Give common heart disease with ECG with ECG graph
common heart diseases ECG findings patterns images diagrams
common heart disease ECG patterns STEMI atrial fibrillation heart block complete ECG strip images
https://geekymedics.com/common-ecg-findings-in-osces
STEMI ST elevation myocardial infarction ECG graph image site:litfl.com OR site:ecglibrary.com
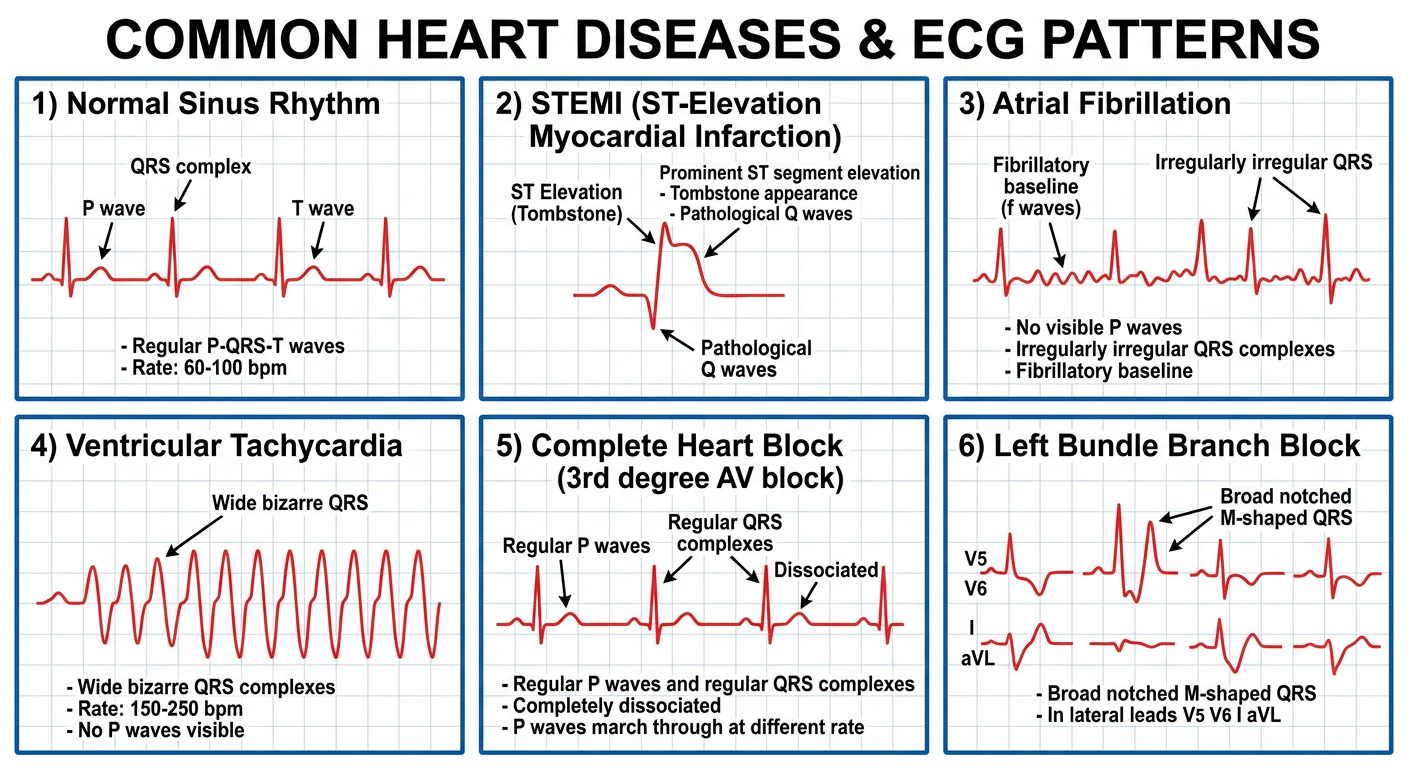
Medical educational poster showing 6 common heart diseases with their ECG graph patterns. Each panel shows: 1) Normal sinus rhythm - regular P-QRS-T waves at 60-100 bpm. 2) STEMI (ST-Elevation Myocardial Infarction) - prominent ST segment elevation with tombstone appearance and pathological Q waves. 3) Atrial Fibrillation - no visible P waves, irregularly irregular QRS complexes, fibrillatory baseline. 4) Ventricular Tachycardia - wide bizarre QRS complexes at 150-250 bpm, no P waves visible. 5) Complete Heart Block (3rd degree AV block) - regular P waves and regular QRS complexes but completely dissociated from each other (P waves march through at different rate). 6) Left Bundle Branch Block - broad notched M-shaped QRS in lateral leads V5 V6 I aVL. Clean clinical diagram style with labeled ECG waves, grid paper background, clear annotations for each condition name and key ECG features.
