Give me hypernatermia
Reading File
Finding Sources
Finding Sources
Searching PubMed
hypernatremia management treatment
Reading File
Reading File
Reading File
Reading File
Reading File
Reading File
Reading File
Reading File
Loading Image
Loading Image
I now have all the information needed for a comprehensive answer. Let me compile it.
Hypernatremia
Definition
Hypernatremia is defined as a serum sodium concentration > 145 mEq/L. It is almost always a disorder of water deficit (not sodium excess), and it reflects a state of hyperosmolality - the body's water is insufficient relative to its sodium content.
- Moderate hypernatremia: 146-159 mEq/L (fairly well tolerated)
- Severe hypernatremia: > 160 mEq/L (associated with significant morbidity/mortality)
- Hospital-acquired hypernatremia with Na+ > 150 mEq/L carries a severity-adjusted relative risk of death of 2.6
Pathophysiology
Serum sodium is the primary determinant of extracellular osmolality. When Na+ rises, water shifts out of cells by osmosis, causing cellular dehydration. The brain is particularly vulnerable - brain shrinkage causes traction on bridging veins, which can lead to subarachnoid hemorrhage and cerebral vein rupture.
Compensatory mechanisms:
- Thirst stimulus (most powerful defense)
- ADH (vasopressin) release - concentrates urine
- Brain generates idiogenic osmoles (organic osmolytes) within hours to pull water back in - this is why rapid correction causes cerebral edema
Beyond CNS effects, hypernatremia also:
- Inhibits insulin release and increases insulin resistance → hyperglycemia
- Decreases hepatic gluconeogenesis and lactate clearance
- Impairs cardiac function
Classification and Causes
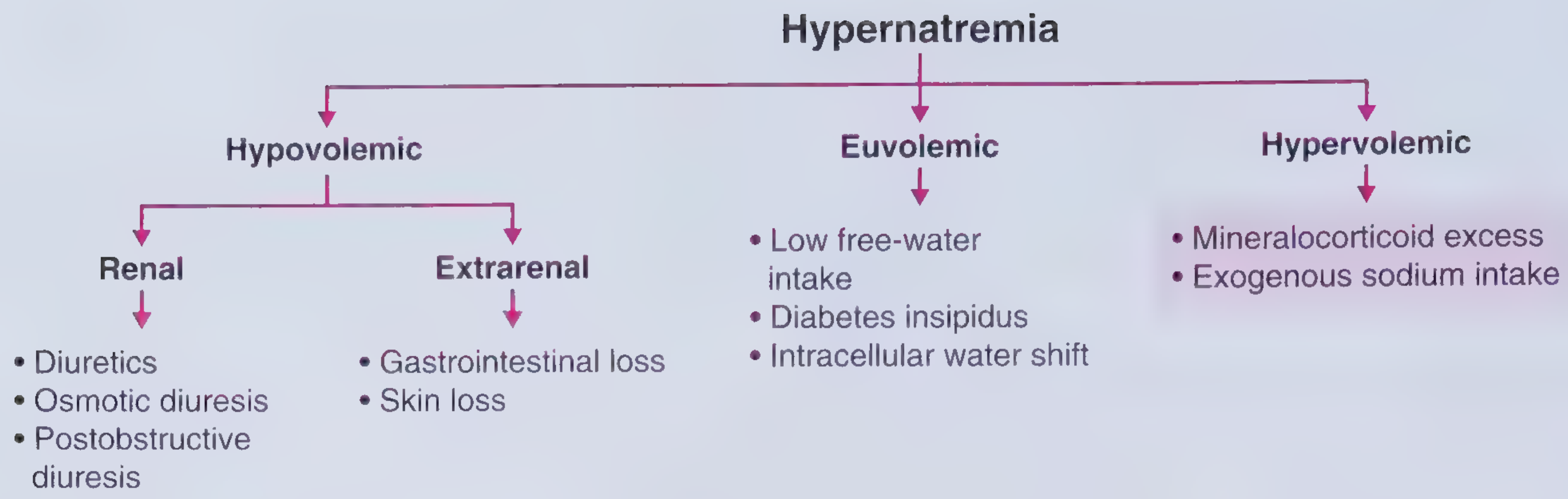
1. Hypovolemic Hypernatremia (water loss > sodium loss)
Renal causes:
- Diuretics (loop > thiazide)
- Osmotic diuresis (glucose, mannitol, enteral feeds)
- Post-obstructive diuresis
Extrarenal causes:
