Colle's fracture
Reading File
Finding Sources
Searching PubMed
"Colles fracture" OR "distal radius fracture" management
Reading File
Reading File
Reading File
Loading Image
Loading Image
Reading File
I now have comprehensive information from multiple authoritative sources. Here is the full answer:
Colles' Fracture
Definition
Colles' fracture is a transverse fracture of the distal radial metaphysis - located within 2 cm of the radial articular surface - with dorsal displacement and dorsal angulation of the distal fragment. It is the most common wrist fracture.
(Rosen's Emergency Medicine; Pfenninger and Fowler's Procedures for Primary Care)
Mechanism
- Fall on an outstretched, extended hand (FOOSH)
- Compression forces on the dorsal cortex produce dorsal comminution
- The fracture line may extend into the radioulnar or radiocarpal joint ("die-punch" fracture)
Radiographic Findings
PA view:
- Distal metaphyseal fracture of radius, often appearing shortened
- Intraarticular extension may be visible (radiocarpal or radioulnar joint)
- Radial displacement of the carpus
- Associated ulnar styloid fracture is common (suggests triangular fibrocartilage complex injury)
Lateral view (most informative):
- Dorsal angulation and displacement - the "dinner fork" deformity
- Loss of normal volar tilt of the distal radial articular surface
Here are the X-ray views showing the classic fracture pattern:
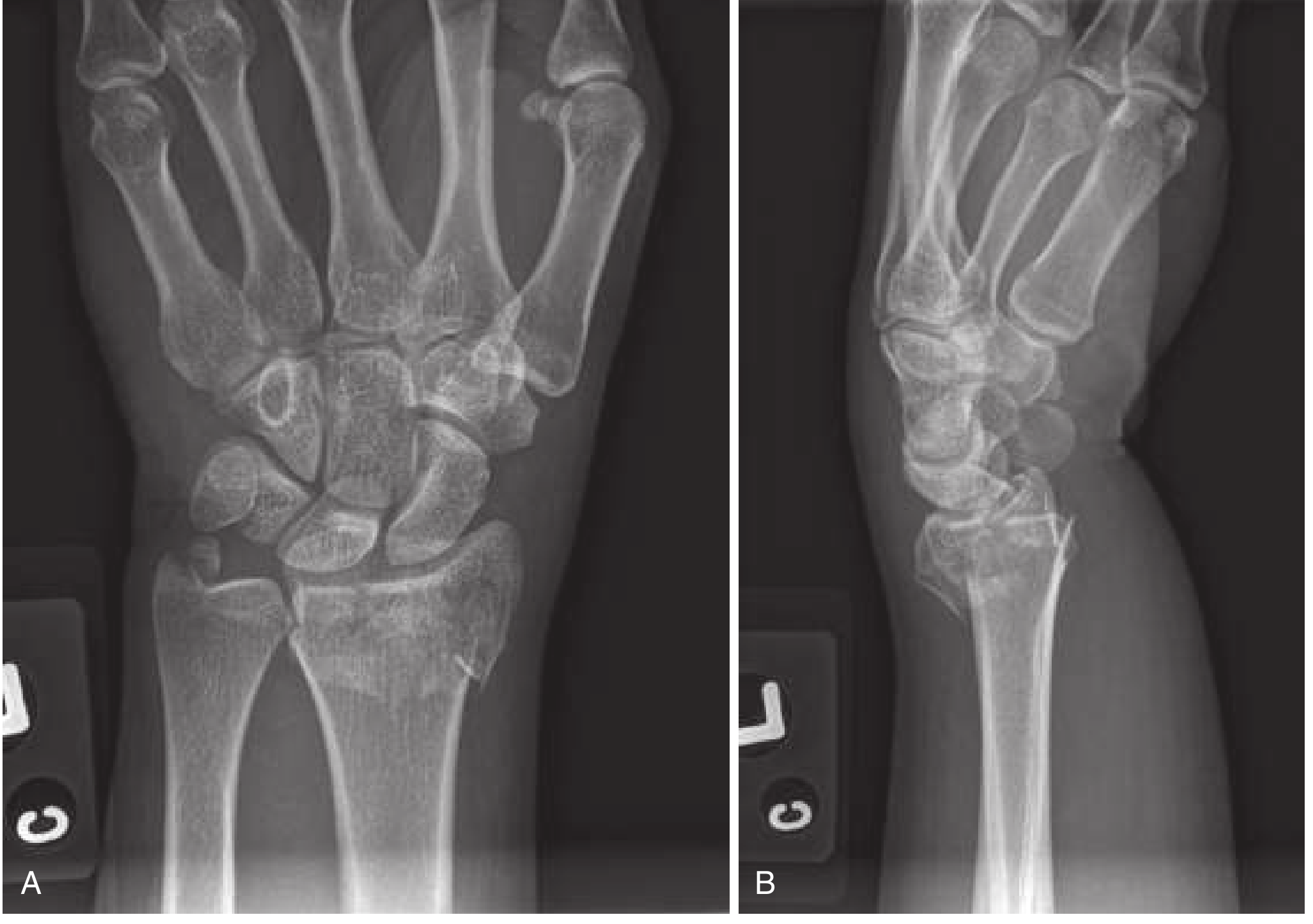
Fig. Colles' Fracture. (A) PA view - fracture, radial shortening, intraarticular extension, ulnar styloid fracture. (B) Lateral view - dorsal displacement and "dinner fork" angulation. (Rosen's Emergency Medicine)
Distal Radius Fracture Patterns (Diagram)
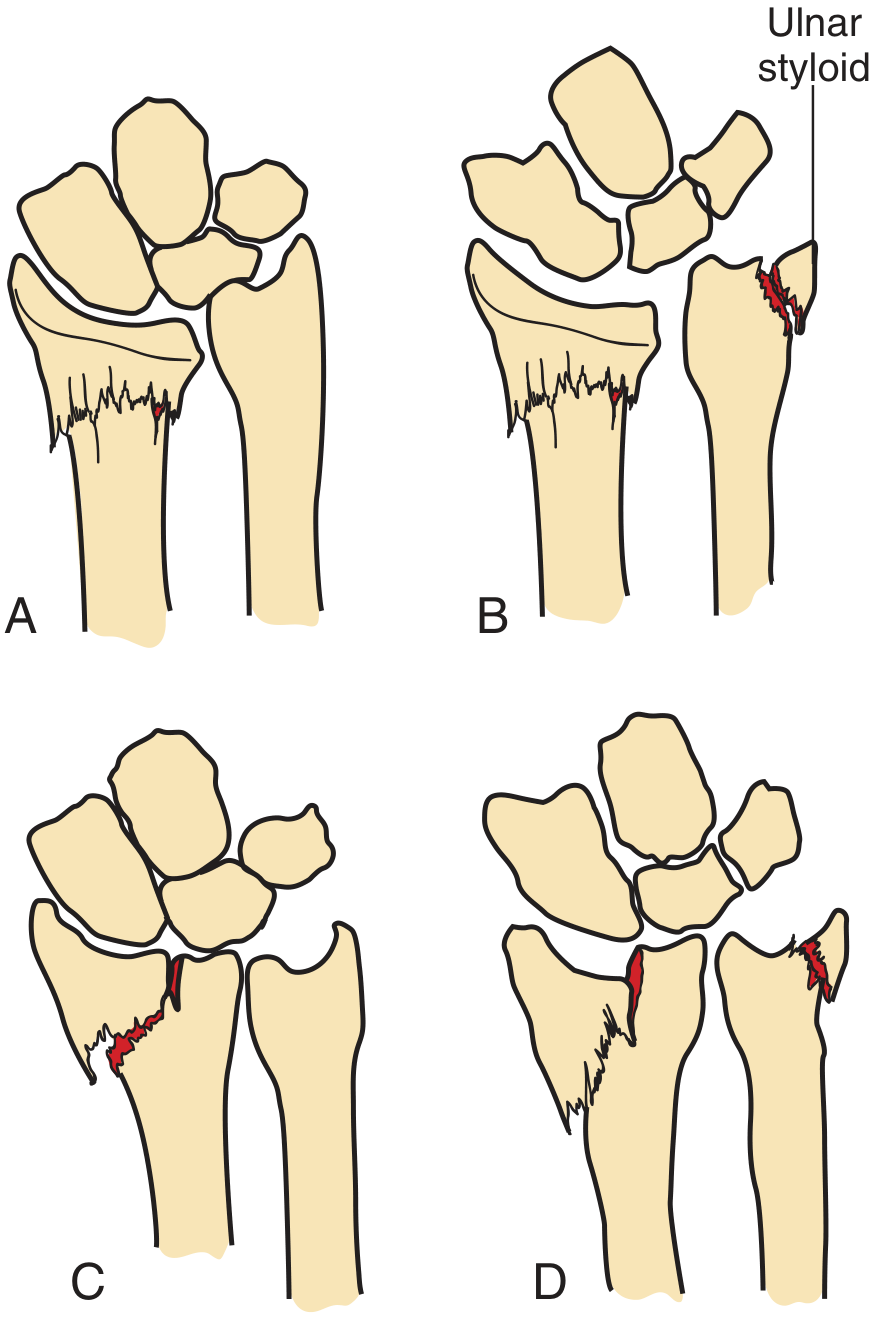
