What are the most recent techniques for hernia repair and tell me its procedure step by step also include images wherever possible
Reading File
Finding Sources
Searching the Web
most recent techniques hernia repair 2024 2025 laparoscopic robotic TAPP TEP
Searching PubMed
"hernia repair"[MeSH Terms] AND "surgical procedures"[MeSH Terms]
Reading File
Reading File
Reading File
Loading Image
Searching PubMed
"inguinal hernia" AND "laparoscopic" AND "robotic"
Reading File
Reading File
Loading Image
Searching the Web
TEP TAPP hernia repair step by step procedure technique surgical steps 2024
Loading Image
Loading Image
Reading File
Reading File
Loading Image
Loading Image
I now have comprehensive content from Sabiston, Bailey & Love, and Current Surgical Therapy, plus excellent images. Let me compile the full answer.
Hernia Repair: Modern Techniques with Step-by-Step Procedures
Hernia repair is one of the most commonly performed surgical operations worldwide. The choice of technique depends on hernia type, patient characteristics, surgeon skill, and available equipment. Below is a complete overview of all major modern approaches.
Overview of Techniques
| Technique | Approach | Mesh Used | Key Advantage |
|---|---|---|---|
| Lichtenstein | Open anterior | Yes | Gold standard, widely teachable |
| Shouldice | Open anterior | No | Best tissue-only repair |
| Desarda | Open anterior | No (autologous) | Tension-free without synthetic mesh |
| TEP | Laparoscopic preperitoneal | Yes | No peritoneal entry |
| TAPP | Laparoscopic transabdominal | Yes | Good visualization |
| Robotic TAPP (r-TAPP) | Robotic | Yes | Best dexterity; emerging evidence |
| Single-port Robotic | Robotic, 1 incision | Yes | Cosmesis, faster recovery |
| eTEP (enhanced-view TEP) | Laparoscopic | Yes | Larger working space |
1. Open Anterior Repair - Lichtenstein "Tension-Free" Repair
The Lichtenstein repair is the most common open mesh-based treatment globally, introduced in 1989. It uses polypropylene mesh to reconstruct the posterior wall of the inguinal canal.
Step-by-Step
Step 1 - Incision and Exposure
- Make an oblique incision ~6-8 cm, inferior and medial to the anterior superior iliac spine, ending just lateral to the symphysis pubis.
- Carry dissection down through subcutaneous fat to the aponeurosis of the external oblique muscle. Ligate/cauterize the superficial epigastric veins.
Step 2 - Open the Inguinal Canal
- Open the external oblique aponeurosis along the direction of its fibers using Metzenbaum scissors, extending through the external inguinal ring medially.
- Identify and preserve the ilioinguinal nerve running through the inguinal canal. Identify the iliohypogastric nerve by elevating the external oblique superiorly.
Step 3 - Cord Isolation and Hernia Sac Management
- Isolate the spermatic cord (with any indirect hernia sac) using a Penrose drain for retraction.
- The indirect sac lies on the anterolateral cord surface. Separate it from adjacent cord structures - divide surrounding cremaster fibers carefully.
- Identify and preserve the genital branch of the genitofemoral nerve within the deep spermatic cord.
- For an indirect sac: dissect to the internal ring, reduce/excise the sac, ligate at the ring. For a direct sac: reduce the bulge, do not excise; imbricate the transversalis fascia if bulky.
Step 4 - Assess the Posterior Canal Wall
- Carefully assess for any defect in Hesselbach's triangle (a direct hernia) and at the femoral canal.
- Place interrupted monofilament sutures to close any transversalis fascial defects.
Step 5 - Mesh Placement
- Cut a flat polypropylene mesh (~7 × 15 cm) to fit the inguinal floor. Create a tail with a slit to accommodate the cord.
- Suture the medial end to the pubic tubercle periosteum with a non-absorbable suture, continuing along the inguinal ligament (inferiorly) to the internal ring.
- Suture the mesh superiorly to the internal oblique aponeurosis/muscle.
- The two tails are crossed around the cord and sutured together lateral to the ring to recreate the deep ring.
Step 6 - Wound Closure
- Close the external oblique aponeurosis over the mesh with continuous absorbable suture.
- Close Scarpa's fascia, then skin.
- Current Surgical Therapy 14e, p. 706-710; Bailey and Love's Short Practice of Surgery 28th Edition
2. Pure Tissue Repair - Shouldice Technique
The Shouldice repair is the best non-mesh inguinal hernia repair, with Level 1A evidence for the lowest recurrence among pure tissue repairs. It is the technique of choice when mesh is contraindicated (contaminated field, bowel strangulation).
