Shoulder all special test with procedure interpretation in detail
Reading File
Finding Sources
Finding Sources
Finding Sources
Finding Sources
Reading File
Reading File
Reading File
Finding Sources
Finding Sources
Reading File
Reading File
Reading File
Finding Sources
Finding Sources
Finding Sources
Reading File
Reading File
I now have comprehensive data from multiple authoritative textbooks. Let me compile the full detailed answer:
Shoulder Special Tests: Complete Guide with Procedure & Interpretation
All tests below are sourced from Miller's Review of Orthopaedics 9th Ed, Campbell's Operative Orthopaedics 15th Ed 2026, Bailey & Love's Surgery 28th Ed, and Tintinalli's Emergency Medicine.
I. IMPINGEMENT / ROTATOR CUFF TESTS
1. Neer Impingement Sign
Procedure: The examiner stabilizes the patient's scapula with one hand (prevents scapular rotation), then passively elevates the arm in the plane of forward flexion (FF) beyond 90 degrees with the arm in full internal rotation.
Positive sign: Pain reproduced in the arc between 70-120 degrees of elevation.
Interpretation: Pain indicates subacromial impingement - the greater tuberosity is being compressed against the undersurface of the acromion and coracoacromial ligament.
Accuracy: Sensitivity 68-89%, Specificity 68.7%. Also positive in 46% with SLAP lesions and 69% with AC joint arthritis.
2. Neer Impingement Test (Injection Test)
Procedure: Same maneuver as Neer sign, but performed before and after injecting 10 mL of 1% lidocaine (Xylocaine) into the subacromial space.
Positive: Relief of pain after injection indicates impingement as the source.
Interpretation: Differentiates subacromial impingement from other causes of shoulder pain. Specificity is low for pinpointing exact pathology (positive in 25% of Bankart lesions, 46% of SLAP lesions). - Campbell's Operative Orthopaedics, p. 2812
3. Hawkins-Kennedy Test
Procedure: The examiner passively places the arm in 90 degrees of forward flexion, with the elbow bent to 90 degrees. The shoulder is then forcibly internally rotated, bringing the forearm across the front of the patient.
Positive: Reproduction of pain in the shoulder.
Interpretation: Internal rotation drives the greater tuberosity and anterior rotator cuff underneath the coracoacromial ligament, reproducing impingement pain. Indicates subacromial impingement syndrome or rotator cuff tendinopathy.
Accuracy: Sensitivity 71.5-92%, Specificity 44-66.3%. High sensitivity makes it a good screening test (good negative predictive value 90-93%). - Campbell's Table 51.2; Bailey & Love, p. 509
4. Painful Arc Sign
Procedure: Patient actively abducts the arm from 0 to 180 degrees while the examiner observes for pain.
Positive: Pain occurring specifically in the arc between 60-120 degrees of abduction.
Interpretation: Pain in this arc results from compression of the rotator cuff (particularly supraspinatus) and subacromial bursa under the acromion. If pain occurs at full elevation (~170 degrees), AC joint pathology is more likely.
Accuracy: Sensitivity 73.5%, Specificity 81.1%, PPV 88.2% - among the highest specificity of impingement tests. - Campbell's Table 51.2
5. Jobe Test (Empty Can Test / Supraspinatus Test)
Procedure: The patient abducts the arm to 90 degrees, then forward flexes 30 degrees (in the plane of the scapula). The thumbs point downward ("empty can" position - as if pouring out a can). The examiner applies downward resistance while the patient tries to maintain the position.
Positive: Pain or weakness against resistance.
Interpretation: Isolates the supraspinatus tendon. Pain indicates supraspinatus tendinopathy or impingement; frank weakness suggests a supraspinatus tear.
Accuracy: Sensitivity 44.1%, Specificity 89.5%, PPV 88.4% - high specificity makes it a good confirmatory test. - Miller's Table 4.7; Tintinalli's, p. 280

6. Drop Arm Test
Procedure: The examiner passively places the patient's arm at 90 degrees of abduction in the plane of the scapula, then releases it. The patient is asked to slowly lower the arm to the side.
Positive: Patient unable to maintain the arm elevated or lowers it with a sudden drop.
Interpretation: Inability to maintain forward elevation indicates a significant supraspinatus tear (complete tear). A "drop" after a slight tap on the wrist also constitutes a positive sign.
Accuracy: Sensitivity 26.9%, Specificity 88.4% - low sensitivity but high specificity means a positive test strongly suggests complete rotator cuff tear. - Miller's Table 4.7; Campbell's Table 51.2
7. Infraspinatus Test (External Rotation Lag Sign)
Procedure: Arm at side, elbow flexed 90 degrees, forearm in neutral. The patient resists external rotation against the examiner. Also: resisted maximal ER with 90 degrees abduction (Hornblower sign).