- GI losses: diarrhea, protracted vomiting, continuous GI suction
- Skin losses: burns, excessive sweating, heatstroke
- Increased insensible losses
2. Euvolemic Hypernatremia (pure water deficit, normal sodium stores)
- Diabetes Insipidus (DI) - most important cause
- Central DI: insufficient vasopressin secretion (head trauma, neurosurgery, sarcoidosis, malignancy, autoimmune, idiopathic)
- Nephrogenic DI: vasopressin resistance (lithium, hypercalcemia, hypokalemia, chronic renal insufficiency, sickle cell disease, polycystic kidney disease)
- Low free water intake (elderly, delirium, intubation, dementia)
- Intracellular water shift (intensive exercise, seizures from ECT)
- Hypothalamic dysfunction / reset osmostat
3. Hypervolemic Hypernatremia (gain of hypertonic fluid)
- Salt tablet or seawater ingestion
- Hypertonic saline infusions / hypertonic sodium bicarbonate
- Hypertonic saline enemas
- Poorly diluted enteral feeds
- Primary hyperaldosteronism (Conn's syndrome) - concurrent hypertension + hypokalemia
- Cushing's syndrome
- Hemodialysis with incorrect dialysate
At-Risk Populations
Hypernatremia almost exclusively develops in patients who cannot access or perceive the need for water:
- Elderly (impaired thirst sensation, "reset osmostat")
- Infants
- Patients with altered mental status / delirium
- Intubated / paralyzed patients
- Patients with dementia
Clinical Features
Symptoms (severity correlates with rate of onset, not just absolute level)
- Mild: Thirst, restlessness, irritability, muscle weakness
- Moderate: Lethargy, insomnia, confusion
- Severe: Depressed sensorium, stupor, coma, seizures, focal neurological deficits
- Rapid-onset hypernatremia is more dangerous than chronic (less time for idiogenic osmole compensation)
Signs
| Finding | Sensitivity | Specificity | LR+ |
|---|---|---|---|
| Tachycardia | 17.8% | 94% | 2.97 |
| Orthostatic hypotension | 61.5% | 50.6% | 1.24 |
| Abnormal subclavicular skin turgor | 73.3% | 79% | 3.49 |
