Bartholin cyst removal
Reading File
Finding Sources
Finding Sources
Searching PubMed
Bartholin cyst treatment management
Reading File
Reading File
Reading File
Reading File
Reading File
Loading Image
Reading File
Loading Image
I now have comprehensive information from multiple authoritative sources. Here is the complete clinical overview:
Bartholin Cyst/Abscess — Management & Removal
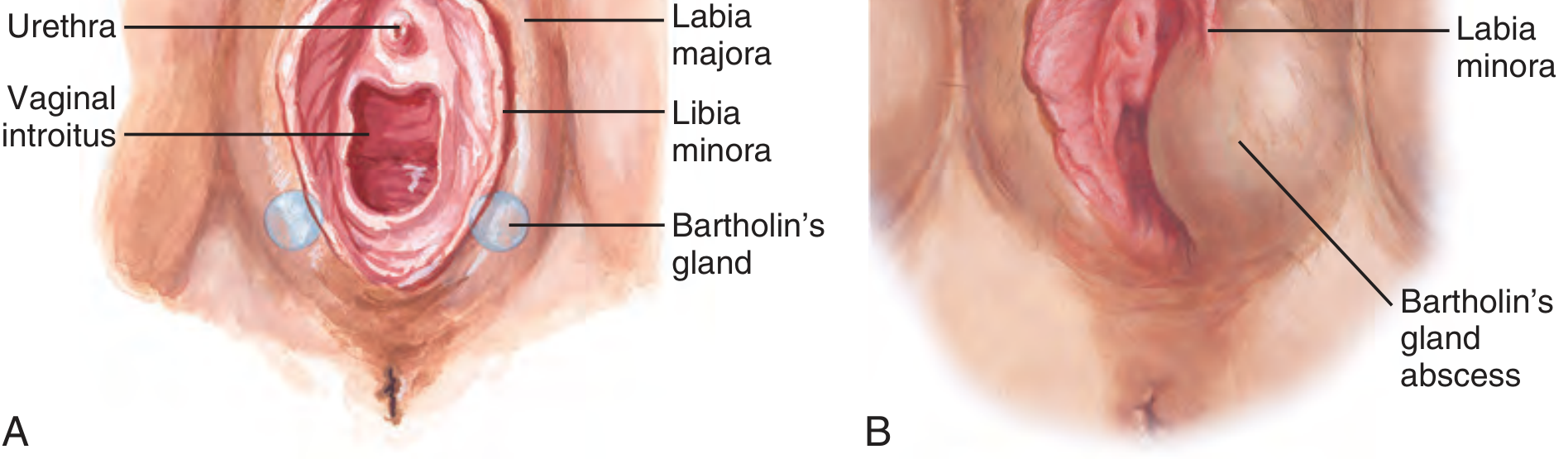
Anatomy
The Bartholin glands are paired mucus-secreting glands located at the 5 and 7 o'clock positions of the posterior vaginal introitus. Duct obstruction causes mucus accumulation (cyst), and superimposed infection produces an abscess.
When to Treat
| Scenario | Management |
|---|---|
| Small, asymptomatic cyst | No treatment needed |
| Symptomatic cyst (painful, growing) | Word catheter or marsupialization |
| Abscess | Drainage (Word catheter or I&D ± marsupialization) |
| Age >40 with solid mass or suspicious epithelium | Excision + biopsy to exclude carcinoma |
Treatment Options
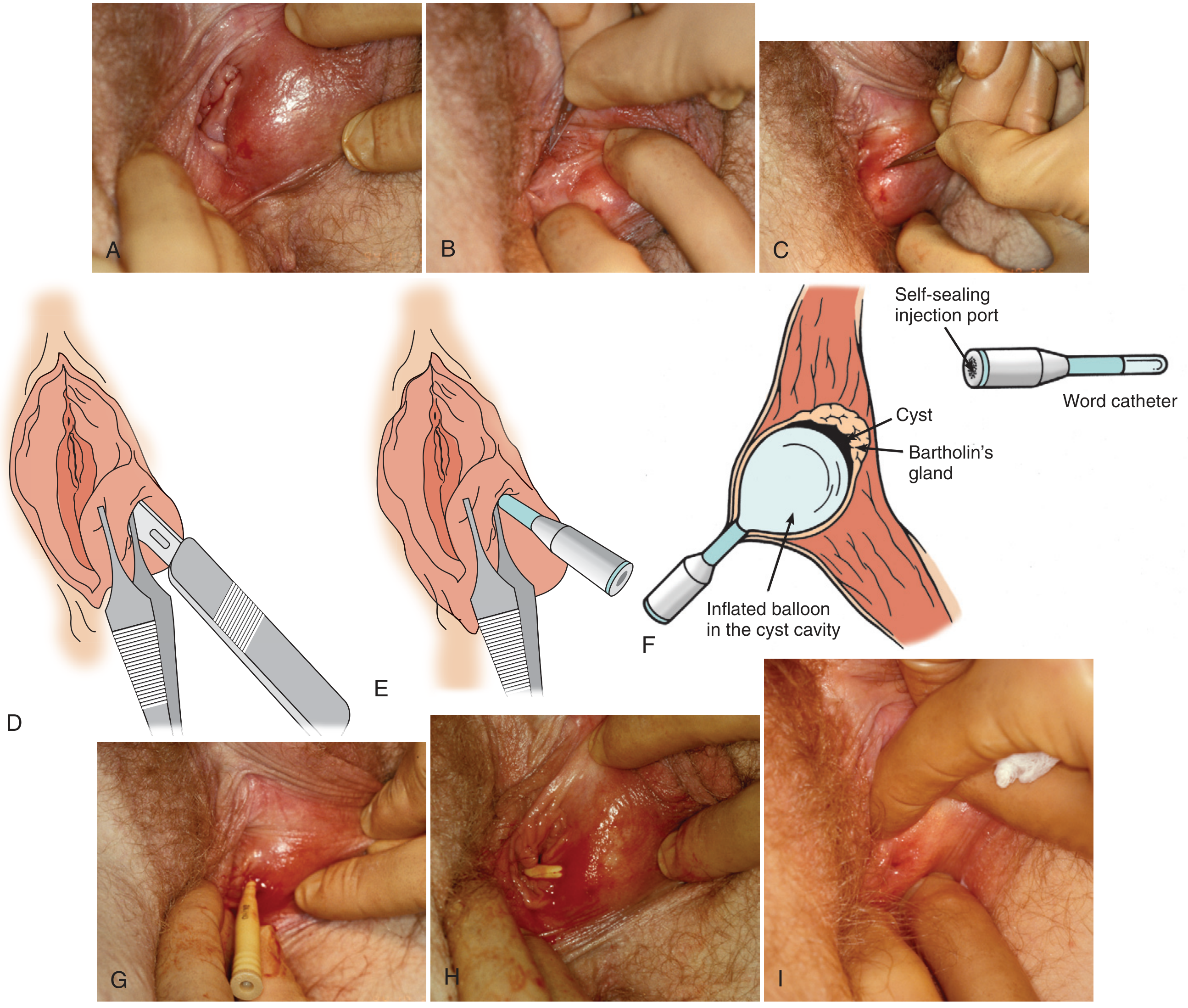
1. Word Catheter Placement (First-line for abscess/symptomatic cyst)
The Word catheter is a small inflatable balloon-tipped catheter that maintains a drainage tract, allowing epithelialization of a permanent gland opening over 4–6 weeks.
Equipment: No. 11 blade, Word catheter, 3 mL syringe + 22-gauge needle (for inflation), 2% lidocaine with epinephrine, pickups with teeth, povidone-iodine.
Step-by-Step Procedure:
- Position: Dorsal lithotomy.
- Prep: Clean with povidone-iodine. Infiltrate over the most prominent point of the cyst/abscess with lidocaine — preferably on the mucosal (vaginal) surface, not the skin, just inside the hymenal ring.
- Incise: Use a No. 11 blade to make a 3–4 mm stab incision through the mucosal surface. Penetration is confirmed by free flow of pus or mucus. Culture if indicated (abscesses are often polymicrobial; Neisseria gonorrhoeae is common).
- Avoid false tract: Before removing the blade, slide Adson forceps with teeth alongside it into the lumen to grasp the tissue — this stabilizes the cavity opening and guides catheter insertion. Remove the blade but keep forceps in place.
- Insert catheter: Pass the Word catheter along the forceps into the cavity. Remove forceps.
- Inflate: Inject 2.5–3 mL saline (not air) through the self-sealing injection port to inflate the balloon. Gently tug to confirm it won't fall out.
- Tuck: If the incision is intravaginal, tuck the catheter stem into the vagina for patient comfort.
- Duration: Leave in place 4–6 weeks, then deflate and remove, leaving a small permanent ostium.
