Osteoarthritis knee clinical fwatures
Reading File
Finding Sources
Finding Sources
Reading File
Finding Sources
Finding Sources
Reading File
Reading File
Finding Sources
Reading File
Finding Sources
Finding Sources
Reading File
Loading Image
Reading File
Now I have comprehensive information. Let me compile the full answer.
Osteoarthritis of the Knee — Clinical Features
Overview
Knee OA is a degenerative joint disease characterized by articular cartilage loss, subchondral bone changes, osteophyte formation, and mild synovial inflammation. It typically presents in patients in their 50s and beyond, with an insidious onset evolving over years to decades. If a younger patient develops significant OA, an underlying secondary cause should be sought.
Symptoms
Pain
- The dominant symptom and primary driver of clinical decision-making
- Classically mechanical in nature — worse with activity (climbing stairs, rising from a chair), and often worse towards the end of the day
- In early disease: pain occurs only with loading/activity
- In advanced disease: pain may be present at rest or at night
- Pain is nociceptive in nature but central sensitization/neuropathic mechanisms contribute in a substantial proportion of patients
Stiffness
- Localized to the involved joint
- Brief — typically lasts 15–30 minutes or less (contrast with RA, where stiffness lasts >1 hour)
- Most noticeable on first mobilizing after inactivity ("gelling phenomenon")
Crepitus
- Patients may feel and hear a grating or grinding sensation during joint movement
- Most prominent under the patella on knee flexion/extension
Functional Limitation
- Difficulty going up and down stairs
- Difficulty rising from a chair
- Catching or locking of the knee (associated with loose bodies or degenerative meniscal tears)
- Can contribute to falls
Signs on Examination
| Finding | Detail |
|---|---|
| Joint line tenderness | Palpable tenderness along the medial or lateral joint line |
| Crepitus | Palpable on passive/active movement; most prominent under patella |
| Effusion | Soft tissue swelling from synovial fluid accumulation |
| Bony swelling | Palpable osteophytes at joint margins |
| Reduced range of motion | Progressive loss of flexion/extension |
| Varus deformity | Most common; medial compartment narrowing causes "bow-leg" alignment |
| Fixed flexion deformity | Inability to fully extend the knee |
| Valgus deformity | Less common; lateral compartment involvement |
| Peri-articular tenderness | May involve surrounding soft tissues |
| Patellofemoral pain | Pain reproduced on patellofemoral compression |
| Ligamentous instability | May develop in advanced disease |
| Muscle wasting/weakness | Quadriceps atrophy from disuse and pain inhibition |
In early disease, there may be very few visible signs. Signs accumulate as the disease progresses.
Radiographic Features (Investigations)
Plain weight-bearing AP, lateral, and sunrise views typically show:
- Joint space narrowing (medial > lateral compartment; or patellofemoral)
- Osteophytes at joint margins
- Subchondral sclerosis (increased bone density beneath cartilage)
- Subchondral cysts
- Loose bodies (fragments of cartilage/bone — "joint mice")
Importantly, radiographic severity does not correlate well with pain or disability.