| Dry oral mucosa | 49% | 87.8% | 4.02 |
Note: No single finding is highly sensitive - hypernatremia-induced brain shrinkage can also cause subarachnoid hemorrhage.
Diagnostic Workup
Initial labs:
- Serum electrolytes, BUN, creatinine, glucose
- Serum osmolality
- Urine sodium + urine osmolality
Urine osmolality is the key branch point:
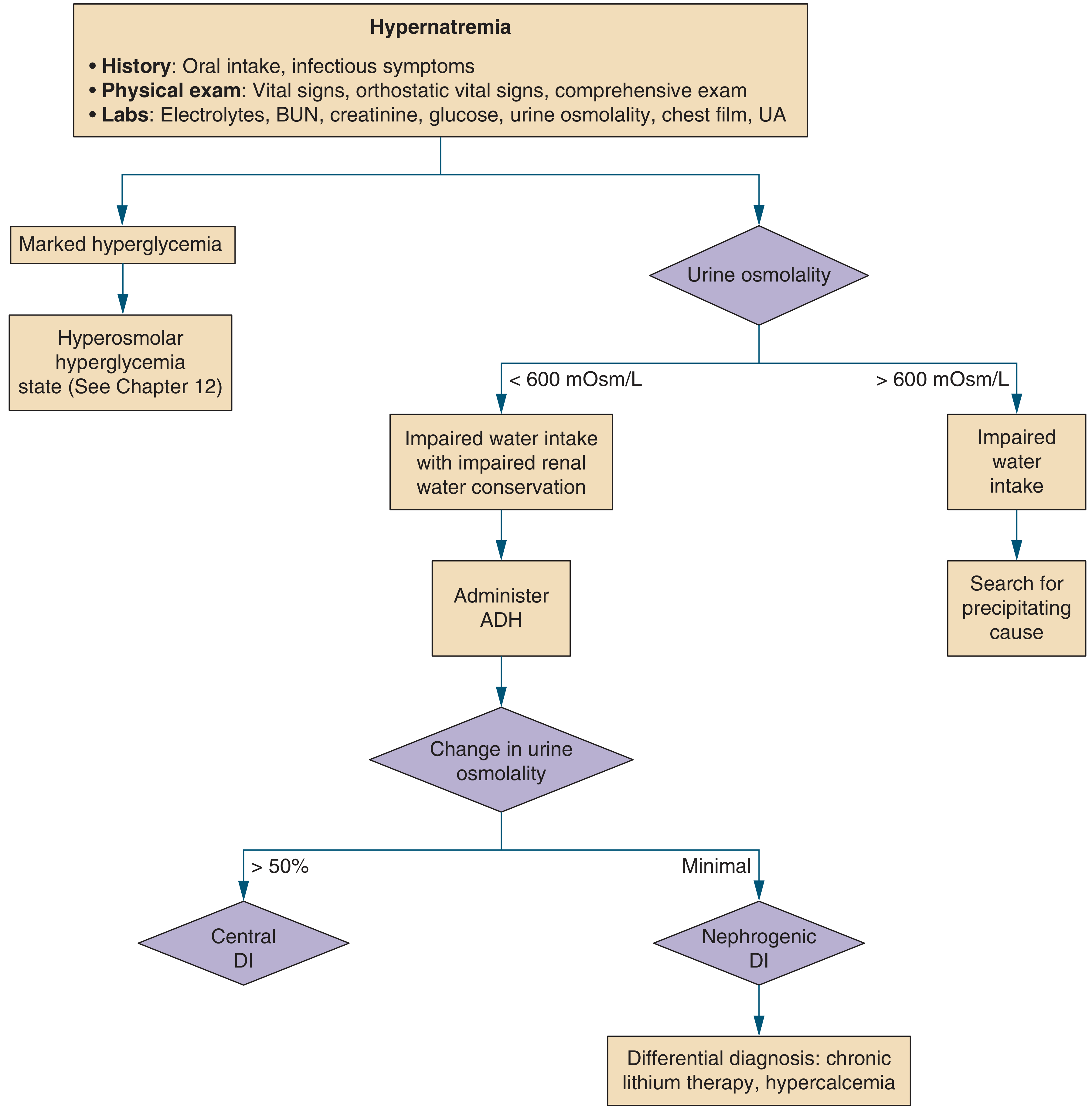
- Urine osmolality > 600 mOsm/kg → kidneys concentrating maximally → impaired water intake is the cause → look for precipitating factor
- Urine osmolality < 600 mOsm/kg → impaired water intake + impaired renal water conservation → administer ADH (desmopressin):
- Urine osmolality increases > 50% → Central DI
- Minimal response → Nephrogenic DI (consider lithium, hypercalcemia)
Free Water Deficit Calculation
TBW deficit (liters) = TBW × [(serum Na+ - 140) / 140]
Where TBW = body weight (kg) × correction factor:
| Population | TBW factor |
|---|---|
| Children & adult men | × 0.6 |
| Adult women | × 0.5 |
| Elderly men | × 0.5 |
| Elderly women | × 0.45 |
Example: 70 kg adult man with Na+ = 160: TBW deficit = (70 × 0.6) × (160-140)/140 = 42 × 0.143 = 6 liters
Management
Three Goals (in order):
- Correct hemodynamic instability first - isotonic normal saline (0.9% NaCl) until hemodynamically stable. Do not chase the sodium until volume is restored - homeostatic Na+ retention mechanisms will prevent progress.
- Treat the underlying cause - fever, vomiting, DI, etc.
- Replace free water deficit slowly
Rate of Correction
- Acute hypernatremia (developed over hours, e.g., salt loading): rapid correction at ≥ 1 mEq/L/hr is relatively safe
- Chronic hypernatremia (developed over days-weeks, the usual case): correct at no more than 0.5 mEq/L/hr or 10-12 mEq/day - brain has generated idiogenic osmoles; rapid correction causes cerebral edema
Failure to consider ongoing sensible and insensible losses is the most common cause of undercorrection.
