Different type pain and it's management and drugs
Reading File
Finding Sources
Finding Sources
Finding Sources
Searching PubMed
pain classification management analgesics
Reading File
Reading File
Reading File
Finding Sources
Reading File
Finding Sources
Finding Sources
Reading File
Reading File
Loading Image
Reading File
Reading File
I now have comprehensive, authoritative information from Goldman-Cecil Medicine and Schwartz's Surgery to give a thorough answer. Let me compose it.
Types of Pain and Their Management
1. Classification of Pain
Pain is defined as an unpleasant visceral or somatic experience associated with actual, potential, or perceived tissue damage. The modern classification (IASP/Goldman-Cecil Medicine 22E) recognizes four main etiologic categories:
A. Nociceptive Pain
Caused by injury or disease affecting somatic structures - the most common type. Results from stimulation of intact nociceptors (free nerve endings of Aδ and C fibers) by mechanical, thermal, or chemical stimuli.
Subdivided into:
| Subtype | Character | Examples |
|---|---|---|
| Somatic | Sharp, well-localized; aching/diffuse if deeper (bones, joints) | Arthritis, myofascial pain, fractures, postoperative incision |
| Visceral | Poorly localized, deep, aching; often referred to somatic areas | Pancreatitis, renal colic, angina (referred to arm), appendicitis |
Classic descriptors: "throbbing," "aching"; worsens with movements that stress the affected structure.
B. Neuropathic Pain
Caused by a lesion or disease affecting the somatosensory nervous system (peripheral or central). Accounts for 15-25% of chronic pain.
Key features:
- Quality: burning, searing, tingling, shooting, electric shock-like
- Associated with allodynia (pain from normally innocuous stimuli) and hyperalgesia (exaggerated pain response)
- Sensory deficit co-extensive with the pain area on exam
Subdivided into:
| Subtype | Examples |
|---|---|
| Peripheral | Diabetic peripheral neuropathy, postherpetic neuralgia, chemotherapy-induced neuropathy, phantom limb pain, chronic post-surgical pain |
| Central | Central post-stroke pain, spinal cord injury pain, multiple sclerosis pain |
C. Nociplastic Pain (formerly "central sensitization")
Arises from altered nociception without clear tissue damage, biomarkers, or somatosensory system lesion. Characterized by:
- Diffuse, widespread pain
- Fatigue, insomnia, mild cognitive impairment ("fibro fog")
- Multiple coexisting pain conditions
- Sensitivity to light, sound, chemical stimuli
Examples: Fibromyalgia, irritable bowel syndrome, complex regional pain syndrome type I, tension-type headache
D. Mixed Pain
Contains components of nociceptive, neuropathic, and sometimes nociplastic pain. Accounts for >50% of chronic pain in some studies.
