severe MAS carries significant risks: air leak syndromes, chronic lung disease, and developmental delay.
Radiographic Features
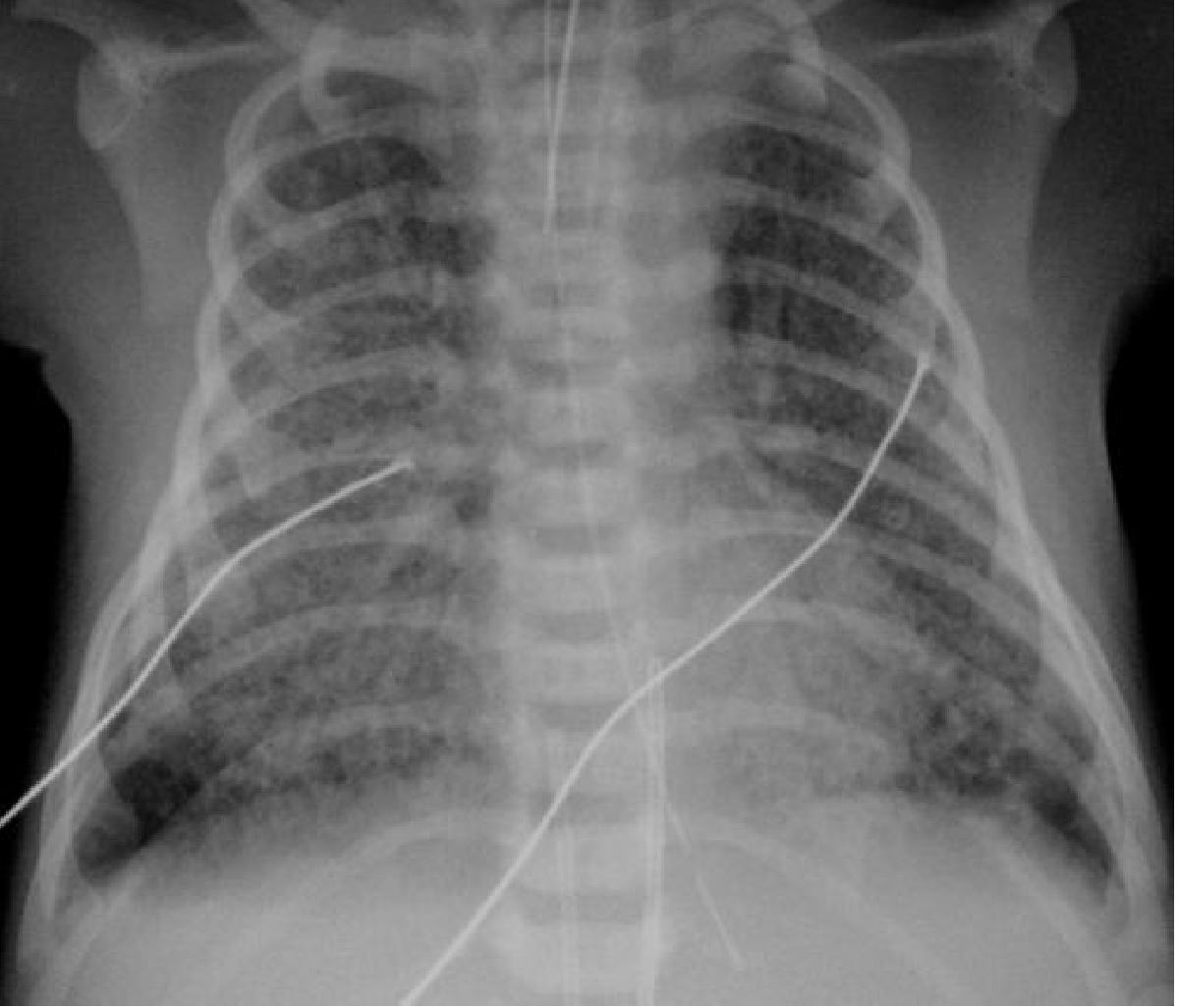
Fig. 70.13 - Infant born at 42 weeks' gestation: bilateral hyperinflation, small left pleural effusion, and asymmetrical coarse opacification in keeping with meconium aspiration. - Grainger & Allison's Diagnostic Radiology, p. 1780
Key X-ray findings include:
- Bilateral hyperinflation (flattened diaphragms, increased AP diameter)
- Asymmetrical coarse patchy opacification (from atelectasis and inflammation)
- Pleural effusions (small, often unilateral)
- Air leaks - pneumothorax and pneumomediastinum are common complications (seen in up to ~30% of mechanically ventilated cases)
Prevention Strategies
Guidelines on intrapartum and peripartum management have evolved significantly:
- Induction at 41 weeks reduces MSAF incidence and MAS compared to expectant management (systematic review evidence)
- Amnioinfusion to dilute thick meconium does NOT reduce MAS incidence or perinatal morbidity in settings with appropriate peripartum surveillance - it is not recommended for this purpose
- Routine oropharyngeal suctioning on the perineum (before shoulder delivery) was once universal practice but was abandoned after evidence showed no benefit
- Routine tracheal intubation and suctioning of vigorous infants is no longer recommended (Wiswell et al., 2000; ILCOR 2005, 2015)
- Selective intubation is now practiced: if the newborn is depressed (not vigorous), tracheal intubation and suctioning remains appropriate - Creasy & Resnik's, p. 1789; Barash Clinical Anesthesia, p. 3581
Management
Mild-Moderate MAS
- Supplemental oxygen
- Supportive respiratory care
- Monitoring for deterioration
Severe MAS
- Mechanical ventilation - required in approximately 30% of affected infants
- Inhaled nitric oxide (iNO) - selective pulmonary vasodilator used to treat severe PPHN; has significantly improved mortality
- Surfactant therapy - counters meconium-mediated surfactant inactivation
- High-frequency oscillatory ventilation (HFOV) - used when conventional ventilation fails
- Extracorporeal Membrane Oxygenation (ECMO) - reserved for infants where all conventional treatments have failed; can be delivered as:
- VA-ECMO (veno-arterial): catheter via internal jugular vein and common carotid artery - supports both cardiac and pulmonary function when pulmonary vascular resistance is very high
- VV-ECMO (veno-venous): double-lumen catheter via internal jugular vein into right atrium - supports gas exchange only
The use of iNO and ECMO has substantially improved survival in severe MAS. - Grainger & Allison's, p. 1780
Summary
| Feature | Details |
|---|---|
| Incidence | 1-2% of MSAF deliveries; MSAF in 4-22% of all births |
| Risk factors | Post-term gestation, fetal hypoxia, non-reassuring FHR |
| Key mechanisms | Airway obstruction, chemical pneumonitis, surfactant inactivation, PPHN |
| Hallmark CXR | Bilateral hyperinflation, coarse patchy opacification, air leaks |
| Mechanical ventilation needed | ~30% of cases |
| Severe complications | Pneumothorax, PPHN, chronic lung disease, developmental delay |
| Key therapies | iNO, surfactant, HFOV, ECMO |
Sources: Creasy & Resnik's Maternal-Fetal Medicine, 8e, p. 1789 | Grainger & Allison's Diagnostic Radiology, p. 1780 | Barash Clinical Anesthesia, 9e, p. 3580
This is a shared conversation. Sign in to Orris to start your own chat.