Positive: Weakness or inability to maintain ER; lag on passive ER.
Interpretation: Tests the infraspinatus (and teres minor at full abduction). Weakness indicates infraspinatus tear.
Hornblower (Hornblower's) Sign: Resisted maximal ER at 90 degrees abduction. Positive (inability) indicates infraspinatus, teres minor, or posterior supraspinatus lesion. - Miller's Table 4.7
8. Subscapularis Tests
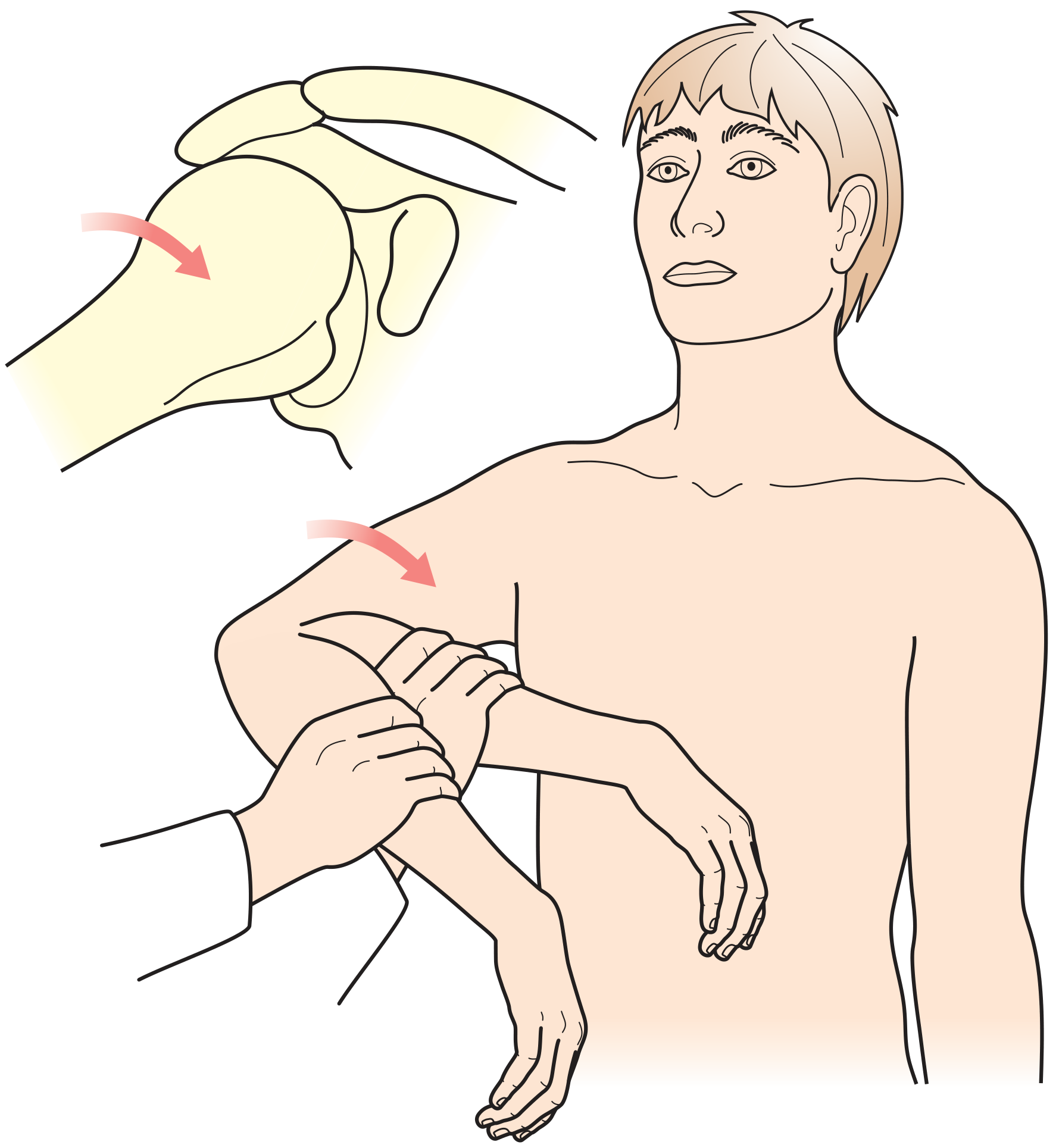
a. Lift-Off Test (Gerber's Lift-Off)
Procedure: Patient places the dorsum of the hand against the lower back (arm in internal rotation behind the back). The patient is asked to push the hand away from the back (lift off).