Examples: Cancer pain, low back pain, headache/migraine
Acute vs. Chronic Pain
| Feature | Acute | Chronic |
|---|---|---|
| Duration | < 3 months / within expected healing | > 3 months or beyond expected healing |
| Purpose | Protective (withdrawal reflex) | No useful purpose; a "disease" in itself |
| Autonomic features | Present (tachycardia, diaphoresis) | Usually absent |
| Psychosocial impact | Minimal | Major - 50-66% have comorbid depression/anxiety |
2. Pain Assessment
- Visual Analogue Scale (VAS) or Numeric Rating Scale (NRS): 0-10
- Mild: 1-3 | Moderate: 4-6 | Severe: 7-10
- A 30% or greater reduction in pain constitutes meaningful clinical improvement
- Children under 3 years: use behavioral/physiologic scales (facial expression, consolability, limb responses)
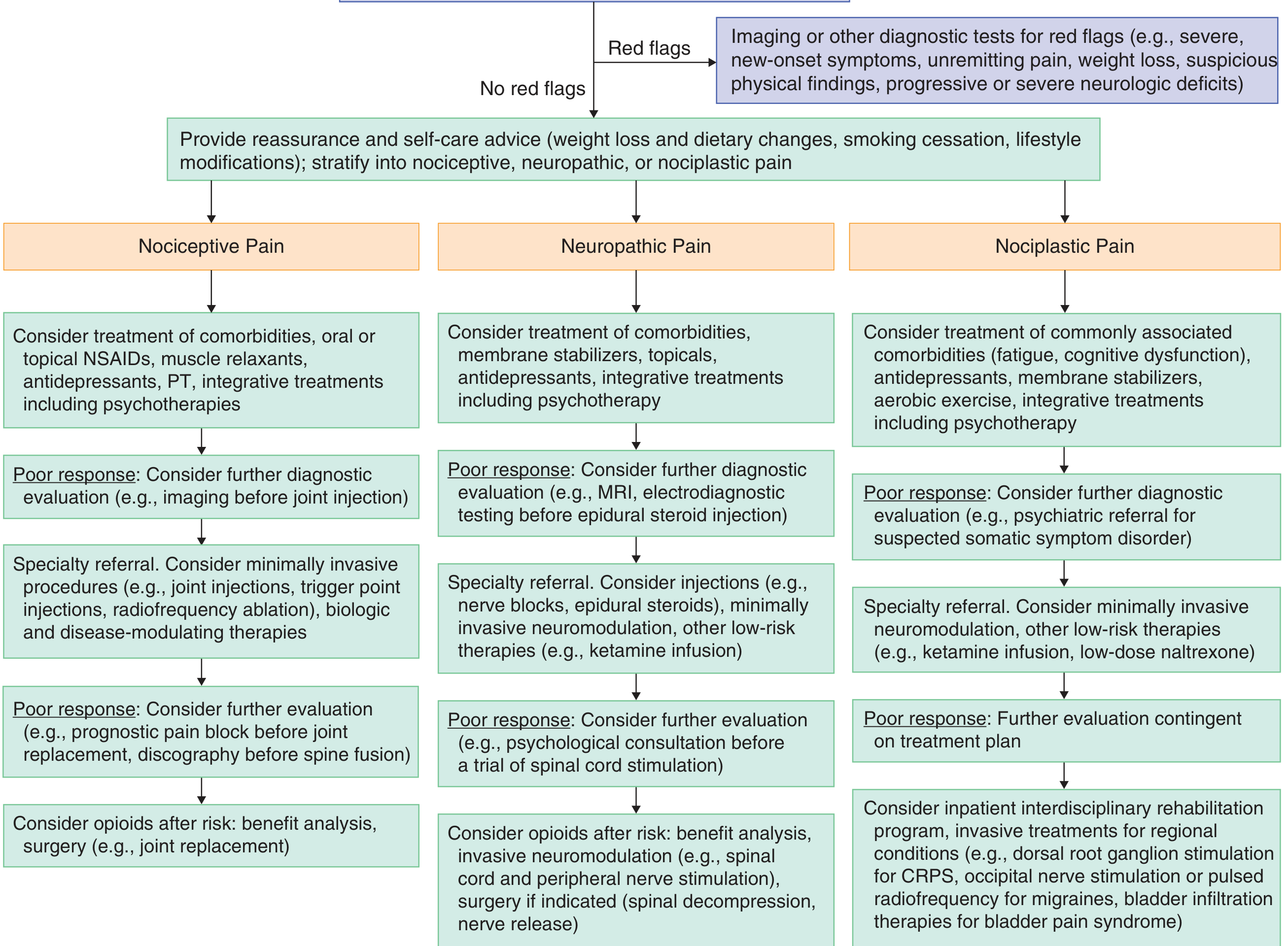
3. Approach to Chronic Pain Management (by type)
The figure below from Goldman-Cecil Medicine illustrates the treatment pathway:
4. Drug Treatment by Pain Type
Step 1 - Mild Pain (VAS 1-3): Non-opioid Analgesics
Acetaminophen (Paracetamol)
- Dose: 325-650 mg PO four times daily; max 3,200 mg/day (use <2,400 mg if other hepatotoxic drugs are taken)
- Mechanism: Acts primarily in the CNS via inhibition of COX; also possible cannabinoid-1 and TRPV1 receptor activity; no significant anti-inflammatory effect
- Caution: Hepatotoxicity in overdose; often ineffective for spinal pain or osteoarthritis
NSAIDs (Non-Steroidal Anti-Inflammatory Drugs)
Work by inhibiting COX-1 and/or COX-2, reducing prostaglandin synthesis both centrally and peripherally.