Common Heart Diseases and Their ECG Findings
ECG Quick Reference - Generated Diagram
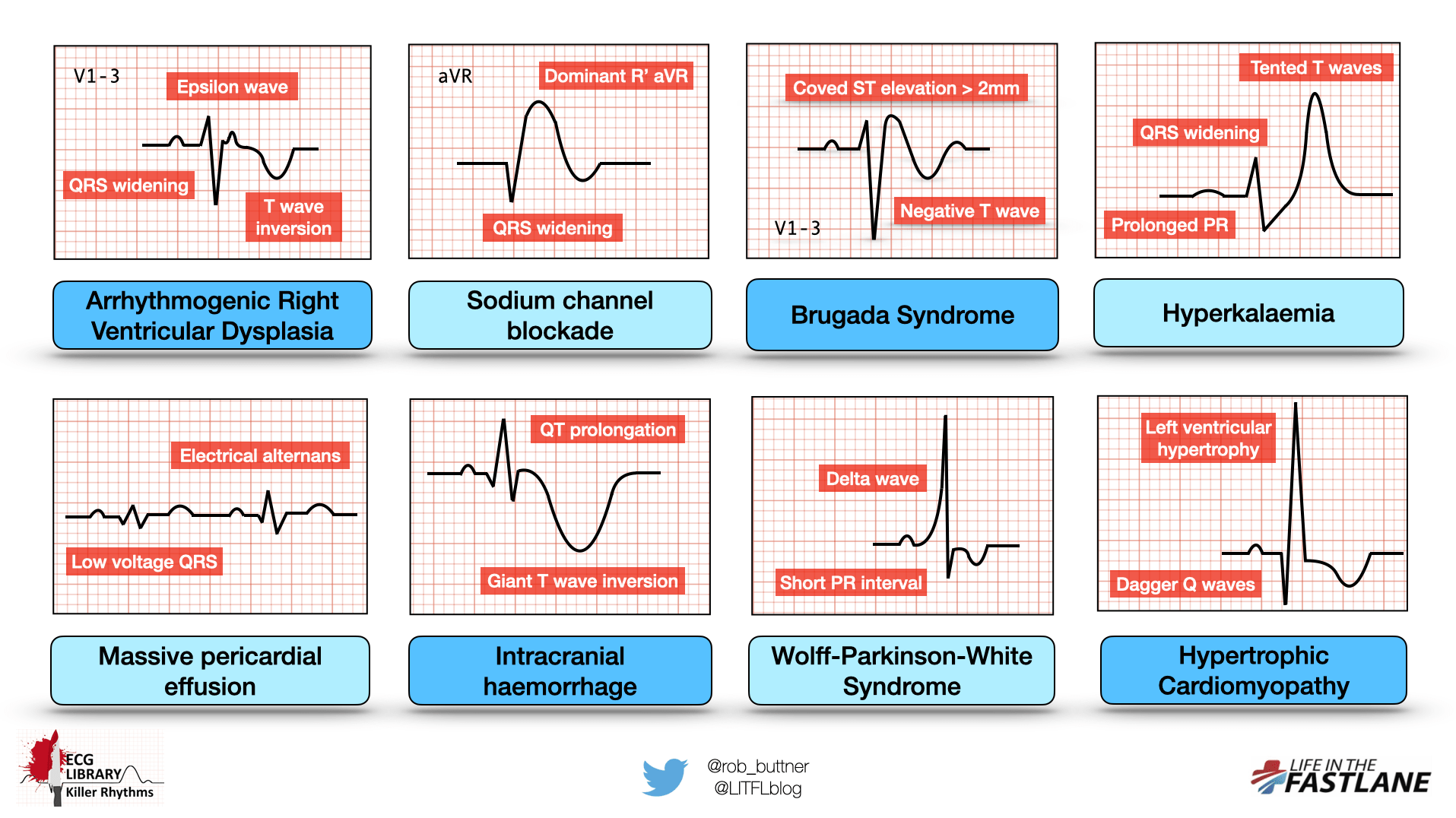
ECG Pattern Reference Chart (from Life in the Fast Lane ECG Library)
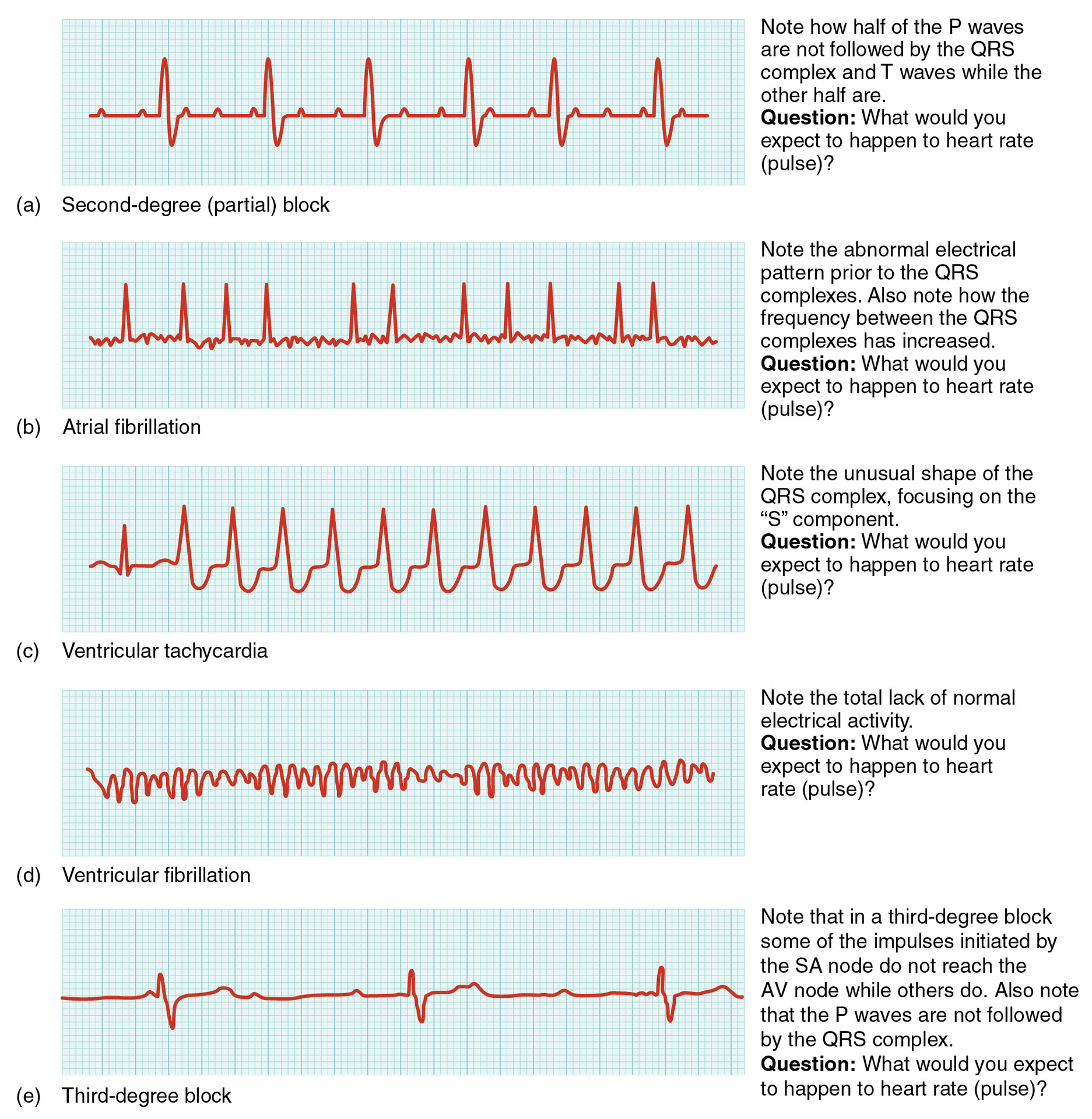
Common Arrhythmias - ECG Strips
1. Normal Sinus Rhythm (Baseline)
- Regular P wave before every QRS
- PR interval: 0.12-0.20 sec
- QRS duration: <0.12 sec
- Normal T wave following QRS
2. ST-Elevation Myocardial Infarction (STEMI) - Heart Attack
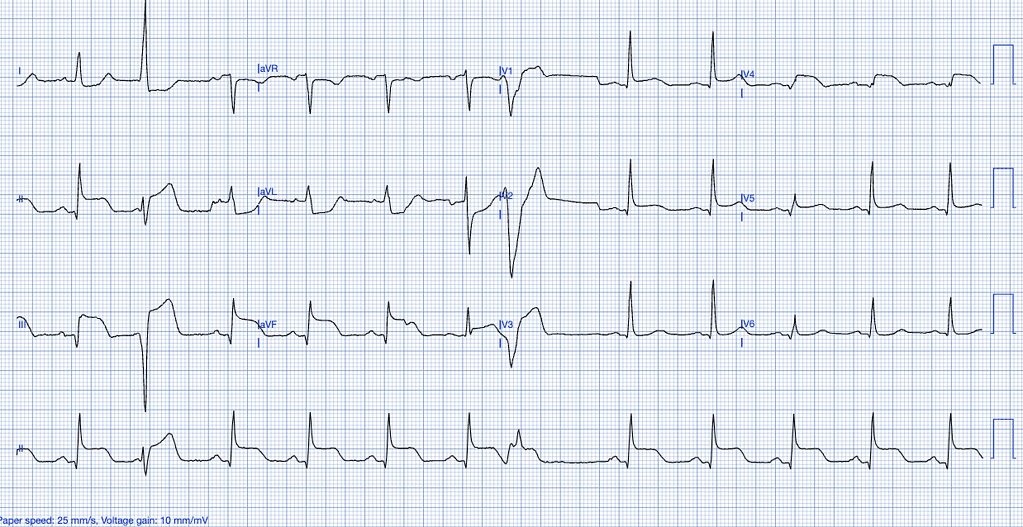
- ST elevation ≥1mm in ≥2 contiguous limb leads, or ≥2mm in precordial leads
- "Tombstone" or "hyperacute" T wave appearance in early phase
- Pathological Q waves develop within hours (>40ms wide, >25% of R wave height)
- Reciprocal ST depression in opposite leads
| Territory | Leads with ST elevation | Artery |
|---|---|---|
| Anterior | V1-V4 | LAD |
| Inferior | II, III, aVF | RCA |
| Lateral | I, aVL, V5-V6 | LCx |
| Posterior | V7-V9 (ST depression V1-V3) | RCA/LCx |
3. Atrial Fibrillation (AF)
- Absent P waves - replaced by chaotic fibrillatory baseline (f-waves)
- Irregularly irregular RR intervals (no pattern at all)