Positive: Inability to lift the hand away from the back.
Interpretation: Tests the subscapularis muscle. Inability to perform the lift-off indicates a subscapularis tear. - Tintinalli's, p. 280; Miller's Table 4.7
b. Modified Lift-Off Test
Procedure: Examiner lifts the arm off the patient's back to a set position, then releases. Patient attempts to keep the arm in that elevated position.
Positive: Arm falls back onto the back (cannot maintain the position).
c. Belly-Press (Napoleon) Test
Procedure: Patient presses the palm of the hand into the abdomen while keeping the elbow elevated (in line with or anterior to the trunk). The examiner tries to pull the elbow posteriorly.
Positive: Inability to keep the elbow forward; wrist flexes to compensate (elbow drops behind trunk).
Interpretation: Tests subscapularis. Wrist flexion compensation is a hallmark positive finding. - Miller's Table 4.7
d. Bear-Hug Test
Procedure: Patient places the hand (fingers extended) on the contralateral shoulder (arm across chest). The examiner attempts to lift the hand off the shoulder with a perpendicular force while the patient resists.
Positive: Inability to maintain the hand on the opposite shoulder (examiner can lift the hand).
Interpretation: Tests upper subscapularis fibers. - Miller's Table 4.7
II. SHOULDER INSTABILITY TESTS
9. Apprehension Test (Crank Test for Anterior Instability)
Procedure: Patient is supine (or sitting/standing). The shoulder is abducted to 90 degrees and the elbow flexed to 90 degrees. The examiner slowly and gently externally rotates the shoulder while applying slight anterior pressure on the humeral head.
Positive: The patient feels apprehension (fear of dislocation), not merely pain.
Interpretation: Apprehension indicates anterior glenohumeral instability. The humeral head is at risk of subluxating or dislocating anteriorly. - Bailey & Love, p. 509; Miller's Table 4.7
10. Relocation Test (Jobe Relocation Test)
Procedure: Performed immediately after a positive apprehension test. With the patient supine, the examiner applies a posteriorly directed force on the anterior humeral head while maintaining the arm in 90 degrees abduction and external rotation.
Positive: Relief of apprehension (and/or pain) with the posterior force.
Interpretation: Confirms anterior instability. The posterior force relocates the humeral head back into the glenoid, eliminating the sensation of impending dislocation. A positive predictive value of 96% for anterior instability. - Rockwood & Green's; Miller's Table 4.7
11. Load-and-Shift Test
Procedure: Patient seated or supine. Examiner stabilizes the scapula with one hand and grasps the humeral head with the other, applying axial load ("loading") to seat the humeral head in the glenoid, then shifts the head anteriorly, posteriorly, and inferiorly.
Grading (Translation):
- Grade 0: Minimal translation
- Grade 1: Head rides to glenoid rim but does not sublux over
- Grade 2: Head rides over rim but spontaneously reduces
- Grade 3: Head locks over the rim (dislocation)
Interpretation: Quantifies glenohumeral laxity and instability in all directions. Compare to contralateral shoulder for bilateral laxity. - Miller's Table 4.7
12. Sulcus Sign
Procedure: Patient standing, arm relaxed at the side. The examiner applies a downward (inferior) traction force to the elbow or wrist.
Positive: A visible sulcus (dimple/groove) appears below the acromion (between the acromion and the humeral head).
Grading:
- Grade 1: Sulcus < 1 cm
- Grade 2: Sulcus 1-2 cm
- Grade 3: Sulcus > 2 cm
Interpretation: Indicates inferior glenohumeral instability or laxity of the inferior glenohumeral ligament complex (IGHLC). A grade 2-3 sulcus that persists with the arm in 30 degrees of ER indicates rotator interval pathology. - Miller's Table 4.7
13. Jerk Test (Posterior Instability)
Procedure: Patient seated, arm in 90 degrees of forward flexion with internal rotation. The examiner applies a posterior axial loading force through the elbow (pushing humerus posteriorly) while horizontally adducting the arm.
Positive: A sudden "jerk" or clunk is felt as the humeral head subluxes posteriorly over the glenoid rim.
Interpretation: Indicates posterior glenohumeral instability or posterior labral tear. The reverse jerk (moving arm from adduction to abduction) may reproduce a second clunk as the head reduces. - Miller's Table 4.7
14. Kim Test (Posterior-Inferior Labral Tear)
Procedure: Patient seated, arm at 90 degrees abduction. Examiner applies axial load and elevates the arm to 45 degrees (diagonal), then simultaneously applies posterior-inferior force on the proximal arm with lateral compression.
