Folic acid
Reading File
Asking for Preferences
Finding Sources
Searching PubMed
"folic acid"[MeSH Terms] AND "deficiency"[MeSH Terms]
Reading File
Reading File
Reading File
Loading Image
Loading Image
Finding Sources
Reading File
Reading File
I now have comprehensive information. Let me compile the full answer.
Folic Acid (Folate / Vitamin B9)
1. Chemistry & Nomenclature
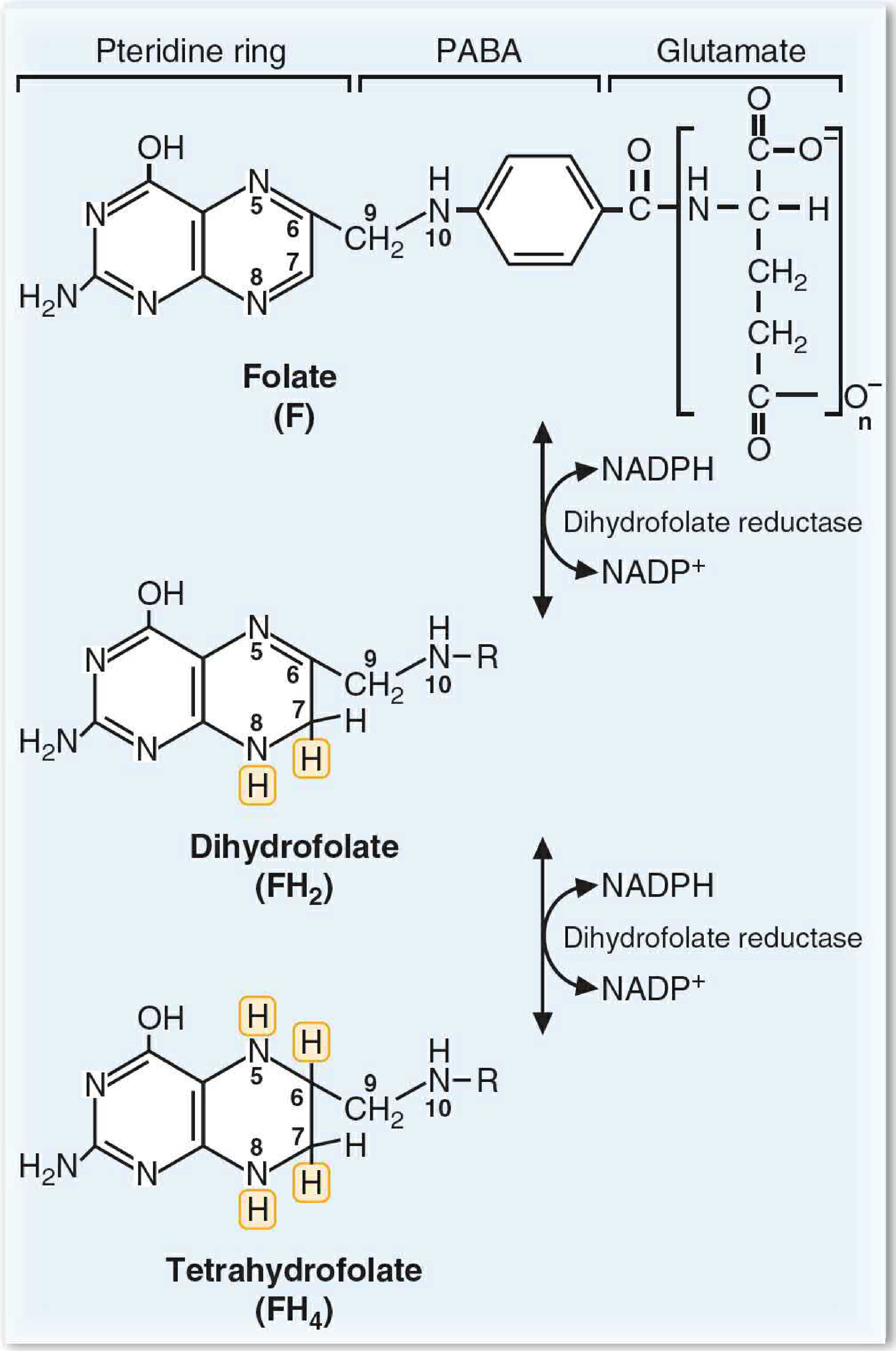
Folic acid is the synthetic, fully oxidized monoglutamate form of the vitamin. The biologically active form in cells is tetrahydrofolate (FH4), a polyglutamate with three structural components:
- A bicyclic pteridine ring
- Para-aminobenzoic acid (PABA)
- A polyglutamate tail (5 glutamate residues joined in amide linkage)
One-carbon groups are bound to N5, N10, or bridging both. Natural dietary folates are mostly in the polyglutamate, partially reduced form. Folic acid supplements and fortified foods contain the fully oxidized synthetic form.
