Test in hernia
Reading File
Finding Sources
Finding Sources
Finding Sources
Reading File
Finding Sources
Finding Sources
Reading File
Reading File
Reading File
Reading File
Reading File
Loading Image
Reading File
I now have comprehensive content to provide a thorough answer on clinical tests in hernia.
Clinical Tests in Hernia
The Two Classical Signs of an Uncomplicated Hernia
According to S Das - Manual on Clinical Surgery:
Two classical signs of an uncomplicated hernia are: (i) Impulse on coughing and (ii) Reducibility.
Examination Protocol
The patient is examined first lying down, then standing (hernias increase in size on standing). Coughing or the Valsalva manoeuvre is used to make the hernia appear. Divarication is best seen asking a supine patient to lift their head off the pillow.
- Bailey and Love's Short Practice of Surgery, 28th ed.
Test 1 - Impulse on Coughing (Cough Impulse Test)
Technique: Place gentle pressure over the lump and ask the patient to cough.
- Positive: An expansile (outward push) impulse is felt - confirms intra-abdominal communication.
- Performed standing (according to S Das).
- If no swelling is visible: place a finger on the superficial inguinal ring; or hold the root of the scrotum between index finger and thumb and feel for impulse.
Absent cough impulse occurs in:
- Strangulated hernia
- Incarcerated (irreducible) hernia
- When the neck of the sac is blocked by adhesions
- Femoral hernia with tight neck (leads to misdiagnosis as a lymph node)
"A swelling with a cough impulse is not necessarily a hernia. A swelling with no cough impulse may still be a hernia but consider other diagnoses." - Bailey and Love's
Test 2 - Reducibility
Assess whether hernia contents can be returned to the abdomen.
- Patient lies down; often an indirect inguinal hernia reduces spontaneously.
- Ask the patient to flex, adduct, and internally rotate the thigh of the affected side (relaxes the inguinal rings and oblique abdominal muscles).
- Apply gentle, even pressure to the fundus of the sac - this is called Taxis.
- Enterocele (bowel): reduces with gurgling; first part is hard, last part slips in easily.
- Omentocele (fat): first part reduces easily, last part resists.
Test 3 - Zieman's Technique (Tri-finger Test)
Used to differentiate the type of hernia (indirect inguinal vs. direct inguinal vs. femoral). Only applicable when there is no obvious swelling or after the hernia is fully reduced.
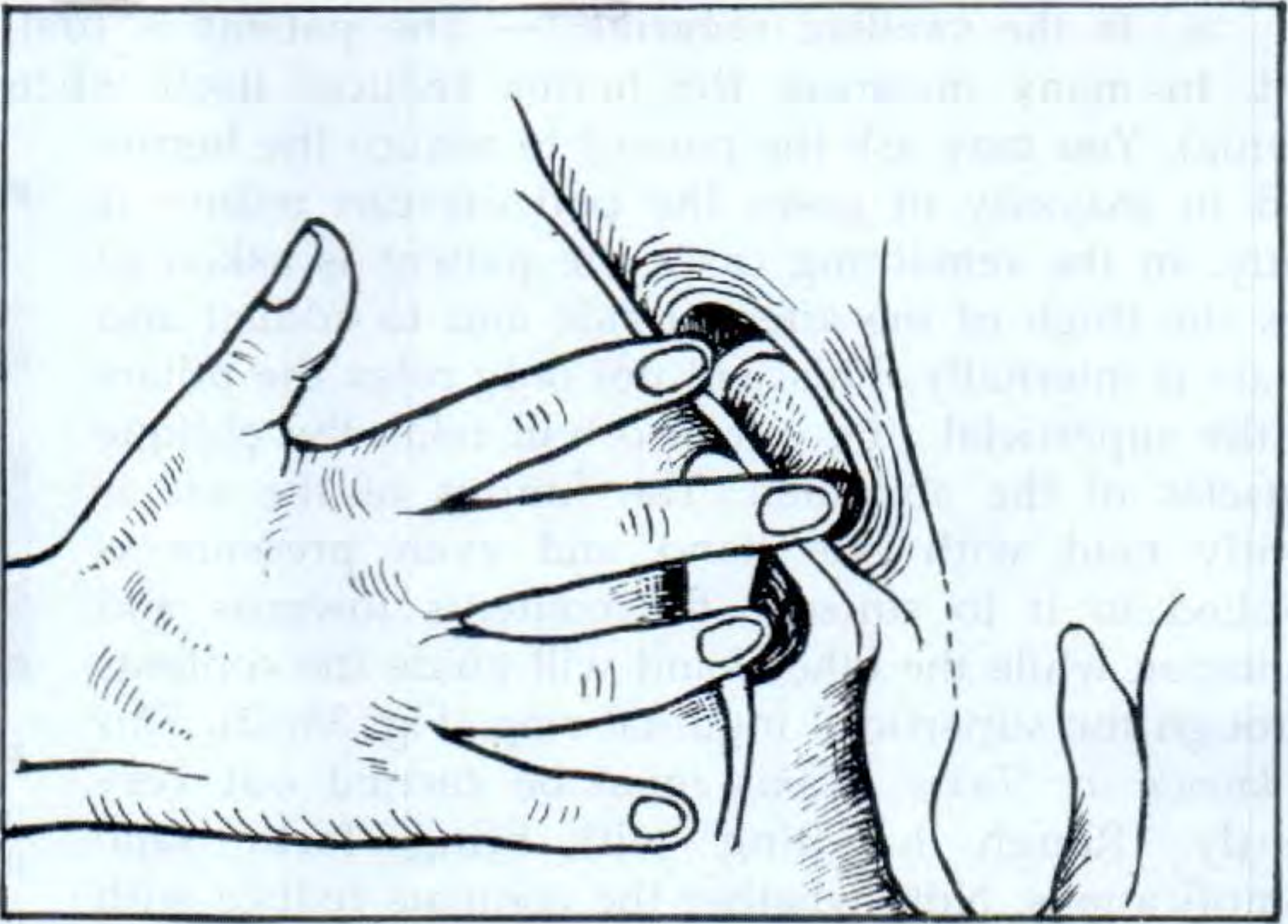
Finger positions (right hand for right groin):
| Finger | Location | Detects |
|---|---|---|
| Index finger | Deep inguinal ring (½ inch above mid-inguinal point - midpoint between ASIS and symphysis pubis) | Indirect (oblique) inguinal hernia |
| Middle finger | Superficial inguinal ring | Direct inguinal hernia |
| Ring finger | Saphenous opening (4 cm below and lateral to pubic tubercle) | Femoral hernia |
Ask the patient to cough (Zieman preferred asking the patient to hold the nose and blow):
-
Impulse on index finger = Indirect hernia
-
Impulse on middle finger = Direct hernia
-
Impulse on ring finger = Femoral hernia
-