Step-by-Step
Step 1 - Same incision and exposure as Lichtenstein through Step 3 above.
Step 2 - Floor Division
- Divide the transversalis fascia from the internal ring to the pubic tubercle, creating two flaps.
Step 3 - Four-Layer Repair (Continuous Suture)
- Layer 1: The deep flap of transversalis is sutured to the under-surface of the superior flap (Poupart's ligament region). Run a monofilament non-absorbable suture continuously.
- Layer 2: Return suture - the superficial flap to the shelving edge of the inguinal ligament.
- Layer 3: Internal oblique muscle/aponeurosis sutured to inguinal ligament.
- Layer 4: Return of Layer 3 suture.
- This four-layer running suture technique is the Shouldice hallmark - it distributes tension across multiple tissue planes.
Step 4 - Close wound as in Lichtenstein.
- Current Surgical Therapy 14e; Bailey and Love's 28th Edition
3. Laparoscopic Hernia Repair - TAPP and TEP
Both TAPP and TEP place a large mesh (at least 10 × 15 cm) in the preperitoneal plane, deep to the abdominal wall, extending medially into the retropubic space and at least 5 cm lateral to the deep inguinal ring. This covers Hesselbach's triangle, the deep inguinal ring, and the femoral canal.
Compared with open repair, the laparoscopic approach offers:
- Reduced immediate and long-term pain (up to 5 years)
- More rapid return to activity
- Fewer wound complications
- Particular benefit for bilateral hernias and recurrence after open repair

3A. Totally Extraperitoneal (TEP) Repair
In TEP, the surgeon develops the extraperitoneal plane just deep to the abdominal muscles without entering the peritoneal cavity.
Step-by-Step
Step 1 - Initial Port Access
- Make a 1.5-2 cm infraumbilical incision. Incise the anterior rectus sheath and retract the rectus muscle laterally.
- Insert a balloon dissector trocar into the extraperitoneal (preperitoneal) space.
Step 2 - Space Development
- Inflate the balloon under direct vision to develop the preperitoneal space (the "space of Retzius" and space of Bogros). This is the key distinguishing step of TEP.
- Insufflate CO2 to ~12 mmHg to maintain the preperitoneal space.
- Place two additional 5 mm trocars in the midline (suprapubic region) under direct vision.
Step 3 - Landmark Identification
- Identify: pubic tubercle/symphysis, Cooper's ligament, inferior epigastric vessels, iliopubic tract, vas deferens, gonadal vessels, and the hernia defect(s).
Step 4 - Hernia Sac Dissection
- For indirect hernia: gently separate the sac from cord structures. Small sacs are reduced; large scrotal sacs may be divided and left in situ to avoid cord injury.
- For direct hernia: reduce the pseudosac (preperitoneal fat/transversalis fascia invagination) back through the defect.
Step 5 - Mesh Placement
- Roll a 15 × 10 cm polypropylene mesh and insert through the umbilical port.
- Unroll to cover Hesselbach's triangle, the deep inguinal ring, and femoral space with overlap.
- Mesh should extend 2 cm medial to the pubic tubercle, 3-4 cm above the Hesselbach triangle, and 5-6 cm lateral to the internal ring.
- In TEP, fixation is often not required - the preperitoneal pressure holds the mesh in place.
Step 6 - Desufflation and Closure
- Carefully desufflate under vision to ensure mesh does not curl. The natural abdominal wall pressure holds the mesh in position.
- Close the rectus sheath. Close skin.
- Bailey and Love's 28th Edition, p. 1091-1092; Campbell-Walsh-Wein Urology
3B. Transabdominal Preperitoneal (TAPP) Repair
In TAPP, the surgeon enters the peritoneal cavity first, then incises the peritoneum above the hernia defect to work in the preperitoneal space.
Step-by-Step
Step 1 - Peritoneal Access and Port Placement
- Establish pneumoperitoneum (CO2, 12-14 mmHg). Enter via umbilical Veress needle or Hassan technique.
- Camera port at umbilicus (10-12 mm), two 5 mm working ports lateral and inferior.
- Place patient in Trendelenburg (head-down) position.