Fluid Choice
| Situation | Fluid |
|---|---|
| Hypovolemia / shock | Normal saline (0.9% NaCl) first |
| After hemodynamic stability | Switch to 0.45% NaCl (half-normal saline) at ~100 mL/hr |
| Pure water deficit (no hemodynamic compromise) | 5% Dextrose in water (D5W) |
| Oral route available | Free oral water intake |
Diabetes Insipidus - Specific Treatment
- Central DI: Desmopressin (DDAVP) 1-2 µg IV/SC in the acute setting - effective for both polyuria and hypernatremia
- Nephrogenic DI: Remove causative drug (lithium), treat hypercalcemia/hypokalemia; low-sodium diet + thiazide diuretics (paradoxically reduce urine output)
Monitoring
- Recheck serum Na+ every 4-6 hours during active correction
- Patients whose hypernatremia is corrected within 72 hours have lower mortality than those corrected beyond 72 hours
- Fewer than 50% of hospital-acquired hypernatremia patients receive free water replacement within 24 hours of identification - this is a recognized gap in care
Disposition
- Most require hospitalization (dehydration + underlying comorbidities)
- Mild cases with intact thirst and no underlying cause may be managed with increased oral water at home
Key Points Summary
| Feature | Detail |
|---|---|
| Definition | Na+ > 145 mEq/L |
| Core mechanism | Free water deficit relative to sodium |
| Most common cause | Inadequate water intake (elderly, encephalopathic, intubated) |
| Key DI differentiator | Desmopressin test (urine osmolality response) |
| Correction rate (chronic) | ≤ 0.5 mEq/L/hr, max 10-12 mEq/day |
| Correction rate (acute) | Can be faster, ~1 mEq/L/hr |
| First fluid in shock | NS (0.9% NaCl) |
| First fluid in pure water deficit | D5W or oral water |
| Mortality marker | Level of consciousness > absolute Na+ value |
| Severity-adjusted mortality risk | RR 2.6 when Na+ > 150 mEq/L |
Sources: Rosen's Emergency Medicine 10e; Frameworks for Internal Medicine; Symptom to Diagnosis 4e; NKF Primer on Kidney Diseases 8e; Comprehensive Clinical Nephrology 7e
From surgery point of view explain haemorrhage types management and blood transfusion indications complications various blood products and appropriate indications basics concepts of hemoststis and mechanism of hemostasis
Reading File
Finding Sources
Finding Sources
Finding Sources
Finding Sources
Finding Sources
Finding Sources
Finding Sources
Reading File
Reading File
Reading File
Reading File
Reading File
Reading File
Reading File
Finding Sources
Finding Sources
Reading File
Reading File
Reading File
Reading File
Reading File
Reading File
Finding Sources
Reading File
Reading File
Reading File
Haemorrhage, Haemostasis, Blood Products & Transfusion - A Surgical Overview
PART 1: MECHANISM OF HAEMOSTASIS
Haemostasis is a precisely orchestrated process involving endothelium, platelets, and clotting factors that forms a blood clot at the site of vascular injury to prevent or limit bleeding. It proceeds in four sequential steps:
Step 1 - Arteriolar Vasoconstriction
Immediately after vascular injury, neurogenic reflexes and endothelium-derived endothelin cause transient vasoconstriction, reducing blood flow. This is temporary - without platelet and coagulation activation, bleeding resumes.
Step 2 - Primary Haemostasis (Platelet Plug Formation)
- Vascular injury exposes subendothelial collagen and von Willebrand Factor (vWF)
- Platelets adhere via GpIb receptors binding to vWF
- Adhesion triggers platelet activation - shape change from discs to spiky plates, release of granule contents (ADP, thromboxane A2)
- ADP and TXA2 recruit additional platelets
- Fibrinogen bridges platelets via GpIIb-IIIa receptors → platelet aggregation
- Result: the primary haemostatic plug (fast but fragile)
Step 3 - Secondary Haemostasis (Coagulation Cascade)
Vascular injury exposes Tissue Factor (TF) on subendothelial smooth muscle cells and fibroblasts. TF binds and activates Factor VII → initiating the coagulation cascade.