Folic acid is reduced to dihydrofolate (FH2), then to tetrahydrofolate (FH4) by dihydrofolate reductase (DHFR) - the enzyme targeted by methotrexate and trimethoprim.
2. Biochemical Functions
FH4 is a carrier of one-carbon units and is required for:
| Pathway | Role |
|---|---|
| Purine synthesis | Provides one-carbon groups for the purine ring |
| Pyrimidine synthesis | Required for dTMP (thymidylate) synthesis |
| Amino acid metabolism | Interconversion of serine/glycine; synthesis of methionine |
| Homocysteine remethylation | 5-methyl-FH4 donates a methyl group to homocysteine, forming methionine (requires vitamin B12 as cofactor) |
The most critical reaction for hematopoiesis is synthesis of deoxythymidine monophosphate (dTMP), which is essential for DNA replication. Deficiency blocks DNA synthesis while RNA synthesis continues, leading to large cells that cannot divide normally.
3. Dietary Sources, Absorption & Pharmacokinetics
Sources: Green leafy vegetables, citrus fruits, legumes, and fortified grains. The name "folate" comes from Latin folium (leaf). Up to 90% of folate can be destroyed by prolonged cooking.
Absorption:
- Dietary folate is in the polyglutamate form and must be hydrolyzed to monoglutamate before absorption in the jejunum
- This conversion is inhibited by acidic foods and substances in legumes
- Absorbed as 5-methyltetrahydrofolate and then stored in cells as polyglutamate
Key pharmacokinetics:
- Total body stores are relatively small and can be depleted within months of poor intake (contrast with B12 stores lasting years)