Positive: Sudden pain or jerk sensation.
Interpretation: Highly sensitive for posterior-inferior labral tears and posterior instability. Combined with the Jerk test, sensitivity for posteroinferior labral lesion approaches 97%. - Rockwood & Green's
15. Gagey (Hyperabduction) Test
Procedure: Examiner stands behind the patient and stabilizes the scapula with one hand. The other hand abducts the arm passively.
Positive: Hyperabduction > 105 degrees (> 15 degrees asymmetry from contralateral side).
Interpretation: Indicates incompetency of the inferior glenohumeral ligament complex. Normal limit is 90 degrees of passive abduction with scapular fixation. - Rockwood & Green's
III. LABRUM / BICEPS TENDON TESTS
16. O'Brien Test (Active Compression Test)
Procedure: Patient standing, arm in 90 degrees of forward flexion, 10-15 degrees of horizontal adduction (across midline), and full internal rotation (thumb pointing down). The examiner applies a downward force while the patient resists. The test is then repeated with the arm in full supination (palm up).
Positive: Pain or click in the pronated position that is relieved (or absent) in the supinated position. Deep joint pain indicates SLAP lesion; pain on top of the shoulder indicates AC joint pathology.
Interpretation: - Positive with pronation + negative with supination = SLAP lesion. - Pain at AC joint in both positions = AC joint pathology. - Miller's Table 4.7; Campbell's
17. Crank Test (SLAP lesion)
Procedure: Patient standing or supine, arm elevated to 160 degrees in the scapular plane. The examiner applies an axial load through the elbow (compressing the glenohumeral joint) while rotating the humerus internally and externally.
Positive: Pain (with or without a click) during rotation, usually in external rotation.
Interpretation: Indicates SLAP (Superior Labrum Anterior to Posterior) tear. The compressive rotation impinges the torn superior labrum. - Miller's Table 4.7
18. Speed Test (Biceps Tension Test)
Procedure: The patient holds the arm in full elbow extension, forearm supinated, shoulder forward flexed to approximately 90 degrees. The examiner applies downward resistance while the patient attempts to maintain the position.
Positive: Pain (and sometimes weakness) in the bicipital groove or anterior shoulder.
Interpretation: Indicates biceps tendon pathology (tenosynovitis, tendinopathy) or SLAP lesion. Sensitivity 38.3%, Specificity 83.3%. - Miller's Table 4.7; Campbell's Table 51.2
19. Yergason Test
Procedure: Patient seated, elbow flexed to 90 degrees, forearm pronated. The examiner resists active supination and external rotation of the forearm/arm.
Positive: Pain in the bicipital groove.
Interpretation: Indicates bicipital tendinopathy or instability of the biceps tendon in its groove (long head of biceps).
20. Anterior Glide Test
Procedure: Patient standing with hand on hip. Examiner loads the glenohumeral joint from behind, applying anterosuperior force while the patient resists.
Positive: Pain with the maneuver.
Interpretation: Indicates SLAP lesion. - Miller's Table 4.7
IV. ACROMIOCLAVICULAR JOINT TESTS
21. Cross-Body Adduction Test (Cross-Arm Test)
Procedure: Arm elevated to 90 degrees of forward flexion, then adducted horizontally across the body toward the opposite shoulder.
Positive: Pain at the acromioclavicular joint.
Interpretation: Compresses the AC joint, indicating AC joint arthritis or osteolysis of the distal clavicle. Sensitivity 38.3%, Specificity 83.3%. - Campbell's Table 51.2
22. AC Joint Palpation and Piano Key Sign
Procedure: Direct palpation of the AC joint. For the piano key sign: pressure is applied downward on the distal end of the clavicle.
Positive Piano Key: Clavicle springs back up when pressure is released, like a piano key.
Interpretation: Indicates AC joint disruption (Grade 3+ sprain), where the distal clavicle is superiorly displaced.
V. NEUROLOGICAL / THORACIC OUTLET TESTS
23. Spurling Test (Cervical Radiculopathy)
Procedure: Neck is passively extended and laterally flexed toward the symptomatic side, then the examiner applies axial compression downward on the head.
Positive: Reproduction of radicular symptoms (pain/tingling) down the arm.
Interpretation: Indicates cervical nerve root compression. Important to differentiate cervical from shoulder pathology. - Textbook of Family Medicine 9th Ed
24. Shoulder Abduction Relief Sign
Procedure: The patient actively places the hand of the symptomatic arm on top of the head.