Key factors in vivo: VII, IX, X, II (prothrombin), fibrinogen, plus cofactors V and VIII.
End result: Thrombin (IIa) converts fibrinogen → fibrin meshwork, cementing the platelet plug into the secondary haemostatic plug. Thrombin also amplifies platelet activation.
Step 4 - Clot Stabilisation and Counter-Regulation
- Factor XIII (activated by thrombin) covalently crosslinks fibrin strands
- Platelet contraction compacts and strengthens the clot
- Excessive clotting is limited by:
- Washout and hepatic clearance of activated factors
- Requirement for phospholipid surfaces (only on activated platelets)
- Endothelial anticoagulants: thrombomodulin, protein C, TFPI
- Fibrinolysis via tissue plasminogen activator (tPA) → plasmin → fibrin degradation
Key summary: Primary haemostasis = platelet plug (GpIb-vWF adhesion + GpIIb-IIIa aggregation). Secondary haemostasis = fibrin mesh (TF-VII → cascade → thrombin → fibrin). Factor XIII stabilises.
PART 2: HAEMORRHAGE - TYPES AND CLASSIFICATION
A. Classification by Vessel Type
| Type | Source | Characteristics |
|---|---|---|
| Arterial | Artery | Bright red, pulsatile, spurting; BP drops early (before tissue ischaemia); can stop temporarily via spasm/thrombosis; lacerated artery bleeds more than transected |
| Venous | Vein | Dark red, steady flow; slower progression allows compensation; large volumes lost before hypotension; lactate/base deficit elevated early |
| Capillary | Capillary bed | Oozing, bright red; minor in isolation; significant in congested/inflamed tissue |
B. Classification by Timing (Surgical)
| Type | Timing | Cause |
|---|---|---|
| Primary | At time of injury | Direct vessel damage |
| Reactionary | Within 24 hours (usually 4-6 h) | Clot displacement as BP rises, ligature slippage |
| Secondary | 7-14 days post-op | Infection eroding vessel wall |
C. Classification by Cause
- Traumatic - direct injury
- Operative/Iatrogenic - surgical bleeding
- Spontaneous - coagulopathy, aneurysm rupture, erosion by tumour or infection
D. Classification by Location
| Term | Location |
|---|---|
| Haematoma | Within tissue |
| Haemothorax | Pleural cavity |
| Haemopericardium | Pericardium |
| Haemoperitoneum | Peritoneal cavity |
| Haemarthrosis | Joint |
| Petechiae | 1-2 mm skin/mucosa (thrombocytopenia) |
| Purpura | 3-5 mm (vasculitis, platelet dysfunction) |
| Ecchymosis | >1 cm - subcutaneous haematoma |
PART 3: ATLS HAEMORRHAGIC SHOCK CLASSIFICATION
(American College of Surgeons - ATLS, 2018)
| Parameter | Class I | Class II (Mild) | Class III (Moderate) | Class IV (Severe) |
|---|---|---|---|---|
| Blood loss (%) | < 15% | 15-30% | 31-40% | > 40% |
| Blood loss (mL, 70 kg) | < 750 | 750-1500 | 1500-2000 | > 2000 |
| Heart rate | Normal | Normal/↑ | ↑ | ↑↑ |
| Blood pressure | Normal | Normal | Normal/↓ | ↓ |
| Pulse pressure | Normal | ↓ | ↓ | ↓ |
| Respiratory rate | Normal | Normal | Normal/↑ | ↑ |
| Urine output | Normal | Normal | ↓ | ↓↓ |
| GCS | Normal | Normal | ↓ | ↓ |
| Base deficit | 0 to -2 | -2 to -6 | -6 to -10 | < -10 |
| Blood products | Monitor | Possible | Yes | Massive transfusion protocol |
Important: BP does not theoretically fall until Class III (>30% blood loss = ~2 L, equivalent to a "six-pack of soda"). BP alone is not a reliable early indicator. The Shock Index (SI) = HR/SBP is a better marker; SI > 0.9 is highly suggestive of critical bleeding.
Relative bradycardia (HR < 100 with SBP < 90) paradoxically carries lower mortality - this vagally-mediated response reduces cardiac output and slows exsanguination. Patients with HR 60-90 bpm have the best survival.