- Enterohepatic circulation (bile reabsorption) contributes to folate economy
- RDA: 400 µg dietary folate equivalents (DFE)/day for adults; 600 µg/day in pregnancy; 500 µg/day while breastfeeding
- 1 µg dietary folate = 1 µg DFE; 1 µg supplemental folic acid = ~2 µg DFE (better bioavailability)
US Fortification: Since 1998, the FDA has required 1.4 mg folic acid per kg of refined grain products, reducing low serum folate prevalence from ~24% to <1%.
4. Causes of Deficiency
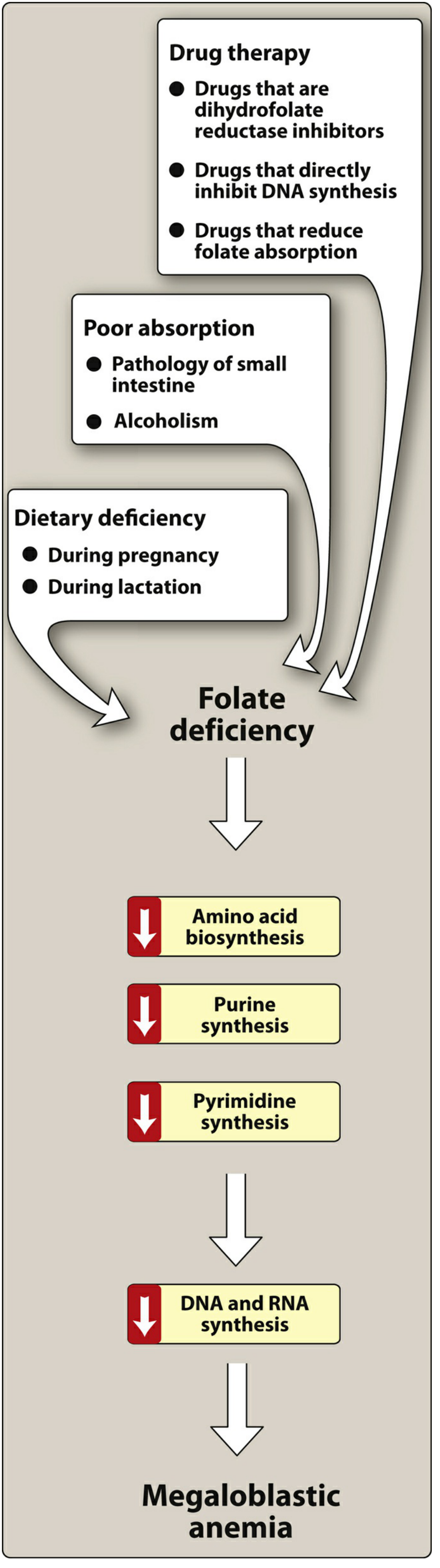
Dietary insufficiency:
- Poor diet (food insecurity, elderly, alcoholism)
- Increased demand - pregnancy, lactation, chronic hemolytic anemias (sickle cell disease)
Malabsorption:
- Celiac disease, Crohn's disease, other small intestinal pathology (folate absorbed in the upper third of small intestine)
- Alcoholism reduces intestinal absorption, hepatic uptake, and increases urinary excretion
Drug-induced:
| Mechanism | Drugs |
|---|---|
| DHFR inhibition | Methotrexate, trimethoprim, pyrimethamine |
| Direct DNA synthesis inhibition | Azathioprine, zidovudine |
| Reduce folate absorption | Phenytoin, phenobarbital |
5. Clinical Features of Deficiency
Megaloblastic (macrocytic) anemia is the hallmark:
- Reduced dTMP synthesis blocks DNA replication
- Erythroid precursors grow but cannot divide - large, abnormal cells result
- Elevated MCV; hypersegmented neutrophils on peripheral blood smear
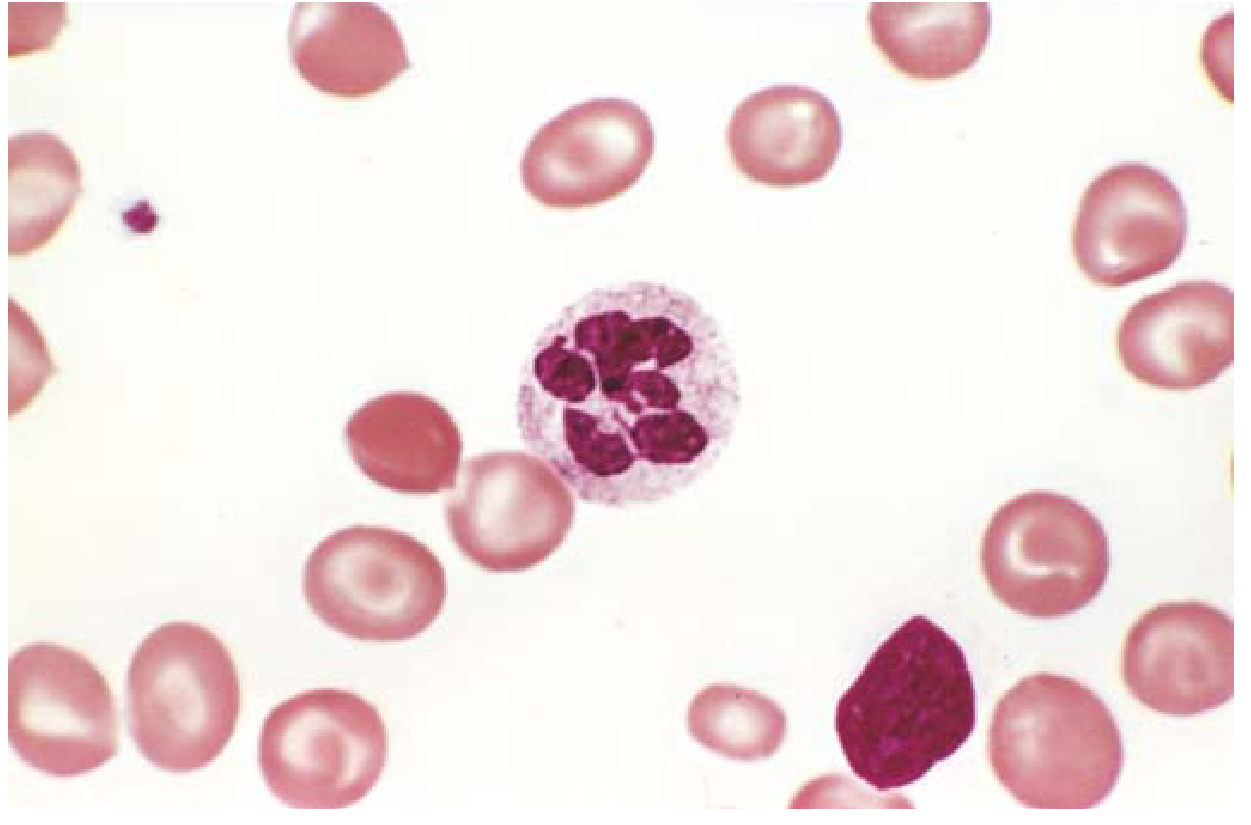
Fig. Peripheral blood smear in megaloblastic anemia showing a hypersegmented neutrophil (6-lobed nucleus).
