Thyroid gland
Reading File
Finding Sources
Finding Sources
Reading File
Reading File
Reading File
Reading File
Reading File
Reading File
Loading Image
Loading Image
Loading Image
Loading Image
Reading File
I now have comprehensive content from all four textbooks. Let me compile the full, detailed answer.
The Thyroid Gland
Anatomy
The thyroid gland is a butterfly-shaped endocrine organ located in the anterior neck, lying deep to the sternohyoid, sternothyroid, and omohyoid muscles. It consists of two lateral lobes connected by a thin isthmus, which crosses the anterior surfaces of the 2nd and 3rd tracheal cartilages. The lateral lobes cover the anterolateral surfaces of the trachea, the cricoid cartilage, and the lower thyroid cartilage. The gland sits in the visceral compartment of the neck, surrounded by the pretracheal fascia alongside the pharynx, trachea, and esophagus. - Gray's Anatomy for Students, p. 1157
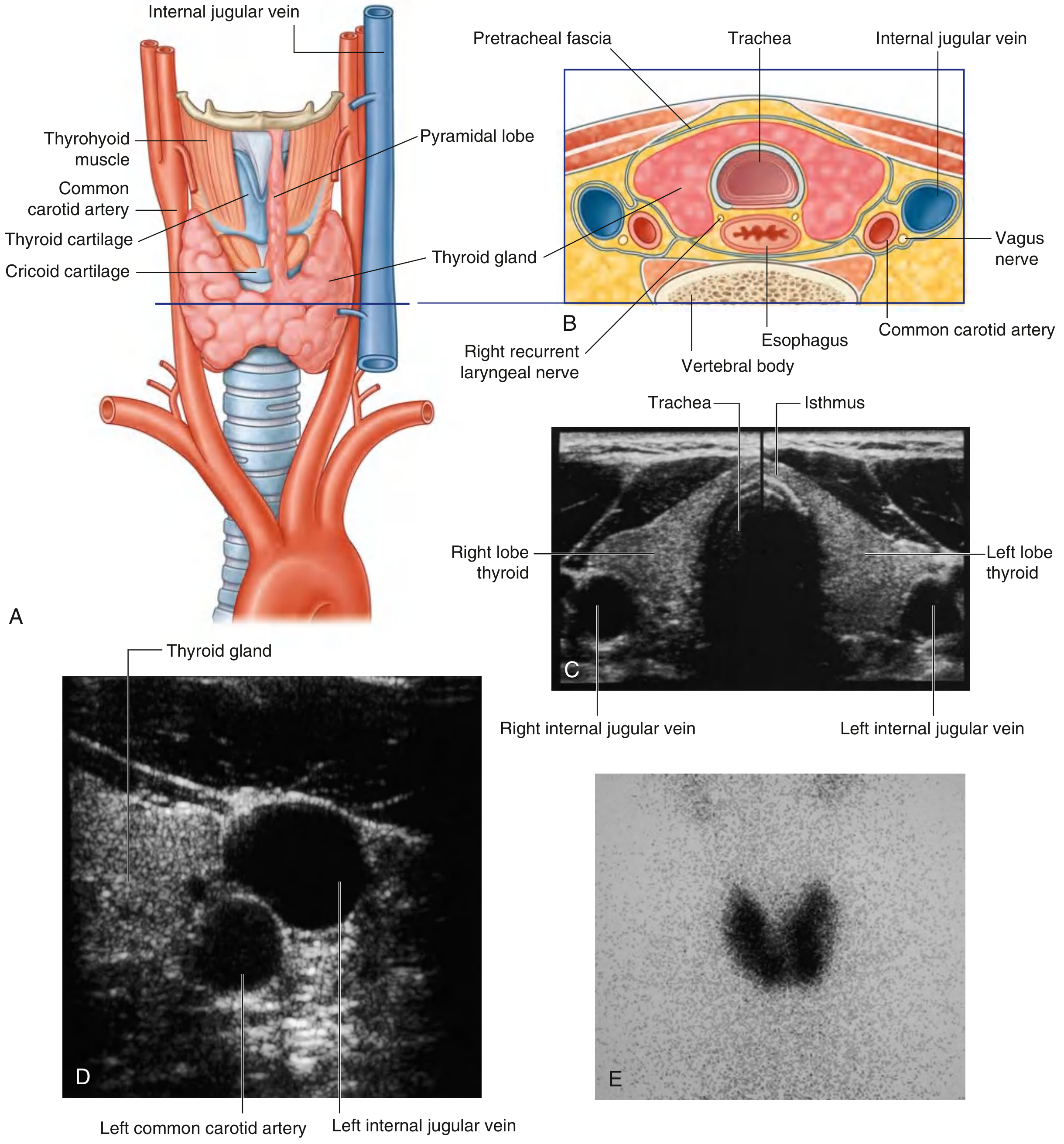
Fig. 8.181 - Thyroid gland in the anterior triangle of the neck (Gray's Anatomy for Students)
Arterial Supply
Two major arteries supply the thyroid:
- Superior thyroid artery - the first branch of the external carotid artery; descends to the superior pole and divides into anterior and posterior glandular branches