PART 4: MANAGEMENT OF HAEMORRHAGE
Principles: The "Double-Armed" Approach
Resuscitation and haemorrhage control must occur simultaneously - resuscitation is an adjunct to, not a substitute for, haemorrhage control. Aggressive resuscitation without haemorrhage control worsens outcomes ("pops the clot").
Step-by-Step Management
1. Initial Assessment and Access
- Two large-bore IV lines; send blood for type and crossmatch
- If IV access fails - intraosseous or large-bore central venous access
2. Haemorrhage Control (Simultaneous)
- Direct pressure / tourniquet for extremity bleeding
- Haemostatic dressings for junctional wounds
- Damage control surgery / angioembolisation for internal bleeding
3. Permissive Hypotension
- Target SBP 70-90 mmHg (or palpable radial pulse) until definitive haemorrhage control
- Controlled resuscitation with 250 mL boluses - reduces mortality vs. aggressive 2 L boluses
- Exception: Traumatic brain injury - maintain adequate cerebral perfusion pressure (higher targets)
4. Initial Fluid
- Class I-II: 1 L warmed isotonic crystalloid and observe response
- Sustained response = bleeding stopped
- Transient/no response = ongoing haemorrhage, switch to blood products
- Class III-IV: direct to blood products and massive transfusion protocol
5. Damage Control Resuscitation (for active haemorrhagic shock)
| Principle | Detail |
|---|---|
| Minimise crystalloid | Prevents haemodilution, hypothermia, coagulopathy |
| Balanced blood products | PRBCs : FFP : Platelets in 1:1:1 ratio |
| Tranexamic acid (TXA) | Given ASAP, within 3 hours of injury; reduces mortality |
| Treat coagulopathy actively | Don't wait for labs in massively bleeding patient |
| Correct hypothermia | Rewarming; use warmed blood products |
6. Emergency Blood
- Type-specific, non-crossmatched blood can be used in emergencies
- Type O-negative for pregnant females and females of childbearing age
- Type O-positive acceptable in males/post-menopausal females when O-neg unavailable
Damage Control Resuscitation Box (ATLS Principles)
- Direct pressure / tourniquet / haemostatic packing
- Early transfer to OR or angiography suite
- Minimise crystalloid (max 1 L before blood)
- Balanced blood products 1:1:1
- TXA within 3 hours
- Permissive hypotension (SBP 70-90) until haemorrhage control
- Treat hypothermia, acidosis, and coagulopathy - the "lethal triad"
PART 5: BLOOD PRODUCTS AND THEIR INDICATIONS
1. Whole Blood
- Rarely available in civilian practice
- Significant advantage: coagulation factor-rich, metabolically active if fresh
- Military studies show improved mortality and decreased component use
- Some level I trauma centres reintroducing in trauma resuscitation
2. Packed Red Blood Cells (PRBCs)
- ~330 mL/unit; haematocrit 50-70%
- Stored in SAG-M (saline-adenine-glucose-mannitol) at 2-6°C; shelf life 5 weeks
- Indications:
- Acute blood loss to replace circulating volume
- Perioperative anaemia to ensure oxygen delivery
- Symptomatic chronic anaemia
Transfusion Trigger (Hb-based):
| Hb (g/dL) | Clinical Decision |
|---|---|
| < 6 | Probably will benefit from transfusion |
| 6-8 | Transfusion unlikely to benefit (absent bleeding or surgery) |
| > 8 | No indication in absence of other risk factors |
Historical target of Hb > 10 g/dL is now shown to increase morbidity and mortality vs. lower targets.