- Ventricular rate 100-160 bpm if uncontrolled
- Narrow QRS complexes (unless aberrant conduction)
4. Ventricular Tachycardia (VT)
- Wide QRS complexes (>0.12 sec, usually >0.14 sec) - bizarre morphology
- Rate 150-250 bpm
- AV dissociation - P waves march through independently (seen in ~50% of cases)
- Fusion beats and capture beats (pathognomonic of VT)
- Concordance in precordial leads (all positive or all negative)
5. Ventricular Fibrillation (VF)
- Completely chaotic electrical activity - no recognizable P, QRS, or T waves
- Rapid irregular undulations of varying amplitude
- No organized rhythm whatsoever
- Requires immediate defibrillation
6. Complete (Third-Degree) AV Block
- Complete AV dissociation - P waves and QRS complexes bear NO relationship to each other
- P waves march at their own rate (usually 60-100 bpm)
- QRS complexes march at their own slower escape rate (20-40 bpm if ventricular, 40-60 if junctional)
- Broad QRS if escape rhythm is ventricular in origin
- Patient is severely bradycardic - requires pacing
7. Second-Degree AV Block
- Mobitz I (Wenckebach): PR interval progressively lengthens until a QRS is dropped, then resets
- Mobitz II: Constant PR interval with sudden non-conducted P waves (more dangerous, often requires pacing)
8. Left Bundle Branch Block (LBBB)
- Broad QRS >0.12 sec (usually >0.14 sec)
- "WiLLiaM" pattern: W shape in V1, M shape in V5/V6
- Broad, notched R waves in I, aVL, V5-V6
- Deep S waves in V1-V3
- No septal Q waves in lateral leads
- New LBBB in the context of chest pain = treat as STEMI equivalent
9. Wolff-Parkinson-White (WPW) Syndrome
- Short PR interval (<0.12 sec) - due to bypassing the AV node
- Delta wave - slurred upstroke at the beginning of QRS
- Broad QRS complex
- Can cause supraventricular tachycardia (SVT) or dangerous AF with rapid conduction
10. Brugada Syndrome
- Coved-type ST elevation >2mm in V1-V3 (Type 1 - diagnostic)
- Followed by a negative T wave
- Can be unmasked by fever, flecainide, or sodium channel blockers
- Risk of VF and sudden death - managed with ICD implantation
11. Left Ventricular Hypertrophy (LVH)
- High voltage QRS - Sokolov-Lyon criterion: S in V1 + R in V5/V6 >35mm
- Left axis deviation
- ST depression and T wave inversion in lateral leads (strain pattern)