- Inferior thyroid artery - a branch of the thyrocervical trunk (from the 1st part of the subclavian artery); supplies the inferior pole and anastomoses with the superior thyroid artery
Venous Drainage
Three pairs of veins drain the thyroid:
- Superior thyroid vein - drains into the internal jugular vein
- Middle thyroid vein - drains into the internal jugular vein
- Inferior thyroid vein - drains into the brachiocephalic vein
Important Relationships
- Recurrent laryngeal nerve - runs posteriorly and is at risk during thyroid surgery
- Parathyroid glands - four in number, embedded in the posterior surface of the thyroid lobes
- External branch of the superior laryngeal nerve - runs close to the superior thyroid artery and can be injured during ligation
Embryology
The thyroid arises as a median outgrowth from the pharyngeal floor near the base of the tongue (foramen cecum). It migrates down via the thyroglossal duct to its final position in the anterior neck. The duct normally disappears but remnants can persist as:
- Thyroglossal duct cyst (most common neck mass in children)
- Lingual thyroid (ectopic thyroid at base of tongue)
- Pyramidal lobe (upward extension along the duct path) - Robbins Pathologic Basis of Disease, p. 995
Histology
The thyroid is the only endocrine gland that stores its secretory product outside cells - in the colloid. It is divided by fibrous septa into lobules, each containing 20-40 follicles.
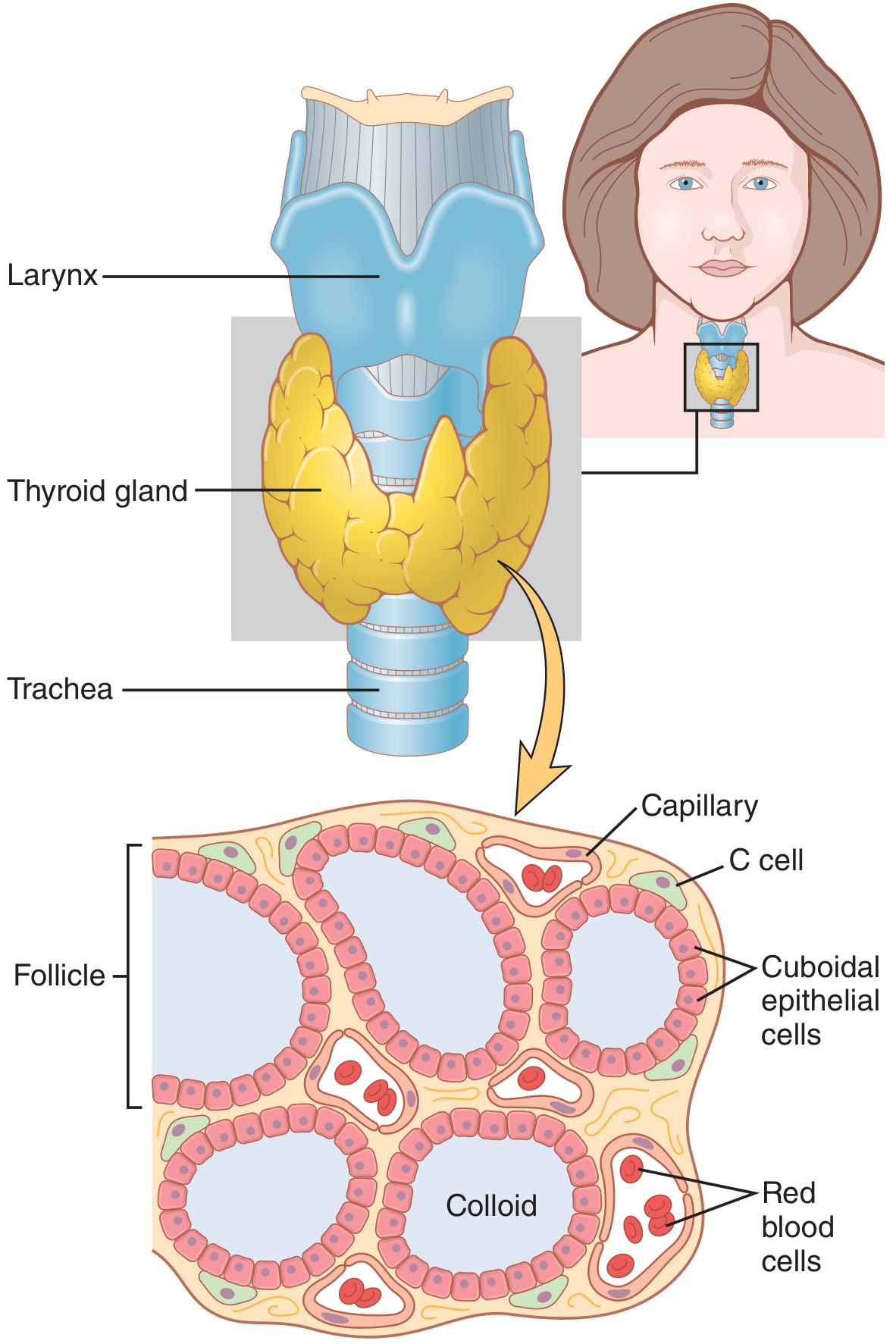
Figure 77.1 - Anatomy and microscopic structure of the thyroid gland (Guyton & Hall Medical Physiology)
Two Cell Types
| Feature | Follicular cells (Thyrocytes) | Parafollicular cells (C cells) |
|---|---|---|
| Location | Line the follicle | In/between follicles |
| Size | Smaller, darker staining | Larger, pale staining |
| Shape | Squamous to low columnar (varies with activity) | Constant in size |
| Product | T3, T4 | Calcitonin |
| Regulation | TSH from anterior pituitary | Serum Ca²+ |
Activity reflects cell shape: Active glands show low columnar epithelium; hypoactive glands show squamous follicular cells. - Junqueira's Basic Histology, p. 1034
Follicular colloid: Contains the large glycoprotein thyroglobulin (660 kDa), the precursor for thyroid hormones. There is sufficient hormone stored in the follicles to supply the body for up to 3 months without additional synthesis.