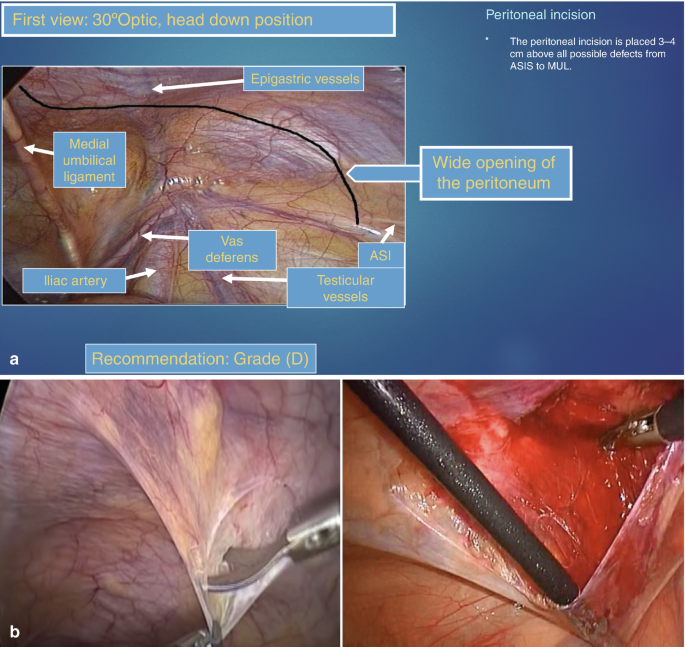
Step 2 - Diagnostic Laparoscopy
- Inspect both inguinal regions. Note the inferior epigastric vessels, medial umbilical ligament, vas deferens, and gonadal vessels. Identify the hernia defect(s): indirect (lateral to inferior epigastric vessels), direct (medial), or femoral.
Step 3 - Peritoneal Incision
- Make a semicircular peritoneal incision ~3-4 cm above the hernia defect(s), running from the medial umbilical ligament to the anterior superior iliac spine (ASIS). This is the critical step unique to TAPP.
- Develop peritoneal flaps cranially and caudally.
Step 4 - Preperitoneal Dissection
- Develop the preperitoneal space (space of Retzius medially, space of Bogros laterally).
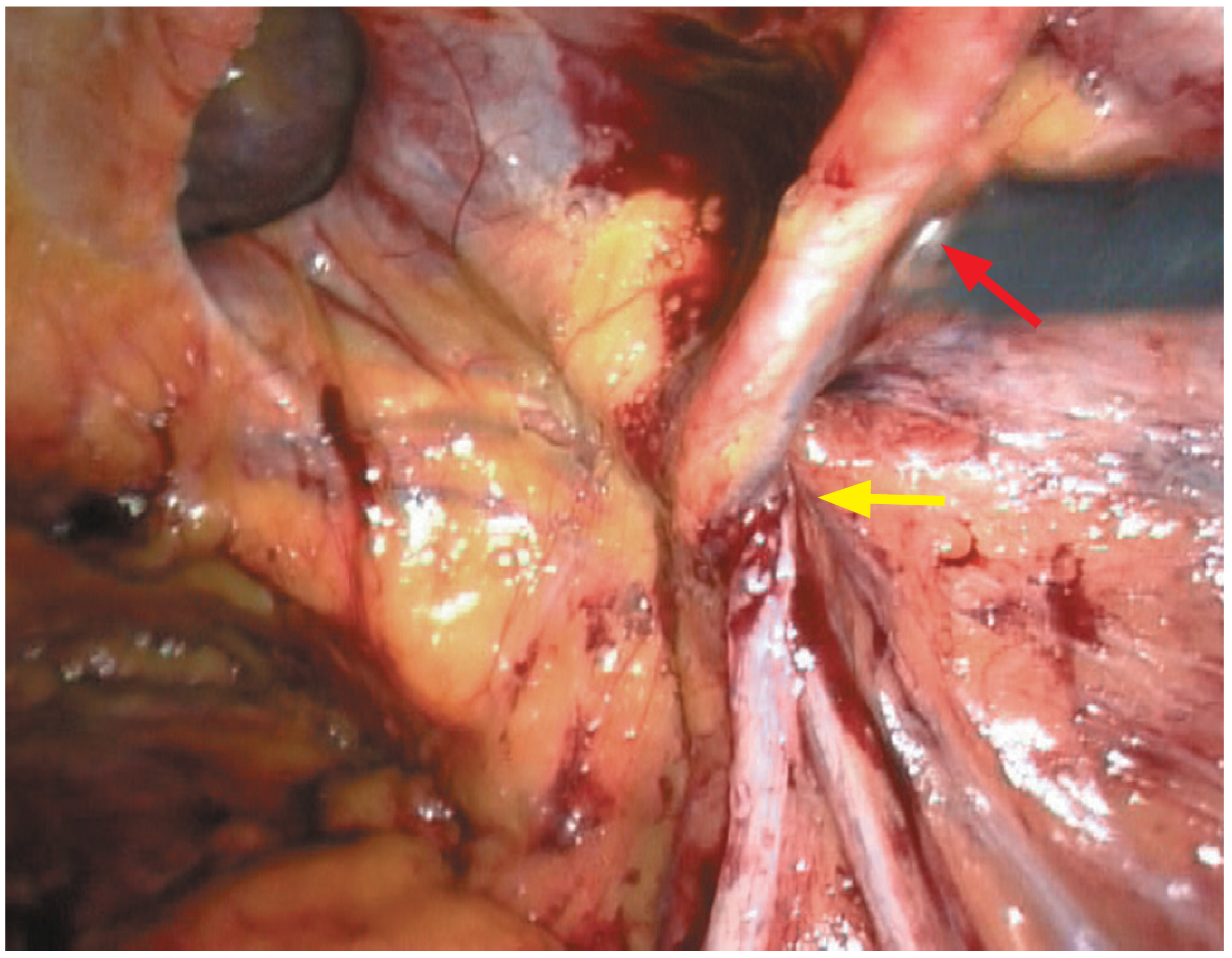
- Identify Cooper's ligament, pubic tubercle, iliopubic tract, and the "triangle of doom" (between vas deferens and gonadal vessels - contains external iliac vessels - must not be stapled).
- Identify the "triangle of pain" (lateral to gonadal vessels - contains the lateral femoral cutaneous nerve and genitofemoral nerve - avoid tacks here).
Step 5 - Hernia Sac Reduction
- Reduce the hernia sac from the preperitoneal space. For large indirect sacs, divide and leave the distal sac to prevent cord injury.
Step 6 - Mesh Insertion and Fixation
- Roll a 15 × 10 cm (minimum) mesh. Insert via the 10-12 mm port.
- Position to cover all potential defect sites with adequate overlap.
- Fixation options: tacker (non-penetrating > penetrating to reduce nerve risk), fibrin glue, or no fixation for small defects.
Step 7 - Peritoneal Closure
- Close the peritoneal flap over the mesh using tacking or running suture - this is essential to avoid mesh contact with bowel (risk of adhesion/fistula).
- Desufflate, close ports.
- Bailey and Love's Short Practice of Surgery 28th Edition, p. 1091-1092; Frontiers in Surgery 2024