| Drug | Dose | Notes |
|---|---|---|
| Ibuprofen | 200-400 mg PO QID; max 3,200 mg/day | Gastropathy, nephropathy, platelet effects |
| Naproxen | 250 mg PO BID; max 1,300 mg/day | Available as transdermal gel |
| Aspirin | 600-1,500 mg PO QID | Gastric bleeding, platelet dysfunction |
| Celecoxib (COX-2 selective) | 100-200 mg BID | Fewer GI bleeds, but increased CV and renal risk |
| Diclofenac (topical) | Apply to affected area | Fewer systemic side effects; useful for focal rheumatologic conditions |
NSAID adverse effects: GI ulceration, renal toxicity, increased cardiovascular events, platelet dysfunction. COX-2 inhibitors reduce GI risk but do not eliminate renal/CV risk.
Step 2 - Moderate Pain (VAS 4-6): Weak Opioids
| Drug | Dose | Notes |
|---|---|---|
| Tramadol | 50-100 mg PO every 4-6 hr | Weak mu-opioid agonist + NE/serotonin reuptake inhibitor; risk of seizures |
| Hydrocodone | 5-7.5 mg PO every 4 hr | Most prescribed opioid in the US; often combined with acetaminophen |
| Codeine | 30-60 mg PO every 4-6 hr | Prodrug metabolized to morphine; poor metabolizers (CYP2D6) get no benefit |
| Oxycodone (low dose) | 5 mg PO every 4 hr | Also available combined with acetaminophen or aspirin |
Step 3 - Severe Pain (VAS 7-10): Strong Opioids
| Drug | Dose | Notes |
|---|---|---|
| Morphine | 10 mg PO every 2-4 hr; 2-4 mg IV/SC every 1-2 hr | Standard reference opioid; caution in renal failure (active metabolite accumulates); slow-release form (MS Contin) available |
| Oxycodone (high dose) | 10-30 mg PO every 4-6 hr | Slow-release form (OxyContin) for persistent pain |
| Hydromorphone | 1-3 mg PO/PR every 4 hr; 1 mg IV/SC every 1-2 hr | Suppository available |
| Fentanyl (transdermal) | 12-25 mcg/h patch every 72 hr | NOT for acute pain; not for opioid-naive patients; unpredictable in cachectic patients |
| Methadone | Consult palliative care/pain team | Very effective for neuropathic pain component; long half-life makes dosing complex; multiple drug interactions; extremely inexpensive |
| Tapentadol | 50-100 mg every 4-6 hr | Mu-opioid agonist + NE reuptake inhibitor; about twice as potent as tramadol; ceiling effect |
Opioid adverse effects: Nausea, constipation (virtually universal), sedation, respiratory depression, pruritus, endocrine deficiency (sexual dysfunction, osteoporosis), tolerance, physical dependence, addiction risk (~20-30% misuse; <8% addiction in selected populations).
Important: Opioids are no longer first-line for any non-cancer pain due to limited evidence of quality-of-life improvement versus nonopioid analgesics and significant abuse potential. They remain the mainstay for cancer pain.
Adjuvant Analgesics (Especially for Neuropathic Pain)
These drugs were developed for other indications but provide analgesia, particularly for neuropathic and nociplastic pain.