Distal radius fracture patterns. A: Colles'. B: Colles' with ulnar styloid fracture. C: Intra-articular Colles'. D: Intra-articular with ulnar styloid fracture. (Pfenninger & Fowler)
Clinical Features
| Feature | Description |
|---|---|
| Deformity | "Dinner fork" deformity - dorsiflexion hump at wrist |
| Pain/swelling | Localized to distal radius |
| Neurology | Median nerve most commonly injured (paresthesias in palm/fingers) |
| Also check | Radial and ulnar nerve function |
Neurologic exam must be performed before and after reduction and splint application. Median nerve injury may result from contusion, traction, fracture fragment compression, or carpal tunnel syndrome (acute carpal tunnel syndrome, ACTS).
Instability Criteria (higher likelihood of requiring surgery)
- Dorsal angulation > 20 degrees
- Intra-articular involvement
- Marked comminution
- Radial shortening > 1 cm
- Distal radioulnar joint instability
- Radiocarpal instability patterns
CT may be warranted for complex intra-articular or comminuted fractures.
Management
Stable, Nondisplaced, Extra-articular Fractures
- Double sugar-tong splint for 3-5 days (allows swelling)
- Followed by short-arm cast for 4-6 weeks
- Follow-up X-rays at 1, 2, and 6 weeks to ensure no displacement
Displaced / Angulated Fractures - Closed Reduction
Anesthesia options:
- Hematoma block (first-line, easy, effective): 22-gauge needle into dorsum of distal radius, aspirate hematoma, instill 5-10 mL of 1% or 2% lidocaine ± bupivacaine
- IV regional anesthesia (Bier block)
- Regional nerve blocks (median, radial, ulnar, brachial plexus)
- Procedural sedation
Reduction technique:
- Apply finger traps for traction - relaxes deforming muscle spasm, may perform reduction alone