4. Robotic Hernia Repair (Most Recent Technique)
Robotic hernia repair has grown dramatically - in Michigan alone, use for inguinal hernia repair increased from 0.7% to 28.8% between 2012 and 2018 (Sabiston Textbook). The robotic approach (r-TAPP) uses the da Vinci system's articulating instruments and 3D vision.
Key Advantages Over Laparoscopic
- Wristed instruments allow easier fascial defect closure and suturing
- Superior 3D visualization and tremor filtering
- Better ergonomics for complex dissection
- Single-port option (da Vinci SP) now available
Robotic Inguinal Hernia Repair (r-TAPP) - Step-by-Step
Step 1 - Patient Positioning and Docking
- Supine position, Trendelenburg.
- Port placement mirrors TAPP but must account for robotic arm collision: 8.5 mm camera port at umbilicus, two 8 mm robotic arm ports placed more lateral than traditional TAPP.
- The robot is docked from between the patient's legs or from the side.
Step 2 - Robotic Peritoneal Entry
- Enter peritoneal cavity. The robotic camera gives a 10× magnified, 3D view.
Step 3 - Peritoneal Incision
- Using robotic scissors/monopolar cautery, create the peritoneal flap exactly as in TAPP (3-4 cm above defect, ASIS to medial umbilical ligament).
- Robotic dexterity makes this incision more precise, especially in obese patients.
Step 4 - Preperitoneal Dissection
- Identify Cooper's ligament, epigastric vessels, vas deferens, gonadal vessels using the high-definition 3D robotic camera. All anatomical triangles (danger zones) are identified.
Step 5 - Sac Reduction and Defect Assessment
Step 6 - Mesh Delivery and Fixation
- The articulating robotic wrists allow easier rolling and deployment of the mesh.
- Suture fixation to Cooper's ligament is possible robotically (not easy laparoscopically) - this is thought to contribute to lower recurrence rates in the RVHR at 2 years.