3. Fresh Frozen Plasma (FFP)
- Removed from fresh blood; stored at -40 to -50°C; shelf life 2 years
- Contains all coagulation factors
- Indications:
- Coagulopathic haemorrhage (first-line)
- Massive transfusion (as part of 1:1:1 ratio)
- Reversal of warfarin in urgent bleeding
- DIC with active bleeding
- Note: Rh-D negative women receiving Rh-D positive FFP should receive Rh-D immunoglobulin (small risk of sensitisation from red cell fragments)
4. Cryoprecipitate
- Cold-precipitated supernatant of FFP; stored at -30°C; shelf life 2 years
- Rich in: Fibrinogen, Factor VIII, Factor XIII, vWF
- Indications:
- Hypofibrinogenaemia (most common surgical indication)
- Factor VIII deficiency (haemophilia A, when FVIII concentrate unavailable)
- vWD Type 1-2
- DIC with low fibrinogen
- Often guided by thromboelastometry (TEG/ROTEM)
5. Platelets
- Pooled concentrate (~250 × 10⁹/L); stored at 20-24°C with agitation; shelf life only 5 days
- Indications:
- Thrombocytopenia with active bleeding or pre-surgery
- Platelet dysfunction (e.g., clopidogrel, aspirin) with active surgical bleeding
- Patients on clopidogrel may need near-continuous platelet infusion during major surgery
- DDAVP (desmopressin) can also improve platelet function in some settings
6. Prothrombin Complex Concentrates (PCCs)
- Highly purified pooled plasma concentrates
- Contain Factors II, IX, X (3-factor PCC) or also Factor VII (4-factor PCC)
- Indications:
- Urgent reversal of vitamin K antagonists (warfarin)
- Massive haemorrhage when FFP unavailable or time-critical
- Haemophilia B (Factor IX deficiency)
7. Tranexamic Acid (TXA)
- Anti-fibrinolytic agent (lysine analogue - inhibits plasminogen activation)
- Surgical indication: Most bleeding trauma patients are hyperfibrinolytic; TXA should be given empirically as early as possible, within 3 hours of injury
- CRASH-2 trial: significant reduction in death from haemorrhage
- Also used in elective surgery to reduce perioperative blood loss
PART 6: MASSIVE TRANSFUSION
Definition: Transfusion of ≥ 10 units PRBCs within 24 hours (or ≥ 4 units in 1 hour).
Massive Transfusion Protocol (MTP) Ratio
- 1:1:1 - PRBCs : FFP : Platelets (one apheresis unit or "six-pack")
- Supported by the PROPPR randomised trial (Holcomb et al.)
- 1:1:1 vs 1:1:2 showed no mortality difference at 24h/30d but better haemostatic laboratory profile with 1:1:1
- Higher plasma/platelet ratios in early resuscitation associated with decreased mortality (PROMMTT study)
Complications of Massive Transfusion
| Complication | Mechanism |
|---|---|
| Coagulopathy (dilutional) | Loss of clotting factors with PRBC-heavy transfusion |
| Hypocalcaemia | Citrate in preservative chelates ionised calcium |
| Hyperkalaemia | Stored blood leaks potassium during storage |
| Hypokalaemia | Citrate metabolised to bicarbonate → alkalosis → K+ shifts intracellularly |
| Hypothermia | Cold stored blood without active warming |
| Iron overload | Each unit contains ~250 mg elemental iron; significant in chronic transfusion patients |
PART 7: TRANSFUSION REACTIONS AND COMPLICATIONS
Immediate Reactions
| Reaction | Signs & Symptoms | Management |
|---|---|---|
| Acute Intravascular Haemolytic (most dangerous - ABO incompatibility) | Fever, chills, low back pain, flushing, dyspnoea, tachycardia, shock, haemoglobinuria, DIC | Stop transfusion immediately. IV hydration for diuresis (maintain urine output). Cardiorespiratory support. Retype + crossmatch. Direct/indirect Coombs test. CBC, PT/aPTT, haptoglobin, LDH, bilirubin, plasma free Hb |
| Febrile Non-Haemolytic (FNHTR) | Fever, chills | Stop transfusion; initially manage as haemolytic until ruled out. Treat with paracetamol. Usually mild. |
| Allergic (mild) | Urticaria, pruritus | Stop transfusion; diphenhydramine; if symptoms resolve, may restart |
| Anaphylaxis (severe allergic) | Dyspnoea, bronchospasm, hypotension, shock | Stop transfusion immediately. Adrenaline, cardiopulmonary support. Do not restart. |
Delayed Reactions
| Reaction | Features |
|---|---|
| Delayed Haemolytic | Days-weeks post-transfusion; low-grade fever; often asymptomatic; antibodies against minor RBC antigens |
| TRALI (Transfusion-Related Acute Lung Injury) | 6-72 hours post; noncardiogenic pulmonary oedema (ARDS-like); anti-leucocyte antibodies in donor product; self-limiting; avoid diuresis (noncardiogenic - will worsen); supportive care; more common after plasma |
| TACO (Transfusion-Associated Circulatory Overload) | Dyspnoea, hypoxia, pulmonary oedema (cardiogenic); in elderly and cardiac patients; treat with diuretics; slow transfusion rate |
| Graft-versus-Host Disease | Rare; in immunocompromised patients; irradiated blood products reduce risk |
Infectious Complications
| Pathogen | Risk per Unit Transfused |
|---|---|
| HIV-1 | 1 in 6 million |
| Hepatitis C | 1 in 100 million |
| Hepatitis B | 1 in 1 million |
| HTLV-1/2 | 1 in 640,000 |
| Parvovirus B19 | 1 in 10,000 |
| Bacteria (especially platelets) | Relatively higher in platelets (stored at room temperature) |
In the UK, all donations are leukodepleted (reduces immunogenicity and vCJD risk). All units tested for HIV-1/2, Hep B, Hep C, syphilis. ABO and Rh-D typed with screen for irregular antibodies.