- Push the distal fragment distally and palmarly while holding the forearm firmly
- Goal: restore volar tilt, radial inclination, and radial length
- Acceptable minimum: neutral (0 degrees) volar tilt; ideally restore anatomic volar tilt (~11°)
- Periosteal entrapment: re-create then reverse the mechanism under traction
After reduction:
- Double sugar-tong splint (NOT circumferential cast - edema risk)
- Splint must immobilize wrist but allow finger movement
- Avoid circumferential casting for at least 24 hours
- Urgent orthopedic follow-up within 2-3 days
Indications for Emergent Reduction
- Neurovascular compromise
- Significant deformity
- Soft tissue tenting
Indications for Surgery
- Unstable, severely comminuted, or intra-articular fractures not amenable to closed reduction
- Fractures in the dominant wrist of high-demand active patients
- All open fractures
- Neurovascularly compromised fractures
Complications (occur in 6-80% of cases)
| Complication | Notes |
|---|---|
| Median nerve injury | Most common nerve injury; acute or delayed |
| Radial/ulnar nerve injury | Less common |
| ACTS (Acute Carpal Tunnel Syndrome) | Requires urgent decompression |
| Malunion | Especially with comminution and inadequate reduction |
| Distal radioulnar joint instability | May impair pronation/supination |
| Post-traumatic arthritis | Risk increases with intra-articular extension |
| Complex regional pain syndrome (CRPS/RSD) | More common in older patients |
| Tendon rupture | Extensor pollicis longus classically |
| Loss of reduction | Higher risk with initial instability features |
Complications are more common in older patients, and those with comminution, displacement, and inadequate reduction.