Step 7 - Peritoneal Closure
- Robotic running suture closure of peritoneum is significantly easier than laparoscopic - this is a key technical advantage of the robotic approach.
Key Trial Data:
- RIVAL Trial (2020): Robotic vs. laparoscopic - no difference in clinical outcomes; robotic had longer operative time and higher cost. No benefit for straightforward inguinal hernias.
- Prospective Hernia Study: Robotic required less pain medication than laparoscopic (P=0.013) and open (P<0.001); faster functional recovery.
- 2025 Meta-analysis (PMID 41384988): Robotic TAPP vs laparoscopic TAPP - similar short-term outcomes.
- Single-port robotic (da Vinci SP, 2023 study): Shorter operative time (78.1 vs 93.2 min, P=0.003) and faster recovery vs multiport.
- Sabiston Textbook of Surgery, p. 163-165
5. Robotic Ventral Hernia Repair (RVHR)
For ventral/incisional hernias, the robotic approach addresses the key limitation of laparoscopic repair - the inability to close the fascial defect.
Step-by-Step
Step 1 - Port placement: camera port contralateral to or away from the hernia site, robotic working ports flanking the hernia defect.
Step 2 - Diagnostic survey and adhesiolysis from surrounding structures.
Step 3 - Defect closure: The articulating wrists allow primary fascial closure using running permanent suture - this is the critical advantage vs laparoscopic.
Step 4 - Mesh deployment (intraperitoneal, anti-adhesive barrier-coated mesh) or retromuscular placement in eTEP approach.
Step 5 - Mesh fixation using running suture. Peritoneal closure over mesh.
Evidence: PROVE-IT RCT - longer operative time (146 vs 94 min) and higher cost for robotic; no difference in pain or hospital stay. A multicenter RCT showed lower hernia recurrence at 2 years with robotic vs laparoscopic (P=0.019).
6. Mesh Technology

Modern meshes fall into three categories:
- Synthetic (most common): Polypropylene, polyester, PTFE. Polypropylene is inert, hydrophobic, and resists infection. Polyester encourages microvascular ingrowth.
- Biologic: Derived from decellularized animal/human tissue - for contaminated fields.
- Composite: Anti-adhesive barrier layer on one face (for intraperitoneal placement).
Mesh plug repairs have been largely abandoned due to "meshoma" formation (fibrous mass) causing chronic pain, and risks of mesh migration and erosion. - Bailey and Love's 28th Edition, p. 1084
Choosing the Right Approach
| Clinical Scenario | Preferred Technique |
|---|---|
| Primary unilateral inguinal hernia, open surgeon | Lichtenstein |
| Bilateral inguinal hernia | TEP or TAPP (one operation) |
| Recurrence after open repair | TEP or TAPP (avoids scarred anterior field) |
| Contaminated field / bowel strangulation | Shouldice (no mesh) |
| Complex ventral/incisional hernia | Robotic TAPP/eTEP |
| Patient requests minimally invasive | TEP or r-TAPP |
Recent Evidence Summary (2024-2025)
| PMID | Year | Finding |
|---|---|---|
| 41384988 | 2025 | Robotic TAPP vs laparoscopic TAPP: similar short-term outcomes (systematic review + meta-analysis) |
| 41452528 | 2025 | Robotic TAPP vs laparoscopic TEP: comparable outcomes (systematic review) |
| 39419843 | 2025 | Single-port vs multi-port laparoscopic/robotic: single-port shows promise for cosmesis |
| 37985490 | 2024 | Robotic surgery for inguinal and ventral hernia: systematic review + meta-analysis |
Complications to Watch For
- Chronic post-herniorrhaphy pain (most common complication, 11-18%): Risk is higher with open approaches. Prevention requires identification and preservation of the ilioinguinal, iliohypogastric, and genital branch of the genitofemoral nerves. Preserving all three reduces chronic pain to <1%.
- Recurrence: Mesh reduces recurrence vs tissue repair (3-fold higher recurrence with Shouldice vs Lichtenstein). Higher risk with smoking, obesity, and poor surgical technique.
- Seroma: More common after laparoscopic repair of large indirect sacs.
- Vascular/nerve injury in laparoscopic: Avoid the triangle of doom (external iliac vessels) and triangle of pain (lateral cutaneous/genitofemoral nerves).
Sources: Current Surgical Therapy 14e, p. 708-710; Sabiston Textbook of Surgery; Bailey and Love's Short Practice of Surgery 28th Edition
This is a shared conversation. Sign in to Orris to start your own chat.