Note: Antibiotics are of no proven benefit once drainage is performed, though practice varies.
2. Marsupialization (Preferred for recurrent cysts; reduces recurrence)
Marsupialization surgically converts the cyst into an open pouch permanently sutured to the vaginal mucosa.
Anesthesia: 2% lidocaine with epinephrine (local block) or pudendal block. Spinal/general anesthesia is an option in a same-day surgery setting.
Step-by-Step:
- Retract the labium laterally and identify the incision site inside the hymenal ring.
- Make a longitudinal fusiform incision 1–2 cm wide through the vaginal mucosa over the cyst wall (not the external skin).
- Before removing the ellipse, grasp the cyst wall with two small hemostats (to prevent collapse). Remove any loculations.
- Biopsy: In patients >40 years, inspect for suspicious epithelium — send for pathology to exclude Bartholin gland carcinoma.
- Irrigate cavity with normal saline.
- Suture the cut edge of the cyst wall to the vaginal mucosa using interrupted 4-0 Vicryl, effectively everting the cyst open. The intent is to keep at least 1 cm gap across the marsupialization.
- No dressing required; apply a pad for drainage.
- Postoperative care: Sitz baths starting the following day.
3. Simple I&D (Emergency setting — highest recurrence rate)
- 5 mm stab incision through the mucosal surface (not skin) at the point of maximal fluctuance.
- Drain contents; may insert a wick or Word catheter.
- High recurrence; gynecology follow-up recommended for definitive marsupialization.
4. Excision of the Bartholin Gland (Reserved for specific indications)
- CPT 56740
- Indicated for: recurrent cysts/abscesses unresponsive to other treatment; age >40 with suspected malignancy.
- More technically demanding; risk of bleeding and hematoma is higher.
- Complete gland removal eliminates recurrence but is not routine.
Key Points
- Location: Always incise on the mucosal surface (vaginal side), not external skin — reduces scarring and improves cosmesis.
- Age >40: Any Bartholin cyst/abscess requires a biopsy to rule out Bartholin gland carcinoma (a rare but important diagnosis).
- Microbiology: Abscesses are commonly polymicrobial; N. gonorrhoeae, E. coli, anaerobes.
- Recurrence: Simple I&D > Word catheter > marsupialization (lowest recurrence).
- Antibiotics: Not routinely indicated after adequate drainage in immunocompetent patients.
Sources: Pfenninger & Fowler's Procedures for Primary Care (3rd ed.); Roberts & Hedges' Clinical Procedures in Emergency Medicine; Berek & Novak's Gynecology; Sabiston Textbook of Surgery
This is a shared conversation. Sign in to Orris to start your own chat.