Comparison: Colles' vs. Smith's Fracture
| Feature | Colles' | Smith's ("reverse Colles'") |
|---|---|---|
| Direction | Dorsal angulation | Volar angulation |
| Mechanism | Fall on outstretched hand | Fall on flexed wrist |
| Deformity | "Dinner fork" | "Garden spade" (volar prominence) |
| Treatment | Usually closed reduction | Often requires surgery |
Sources: Rosen's Emergency Medicine, Tintinalli's Emergency Medicine, Pfenninger and Fowler's Procedures for Primary Care
Colle's fracture according to book beiley and love in short understandable way
Finding Sources
Finding Sources
Finding Sources
Finding Sources
Reading File
Reading File
Reading File
Finding Sources
Finding Sources
Finding Sources
Loading Image
Reading File
I have all the Bailey & Love content. Here is a clean, short, and easy-to-understand summary directly from the book:
Colles' Fracture - Bailey & Love's Short Practice of Surgery (28th Ed.)
What Is It?
A dorsally displaced fracture of the distal radius (at the metaphysis, ~2 cm from the wrist joint). It is the most common type of extra-articular (Type A) distal radial fracture.
Named after Abraham Colles, an Irish surgeon who described it in 1814 - before X-rays existed.
How It Happens
- Fall on an outstretched hand (FOOSH)
- Compressive force drives the distal radius upward and backward (dorsally)
- Very common in older, osteoporotic women
Classic Deformity
"Dinner fork" deformity - the wrist looks like the profile of a dinner fork from the side:
- The distal fragment displaces dorsally (backward)
- Associated swelling, tenderness, and restricted wrist movement
X-ray Findings
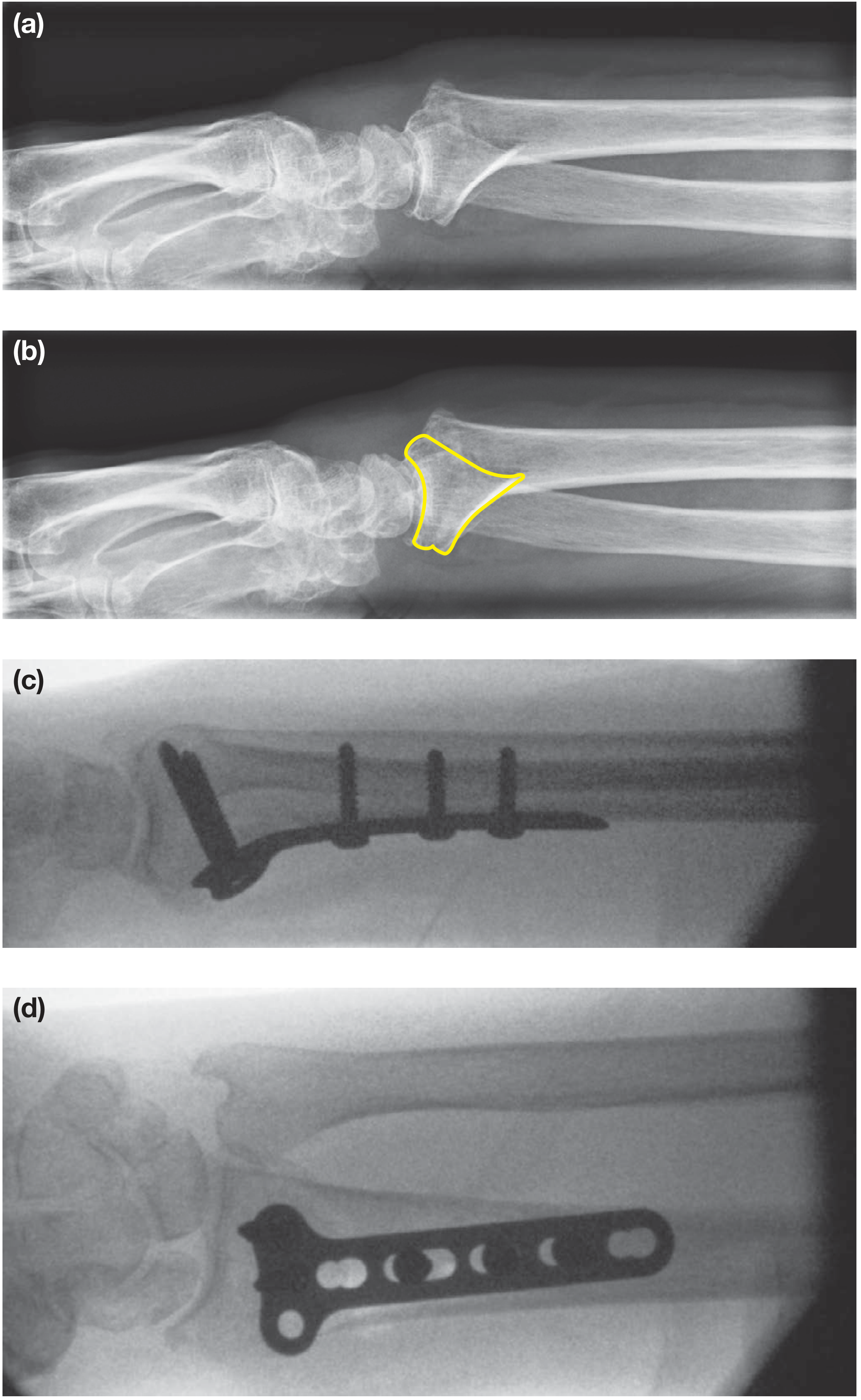
Fig. 32.23 - Extra-articular (Type A) distal radial fracture showing dorsal displacement, and fixation with a volar plate. (Bailey & Love, 28th Ed.)