Pathological Basis of Findings
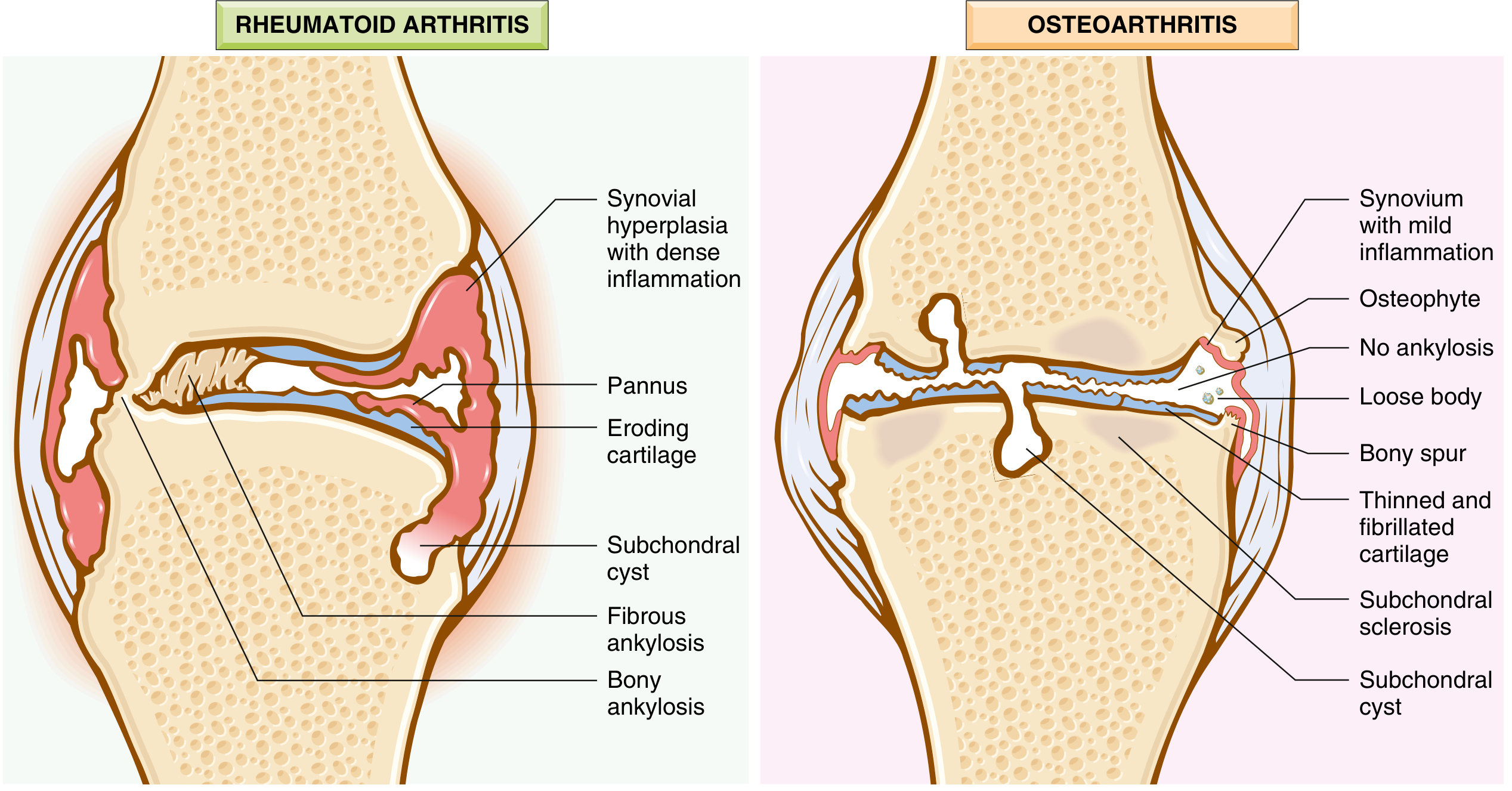
Comparison of OA (right) and RA (left) joint features. OA shows osteophytes, thinned/fibrillated cartilage, subchondral sclerosis, subchondral cysts, loose bodies, and mild synovial inflammation — but no ankylosis or pannus.
| Pathological Change | Clinical Correlate |
|---|---|
| Cartilage fibrillation and thinning | Crepitus, pain |
| Osteophyte formation | Bony swelling, deformity, impingement |
| Subchondral cysts | Seen on X-ray |
| Bone eburnation (ivory-like surface) | Loss of cushioning → pain |
| Loose bodies ("joint mice") | Locking, catching sensation |
| Mild synovial inflammation | Effusion, warmth |
| Quadriceps atrophy | Instability, worsening pain |
Diagnosis
Diagnosis is clinical, based on:
- Symptoms: pain (mechanical), brief morning stiffness, functional limitation
- Examination: crepitus, restricted/painful movement, joint tenderness, bony enlargement
Plain radiographs are not mandatory but are useful for atypical presentations or diagnostic clarity.
Red flags suggesting an alternative/additional diagnosis:
- Morning stiffness >30 min → consider RA
- Recent trauma → fracture
- Hot, swollen joint → crystal arthropathy or septic arthritis
Sources: Goldman-Cecil Medicine, p. 2768–2769; Robbins & Kumar Basic Pathology, p. 791; Rosen's Emergency Medicine, Ch. 48
This is a shared conversation. Sign in to Orris to start your own chat.