Positive: Relief of arm/shoulder pain with this maneuver.
Interpretation: Suggests cervical root compression (radiculopathy), not primary shoulder pathology. Helps distinguish cervical from intrinsic shoulder conditions. - Campbell's Operative Orthopaedics
VI. FROZEN SHOULDER / GLENOHUMERAL OSTEOARTHRITIS
25. Passive Range of Motion Assessment
Procedure: Examiner passively moves the shoulder through all planes: forward flexion, external rotation (arm at side), and internal rotation (hand behind back). Compare active vs. passive ROM.
Interpretation:
- Frozen shoulder (adhesive capsulitis): Both active and passive ROM are equally restricted in a capsular pattern (ER > FF > IR most restricted).
- Rotator cuff tear: Active ROM reduced but passive ROM preserved (or closer to normal).
- Glenohumeral OA: Reduced passive ROM with crepitus.
Summary Table
| Test | Structure Tested | Position | Positive Finding |
|---|---|---|---|
| Neer Sign | Subacromial impingement | Passive FF >90° in IR | Pain 70-120° arc |
| Hawkins-Kennedy | Subacromial impingement | 90° FF + forced IR | Pain reproduced |
| Painful Arc | Supraspinatus/bursa | Active abduction | Pain 60-120° |
| Jobe (Empty Can) | Supraspinatus | 90° abd + 30° FF, thumb down, resist | Pain or weakness |
| Drop Arm | Supraspinatus (full tear) | Release arm from 90° FF | Arm drops suddenly |
| Hornblower Sign | Infraspinatus/teres minor | Resisted ER at 90° abd | Inability to ER |
| Lift-Off | Subscapularis | Hand off back | Cannot lift off |
| Belly-Press | Subscapularis | Press abdomen, elbow forward | Elbow drops back |
| Bear-Hug | Upper subscapularis | Hand on opposite shoulder | Cannot resist removal |
| Apprehension | Anterior instability | 90° abd + ER | Apprehension (not pain) |
| Relocation | Anterior instability | Post. force on humeral head in apprehension | Relief |
| Load-and-Shift | GH laxity (all directions) | Seated, load + translate head | Graded translation |
| Sulcus Sign | Inferior instability (IGHLC) | Inferior traction, arm at side | Visible sulcus |
| Jerk Test | Posterior instability | 90° FF IR + axial load + horizontal adduction | Clunk/jerk |
| Kim Test | Post-inf labral tear | 90° abd + diagonal loading + post-inf force | Pain/jerk |
| O'Brien | SLAP / AC joint | 90° FF, 10-15° adduction, pronation vs. supination | Pain decreases with supination |
| Crank Test | SLAP | 160° elevation + axial load + rotation | Pain/click |
| Speed Test | Biceps tendon / SLAP | Resisted FF, elbow extended, forearm supinated | Bicipital groove pain |
| Yergason | Biceps tendon (LHB) | Resist supination/ER at 90° elbow flexion | Bicipital groove pain |
| Cross-Body Adduction | AC joint | Horizontal adduction | AC joint pain |
| Spurling | Cervical root | Extension + lateral flex + axial compression | Radicular pain |
| Abduction Relief Sign | Cervical root | Hand on head | Pain relief |
Diagnostic Accuracy Summary (from Campbell's Table 51.2)
| Test | Sensitivity | Specificity |
|---|---|---|
| Neer Sign | 68% | 68.7% |
| Hawkins-Kennedy | 71.5-92% | 44-66.3% |
| Painful Arc | 73.5% | 81.1% |
| Jobe (Empty Can) | 44.1% | 89.5% |
| Speed Test | 38.3% | 83.3% |
| Drop Arm | 26.9% | 88.4% |
| Infraspinatus Test | 41.6% | 90.1% |
| Apprehension + Relocation | --- | PPV 96% (anterior instability) |
Key principle: No single test is perfectly accurate. Combining 5+ positive impingement tests significantly improves diagnostic confidence. Apprehension + Relocation together have the strongest predictive value for anterior instability.
Sources: Miller's Review of Orthopaedics 9th Ed (Table 4.7); Campbell's Operative Orthopaedics 15th Ed 2026 (Table 51.2); Bailey & Love's Short Practice of Surgery 28th Ed (Ch. 35, 38); Tintinalli's Emergency Medicine (Ch. 280); Rockwood & Green's Fractures in Adults 10th Ed; Textbook of Family Medicine 9th Ed.
This is a shared conversation. Sign in to Orris to start your own chat.