- Distal radius displaced proximally and dorsally
- Possible ulnar styloid fracture (associated)
- Possible extension into radiocarpal or radioulnar joints ("die-punch" fracture)
Treatment (as per Bailey & Love)
1. Stable / Undisplaced Fractures
- Below-elbow plaster cast until healed (4-6 weeks)
- Keep elbow and shoulder moving to prevent stiffness
2. Displaced Fractures - Closed Reduction + Cast
- Most Colles' fractures (dorsal displacement) can be reduced closed and held in a cast
- However: fractures with significant initial displacement or dorsal comminution are at risk of re-collapsing ("slipping") in the cast
- These need close review with X-rays in the first few weeks
3. Unstable / At-Risk Fractures - Surgery
If the fracture is likely to slip or has already slipped, Bailey & Love describes three surgical options:
| Method | Description |
|---|---|
| K-wires (percutaneous) | Wires placed across fracture fragments through the skin after closed reduction; cast applied for 4-6 weeks |
| Intrafocal K-wires | Wires inserted through the fracture site itself to lever-reduce and lock the fragments |
| Plate and screw fixation | Volar locking plate - most stable, allows early movement |
External fixation is another option, especially for highly comminuted fractures.
4. Intra-articular Fractures (Types B & C)
- Require anatomical reduction of the joint surface
- Gap/step of < 2 mm is acceptable
- Treated with closed reduction + K-wires, plate fixation, or external fixation
In Children
- Usually a Salter-Harris Type 2 physeal fracture or metaphyseal fracture
- Closed manipulation + below-elbow cast works well
- X-ray checks weekly for 3 weeks - if re-displacement occurs, use K-wires
- Growth arrest is rare
Key Points (Bailey & Love Summary)
- Colles' fracture = dorsal displacement of the distal radius
- Most can be treated with closed reduction + cast
- Unstable or comminuted ones need K-wires or plating
- Intra-articular fractures need anatomical joint reduction (< 2 mm step)
- After treatment - move elbow and shoulder to prevent stiffness while in cast
- Opposite injury = Smith's fracture (volar/forward displacement) - usually needs a plate
Source: Bailey and Love's Short Practice of Surgery, 28th Edition, Chapter 32 - Fractures
Green stick fracture according to book bailey and love give in short in exam writing format
Finding Sources
Reading File
Reading File
Loading Image
All the Bailey & Love content is retrieved. Here is the exam-format answer:
Greenstick Fracture
Bailey & Love's Short Practice of Surgery, 28th Ed.
Definition
An incomplete fracture seen exclusively in children and adolescents, where only one cortex fails (the tension side) while the opposite cortex remains intact and bent.
Named after the way a "green" (living, sap-filled) stick breaks - it snaps and splinters on one side but does not break all the way through. (Bailey & Love, Fig. 32.8)
Why It Occurs in Children (Not Adults)
Children's bones are plastic and less brittle than adult bone. When a force is applied, instead of breaking completely across, the bone bends and only the side under tension fails - the compression side merely bends or buckles.