Antidepressants
| Drug Class | Examples | Use |
|---|---|---|
| TCAs (first-line) | Nortriptyline, Imipramine, Amitriptyline | Neuropathic pain, headache, musculoskeletal pain; nortriptyline/imipramine preferred over amitriptyline (fewer side effects) |
| SNRIs | Duloxetine, Venlafaxine | Diabetic neuropathy, fibromyalgia; approved for multiple pain conditions |
| SSRIs | Fluoxetine, Paroxetine | Least effective for pain; mainly treat comorbid depression |
In terms of analgesic efficacy: TCAs > SNRIs > SSRIs
Anticonvulsants / Membrane Stabilizers
| Drug | Use |
|---|---|
| Gabapentin | Neuropathic pain, postherpetic neuralgia; acts additively with antidepressants and opioids |
| Pregabalin | Diabetic neuropathy, fibromyalgia, postherpetic neuralgia; often better than antidepressants for "lancinating" neuropathic pain |
| Carbamazepine | Drug of choice for trigeminal neuralgia; risk of agranulocytosis limits use |
Topical Agents
| Drug | Use |
|---|---|
| Lidocaine patch (5%) | Postherpetic neuralgia; localized neuropathic pain |
| Capsaicin cream/patch | Depletes substance P; neuropathic pain, osteoarthritis |
| Diclofenac gel | Focal inflammatory/musculoskeletal pain |
Other Adjuvants
| Drug | Use |
|---|---|
| Ketamine (NMDA antagonist) | Refractory neuropathic pain; infusion for complex cases |
| Muscle relaxants (cyclobenzaprine, baclofen) | Musculoskeletal pain with spasm |
| Corticosteroids | Inflammatory pain, cancer pain, nerve compression |
| Bisphosphonates / Calcitonin | Bone pain from metastases or osteoporosis |
| Low-dose naltrexone | Emerging evidence for nociplastic pain (fibromyalgia) |
5. Non-Pharmacological Management
| Modality | Best for |
|---|---|
| Physiotherapy / Exercise | Musculoskeletal, nociceptive, nociplastic pain |
| Cognitive Behavioral Therapy (CBT) | Chronic pain, nociplastic pain |
| Nerve blocks / Epidural steroids | Neuropathic, radicular pain |
| Radiofrequency ablation / Trigger point injections | Nociceptive (facet, myofascial) |
| Spinal cord stimulation | Refractory neuropathic pain, CRPS |
| Transcutaneous Electrical Nerve Stimulation (TENS) | Localized pain |
| Acupuncture | Musculoskeletal, headache |
6. Summary: Drug Selection by Pain Type
| Pain Type | First-Line Drugs | Second-Line / Adjuvants |
|---|---|---|
| Nociceptive (somatic) | NSAIDs, Acetaminophen | Opioids (if severe), muscle relaxants, topical NSAIDs |
| Nociceptive (visceral) | NSAIDs, opioids (for acute) | Antispasmodics, nerve blocks |
| Neuropathic | TCAs (nortriptyline), SNRIs (duloxetine), Gabapentin/Pregabalin | Topical lidocaine/capsaicin, carbamazepine (trigeminal), ketamine |
| Nociplastic | SNRIs (duloxetine), TCAs, aerobic exercise | Gabapentin/pregabalin, low-dose naltrexone |
| Cancer pain | WHO analgesic ladder: NSAID -> weak opioid -> strong opioid + adjuvants | Ketamine, nerve blocks, bisphosphonates, steroids |
| Acute severe pain | Strong opioids IV/IM + NSAIDs | Regional anesthesia, ketamine |
Sources:
- Goldman-Cecil Medicine International Edition (2023), Chapter 26: Pain
- Schwartz's Principles of Surgery, 11th Ed., Chapter on Analgesics for Persistent Pain
- Rosen's Emergency Medicine, Chapter 157: Pain Foundations
- Rheumatology 2-Volume Set (Elsevier, 2022): Types of Pain
This is a shared conversation. Sign in to Orris to start your own chat.