First step in any suspected transfusion reaction:
- Stop the transfusion
- Notify the blood bank
- Retype and crossmatch a new sample - so transfusion can resume safely as quickly as possible
Do not abandon all future transfusion after a reaction - reactions are usually unit-specific and patient-specific. Appropriately matched future units can be transfused safely.
Premedication
- Routine premedication (paracetamol/diphenhydramine) is NOT recommended for all patients
- Reserved for patients with prior febrile or allergic transfusion reactions
PART 8: BLOOD GROUPS AND COMPATIBILITY
ABO System
| Phenotype | Antigens | Antibodies | Frequency |
|---|---|---|---|
| O | O | Anti-A, Anti-B | 46% |
| A | A | Anti-B | 42% |
| B | B | Anti-A | 9% |
| AB | A and B | None | 3% |
- O-negative: universal donor (no A, B, or Rh-D antigens)
- AB: universal recipient
- Rhesus D system: major cause of haemolytic transfusion reactions and haemolytic disease of the newborn
Summary Framework
HAEMORRHAGE
├── By vessel: Arterial / Venous / Capillary
├── By timing: Primary / Reactionary / Secondary
├── By severity (ATLS Class I-IV based on % blood volume lost)
│
HAEMOSTASIS
├── Step 1: Vasoconstriction (endothelin)
├── Step 2: Primary platelet plug (vWF-GpIb → GpIIb-IIIa-fibrinogen)
├── Step 3: Coagulation cascade (TF-VII → thrombin → fibrin)
└── Step 4: Clot stabilisation (FXIIIa crosslinks fibrin) + fibrinolysis
│
MANAGEMENT (haemorrhagic shock)
├── Control bleeding (pressure/tourniquet/surgery/IR)
├── Permissive hypotension (SBP 70-90 until control)
├── Damage control resuscitation: PRBCs:FFP:Platelets = 1:1:1
├── TXA within 3 hours
└── Treat lethal triad: hypothermia + acidosis + coagulopathy
│
BLOOD PRODUCTS
├── PRBCs: O2 carriage; trigger Hb < 6-8 g/dL
├── FFP: all factors; coagulopathy/massive transfusion
├── Cryoprecipitate: fibrinogen + FVIII + FXIII; hypofibrinogenaemia
├── Platelets: thrombocytopenia/platelet dysfunction; 5-day shelf life
└── PCC: Factor II/IX/X; urgent warfarin reversal
│
TRANSFUSION COMPLICATIONS
├── Haemolytic (ABO) → STOP, hydrate, Coombs
├── FNHTR → paracetamol, rule out haemolytic
├── TRALI → supportive, no diuretics
├── TACO → diuretics, slow rate
└── Infectious: extremely rare with modern screening
Sources: Current Surgical Therapy 14e; Bailey and Love's Short Practice of Surgery 28e; Sabiston Textbook of Surgery; Robbins & Kumar Basic Pathology; Tintinalli's Emergency Medicine; Miller's Anesthesia 10e; ATLS Student Course Manual 2018
This is a shared conversation. Sign in to Orris to start your own chat.