Types of Incomplete Paediatric Fractures (Bailey & Love)
| Type | Mechanism | What Happens |
|---|---|---|
| Greenstick | Bending force | Tension cortex cracks; compression cortex intact |
| Torus / Buckle | Compressive force | Compression cortex buckles; no fracture line through |
| Plastic deformation | Bending force | Bone bends without any visible fracture line |
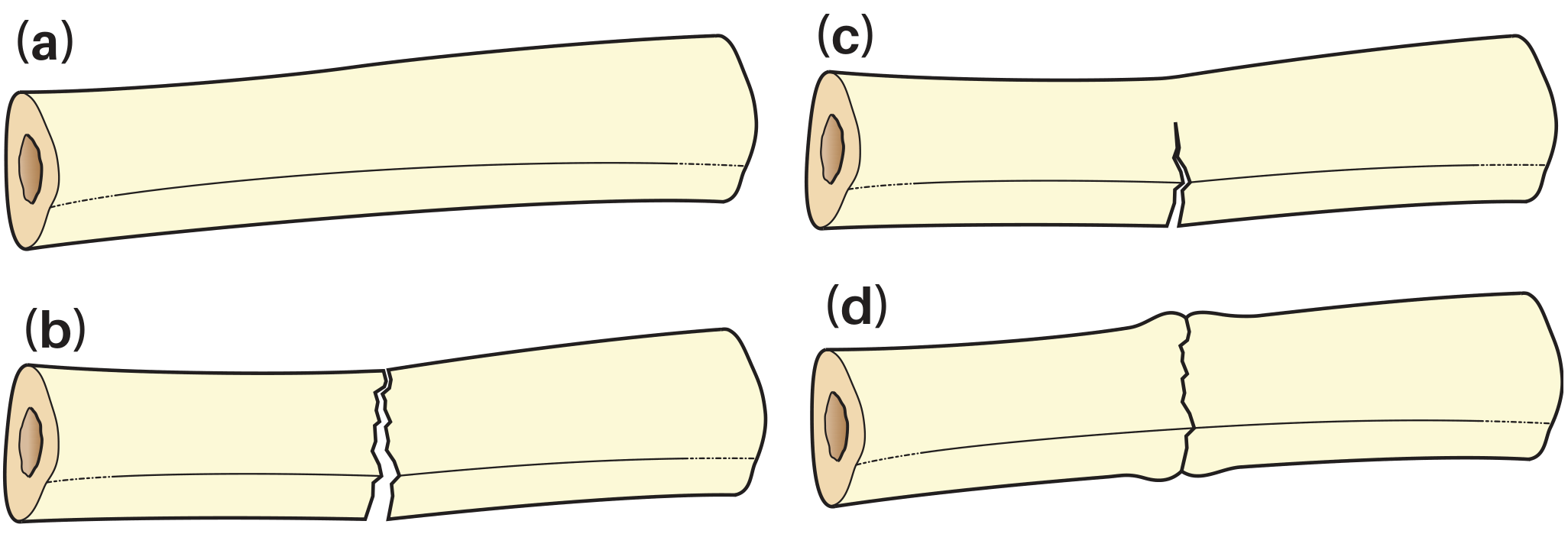
Fig. 32.7 - Types of bony injury. (c) = greenstick; (d) = torus/buckle. (Bailey & Love, 28th Ed.)
Key Features
- Age: Children and adolescents only
- Cortex: One cortex broken (tension side); one intact (compression side)
- Periosteum: Usually intact on compression side - acts as a hinge
- Fracture line: Incomplete - does not cross the whole bone
- Deformity: Angulation present but no complete displacement
- Radiograph: Fracture line visible on one cortex only; opposite side shows bending
Treatment
- Closed reduction under anaesthesia - the deforming force is reversed
- Some surgeons "complete" the fracture intentionally to prevent re-angulation (the intact periosteum can spring back if not fully corrected)
- Immobilised in a plaster cast until healed
- Prognosis is excellent - children's bones remodel well
Important Distinction
| Greenstick | Torus (Buckle) | |
|---|---|---|
| Side affected | Tension cortex cracks | Compression cortex buckles |
| Stability | Less stable (may re-angulate) | Stable |
| Treatment | Reduction often needed | Cast/splint only, no reduction |
Source: Bailey and Love's Short Practice of Surgery, 28th Edition, Chapter 32 - Fractures (p. 443)
This is a shared conversation. Sign in to Orris to start your own chat.