The thyroid is extremely well vascularized - blood flow is about five times the weight of the gland per minute, comparable only to the adrenal cortex. - Guyton & Hall, p. 930
Hormone Synthesis
The HPT (hypothalamus-pituitary-thyroid) axis controls hormone synthesis:
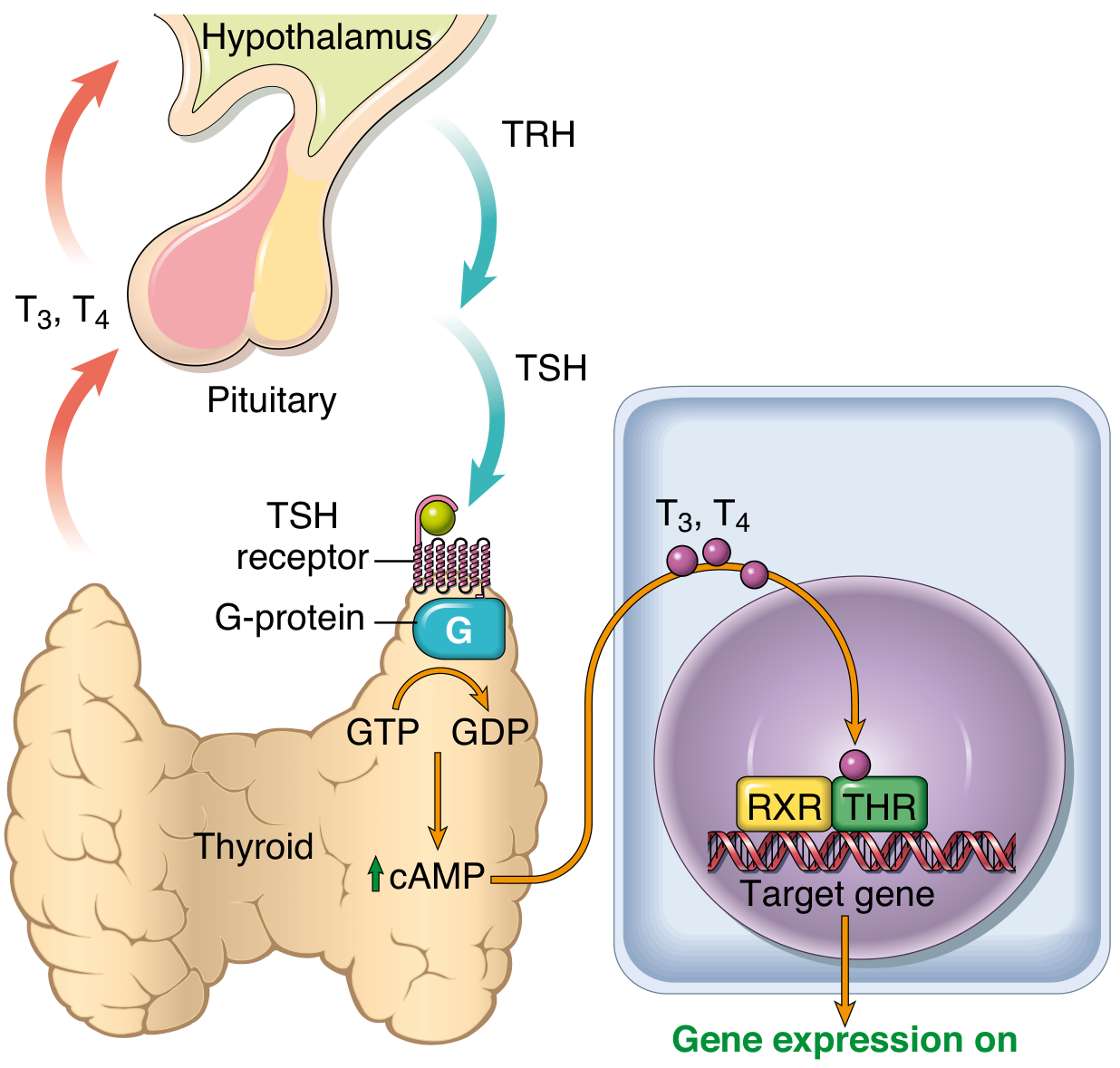
Fig. 24.8 - Hypothalamus-pituitary-thyroid axis and mechanism of action (Robbins Pathologic Basis of Disease)
Steps of Thyroid Hormone Synthesis
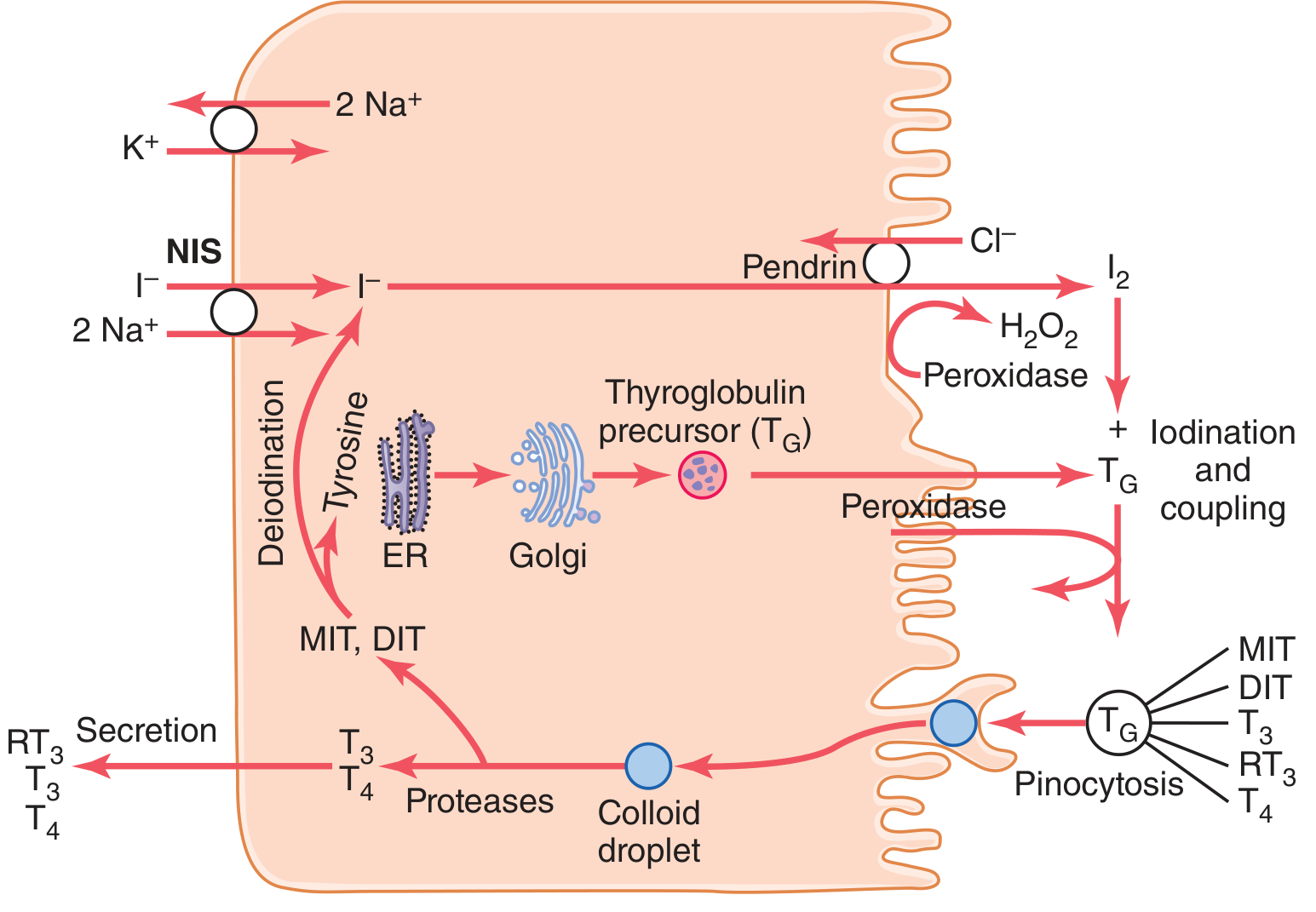
Figure 77.2 - Thyroid cellular mechanisms (Guyton & Hall Medical Physiology)
-
Iodide trapping - The sodium-iodide symporter (NIS) on the basolateral membrane co-transports 1 I⁻ with 2 Na⁺ into the cell (using Na⁺-K⁺-ATPase-driven gradient). Concentration ratio is normally ~30x blood, rising to 250x when maximally active.
-
Iodide transport to follicle - Iodide is moved across the apical membrane into the follicular lumen by pendrin (chloride-iodide counter-transporter).
-
Oxidation of iodide - Thyroid peroxidase (using H₂O₂) oxidizes iodide (I⁻) to active iodine (I₀ or I₃⁻) at the apical membrane.
-
Organification - Oxidized iodine binds tyrosine residues on thyroglobulin. Iodination of one tyrosine produces monoiodotyrosine (MIT); two iodines produces diiodotyrosine (DIT).