S Das - Manual on Clinical Surgery, 13th ed.
Test 4 - Invagination Test (Finger Invagination / Digital Examination of Inguinal Canal)
Technique:
- Hernia is first reduced.
- Invaginate the scrotal skin from the bottom of the scrotum upward along the spermatic cord.
- Introduce the fingertip into the superficial inguinal ring (normal ring admits only the tip of one finger; if >1 finger, ring is dilated).
- Ask the patient to cough.
Interpretation based on direction the finger naturally goes:
| Direction of finger in canal | Type |
|---|---|
| Upwards, backwards, and laterally | Indirect (oblique) hernia |
| Directly backwards | Direct hernia |
On coughing:
- Impulse felt on the tip of the finger = Indirect (oblique) hernia
- Impulse felt on the pulp of the finger = Direct hernia
"When results of physical examination are compared against operative findings, there is a probability somewhat higher than chance (i.e., 50%) of correctly diagnosing the type of hernia." - Schwartz's Principles of Surgery, 11th ed.
Test 5 - Ring Occlusion Test (Deep Inguinal Ring Occlusion Test)
Confirmatory test to differentiate indirect from direct inguinal hernia.
Technique:
- Hernia is fully reduced first.
- Patient stands.
- Examiner places thumb over the deep inguinal ring (½ inch above mid-inguinal point).
- Patient is asked to cough.
Interpretation:
| Finding | Type |
|---|---|
| No bulge appears | Indirect hernia (deep ring is occluded, hernia cannot escape) |
| Bulge appears medial to the occluding finger | Direct hernia (exits through posterior wall, not through deep ring) |
- Similarly, for femoral hernia - pressure over the femoral canal prevents the hernia from coming out.
- S Das - Manual on Clinical Surgery, 13th ed.; Schwartz's Principles of Surgery, 11th ed.
Test 6 - Reducibility Direction (Distinguishing Inguinal from Femoral)
- Inguinal hernia: swelling is above and medial to the pubic tubercle.
- Femoral hernia: swelling is below and lateral to the pubic tubercle (in the upper leg, not lower abdomen).
Summary Table of All Tests
| Test | Position | What is Assessed |
|---|---|---|
| Cough impulse | Standing | Confirms hernia (vs. other swellings) |
| Reducibility / Taxis | Lying | Rules out incarceration/strangulation |
| Zieman's (tri-finger) | Standing, hernia reduced | Type: indirect / direct / femoral |
| Invagination test | Supine, hernia reduced | Type: indirect (tip) vs. direct (pulp); ring size |
| Ring occlusion test | Standing, hernia reduced | Indirect (controlled) vs. direct (escapes medially) |
| Position relative to pubic tubercle | Lying/standing | Inguinal (above & medial) vs. femoral (below & lateral) |
Key clinical pearl: Strangulation is a surgical emergency - suggested by absent cough impulse, overlying skin erythema/cellulitis, and tenderness. Check the contralateral side too, as up to 20% of patients have an occult hernia on the other side.
- Bailey and Love's Short Practice of Surgery, 28th ed.
- S Das - Manual on Clinical Surgery, 13th ed.
- Schwartz's Principles of Surgery, 11th ed.
This is a shared conversation. Sign in to Orris to start your own chat.