- Seen in long-standing hypertension, aortic stenosis, HCM
12. Pericarditis
- Stage 1: Diffuse saddle-shaped ST elevation in almost all leads + PR depression
- Stage 2: ST returns to baseline, T waves flatten
- Stage 3: T wave inversion
- Stage 4: Normalization
- Key: Widespread ST elevation (not in a coronary territory) distinguishes it from STEMI
Quick Summary Table
| Condition | Rate | P waves | QRS | Hallmark feature |
|---|---|---|---|---|
| Normal | 60-100 | Present, regular | Narrow | Baseline |
| STEMI | Variable | Present | Narrow | ST elevation + Q waves |
| Atrial Fibrillation | 100-160 | Absent (f-waves) | Narrow | Irregularly irregular |
| VT | 150-250 | Dissociated | Wide | AV dissociation |
| VF | - | None | None | Chaotic waveform |
| 3rd degree block | 20-60 | Present, regular | Wide/Narrow | P-QRS dissociation |
| LBBB | Normal | Present | Wide | WiLLiaM pattern |
| WPW | Normal | Present | Wide | Delta wave + short PR |
| Brugada | Normal | Present | Normal | Coved ST V1-V3 |
| LVH | Normal | Present | Tall | High voltage + strain |
| Pericarditis | Normal | Present | Narrow | Diffuse saddle ST elevation |