-
Coupling - MIT + DIT → T3 (triiodothyronine); DIT + DIT → T4 (thyroxine). Both remain within the thyroglobulin molecule until secretion.
-
Storage - Thyroid hormones are stored as part of thyroglobulin in the follicular colloid.
-
Secretion - TSH stimulates thyrocytes to pinocytose colloid droplets. Proteases cleave thyroglobulin to release free T3 and T4 into the bloodstream. MIT and DIT are deiodinated intracellularly, and iodide is recycled.
Iodine requirement: ~50 mg/year (~1 mg/week) of dietary iodine. Table salt is iodized at 1 part sodium iodide per 100,000 parts NaCl to prevent deficiency. - Guyton & Hall, p. 930-931
Circulating Hormones and Peripheral Conversion
- Most secreted hormone is T4 (85%), with smaller amounts of T3 (15%)
- In plasma, hormones are bound to thyroxine-binding globulin (TBG), transthyretin, and albumin - these act as a buffer maintaining stable free hormone levels
- In peripheral tissues, ~80% of T4 is deiodinated to T3 (the active form)
- T3 binds nuclear thyroid hormone receptors with 10-fold greater affinity than T4 and has proportionately greater biological activity
- T3 acts on the nucleus as a heterodimer with retinoid X receptor (RXR) at thyroid hormone response elements, activating or suppressing gene transcription - Robbins, p. 995
Kinetics of Action
| Hormone | Latent Period | Peak Effect | Half-life |
|---|---|---|---|
| T4 (thyroxine) | 2-3 days | 10-12 days | ~15 days |
| T3 (triiodothyronine) | 6-12 hours | 2-3 days | ~1 day |
Physiological Actions of Thyroid Hormones
Thyroid hormones activate nuclear transcription of many genes and increase the functional activity of virtually every cell in the body:
| System | Effect |
|---|---|
| Metabolism | Increases basal metabolic rate (BMR); stimulates carbohydrate and lipid catabolism; increases protein synthesis |
| Cardiovascular | Increases heart rate, cardiac output, and blood flow |
| Nervous system | Critical for fetal and neonatal brain development; maintains alertness and reflexes in adults |
| Growth | Promotes normal growth and skeletal maturation |
| Thermogenesis | Increases heat production (uncouples oxidative phosphorylation) |
| GI | Increases gut motility |
Calcitonin (C cells)
C cells (parafollicular cells) secrete calcitonin, a polypeptide hormone that:
- Is released in response to elevated serum calcium
- Lowers plasma calcium by inhibiting osteoclast activity (reducing bone resorption)
- Acts as a physiological antagonist to parathyroid hormone (PTH)
- Has clinical use as a marker for medullary thyroid carcinoma - Junqueira's Basic Histology, p. 1035; Guyton & Hall, p. 930
HPT Axis and Feedback Regulation
- Hypothalamus releases thyrotropin-releasing hormone (TRH)
- Anterior pituitary responds with thyroid-stimulating hormone (TSH/thyrotropin)
- TSH binds the TSH receptor on follicular cells → activates Gs protein → increases cAMP → stimulates thyroid hormone synthesis and release AND thyroid gland growth
- Elevated T3/T4 feeds back negatively to inhibit both TRH and TSH secretion
Mutations in thyroid hormone receptors:
- THRB (TR-beta) mutations → resistance to thyroid hormone, elevated T3/T4 levels (impaired feedback)
- THRA (TR-alpha) mutations → different phenotype with mildly low T4 but elevated T3/T4 ratio - Robbins, p. 995-996
Sources:
- Gray's Anatomy for Students (pp. 1157-1158) - Anatomy, blood supply, embryology
- Guyton & Hall Textbook of Medical Physiology (pp. 930-934) - Physiology, hormone synthesis
- Robbins & Cotran Pathologic Basis of Disease (pp. 995-996) - Pathology, HPT axis
- Junqueira's Basic Histology (pp. 1034-1036) - Histology, cell types, calcitonin
This is a shared conversation. Sign in to Orris to start your own chat.