Other features:
- Weakness, easy fatigability
- Sore tongue (glossitis) - GI epithelium also rapidly turns over
- Diarrhea, malabsorption
- No neurologic complications - this is the key distinction from vitamin B12 deficiency
Critical distinction: Both folate and B12 deficiency cause identical megaloblastic anemia. However, only B12 deficiency causes subacute combined degeneration of the spinal cord (posterior and lateral columns). Treating B12 deficiency with folic acid alone corrects the anemia but allows the neuropathy to progress. Always determine the underlying cause before empiric treatment.
Lab diagnosis:
- Low serum folate (<3 ng/mL)
- Low red cell folate (better reflects body stores)
- Normal or high serum B12 distinguishes folate from B12 deficiency
- Peripheral smear + bone marrow: megaloblasts, hypersegmented neutrophils
6. Clinical Uses of Folic Acid
Neural Tube Defects (NTDs) - Prevention
Folate deficiency in the first 2 weeks of gestation causes failure of neural tube closure, resulting in anencephaly and spina bifida.
- Periconceptional folic acid supplementation reduces NTD risk
- Standard recommendation: 400-800 µg/day for all women of childbearing age
- High-risk (prior NTD pregnancy): 4 mg/day beginning 1 month before conception
- Food fortification has reduced NTD incidence by ~50%
Treatment of Megaloblastic Anemia
- Oral folic acid, rapidly absorbed in the jejunum
- Nontoxic; excess excreted in urine
- Rare hypersensitivity to parenteral injections reported
Homocysteine Lowering
Folate (with B12 and B6) lowers plasma homocysteine. Hyperhomocysteinemia raises the risk of stroke and coronary artery disease. However, meta-analyses of 12 RCTs (n = ~17,000) have shown that folic acid supplementation does not reduce recurrent stroke, coronary events, or mortality in patients with established vascular disease. The role in primary prevention in susceptible populations remains under study.
Cancer
Epidemiological data link higher folate status with lower colorectal cancer risk (proposed mechanism: maintaining DNA methylation and replication fidelity). However, in individuals with pre-existing colorectal adenomas, folic acid supplementation is not advised as it may not prevent, and could promote, recurrence.
Cognitive Function
Some evidence suggests supplementation with 400 µg folic acid + 100 µg B12 daily improves immediate and delayed memory in older adults, possibly through homocysteine lowering.
7. Drug Interactions Summary
| Drug | Effect on Folate |
|---|---|
| Methotrexate | Inhibits DHFR - blocks folate activation |
| Trimethoprim | Weak DHFR inhibitor (bacterial > human) |
| Phenytoin / phenobarbital | Reduce intestinal absorption |
| Sulfasalazine | Impairs absorption and metabolism |
| Oral contraceptives | May reduce folate levels (FDA now approves folate-supplemented OCP formulations) |
Summary Table
| Feature | Folate Deficiency | B12 Deficiency |
|---|---|---|
| Anemia type | Megaloblastic | Megaloblastic |
| Neurologic effects | None | Subacute combined degeneration |
| Onset of deficiency | Months (small stores) | Years (large stores) |
| Common cause | Poor diet, alcohol, malabsorption, drugs | Pernicious anemia, malabsorption |
| Key lab | Low serum/RBC folate | Low serum B12, elevated MMA |
Sources: Lippincott Illustrated Reviews: Pharmacology; Robbins & Kumar Basic Pathology; Yamada's Textbook of Gastroenterology; Basic Medical Biochemistry - A Clinical Approach, 6e
This is a shared conversation. Sign in to Orris to start your own chat.