Decompensated Liver disease
Reading File
Finding Sources
Finding Sources
Searching PubMed
"decompensated liver disease" management
Reading File
Finding Sources
Finding Sources
Finding Sources
Finding Sources
Finding Sources
Reading File
Reading File
Finding Sources
Reading File
Reading File
Reading File
Loading Image
Reading File
Loading Image
Reading File
Excellent - I now have a comprehensive body of content. I have enough to write a detailed, well-structured answer. Let me now compile everything.
Decompensated Liver Disease
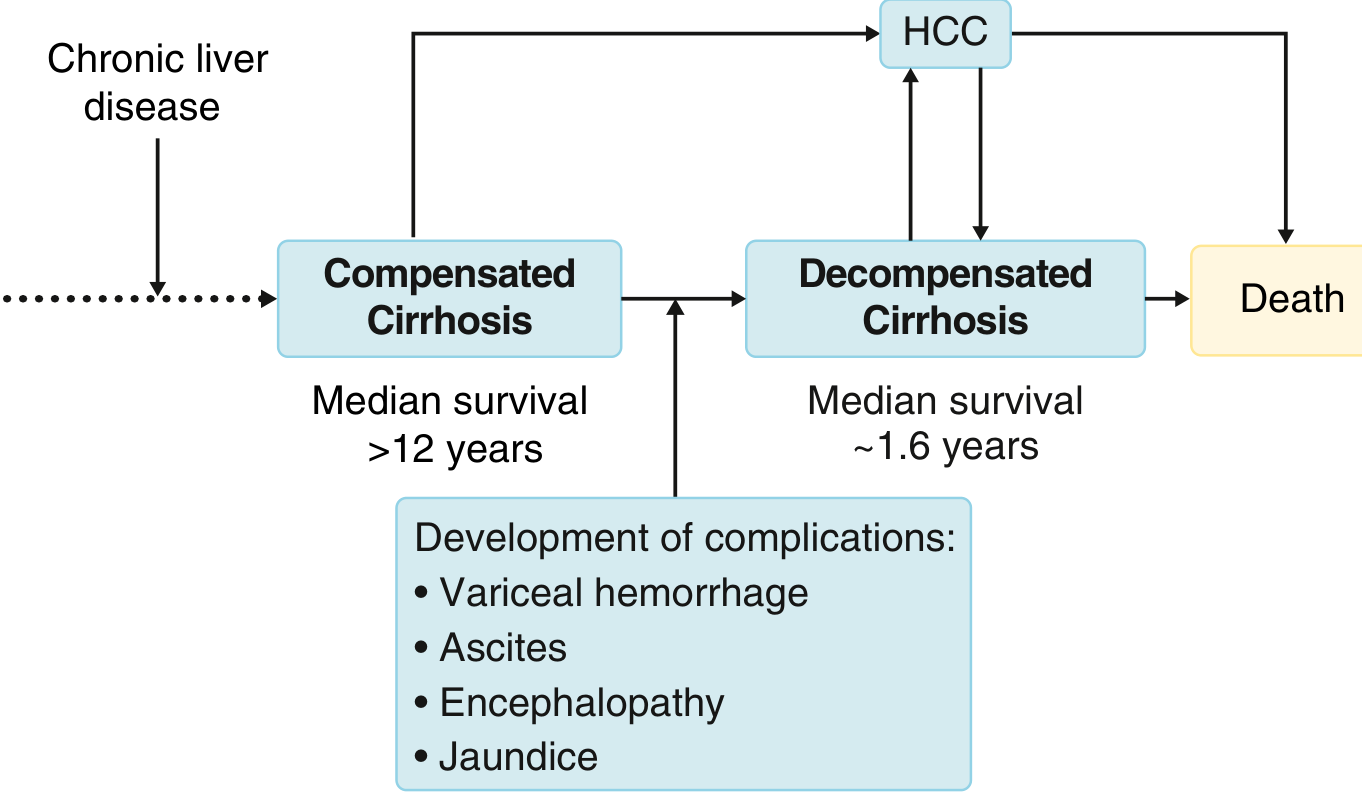
Definition and Natural History
Decompensated liver disease (decompensated cirrhosis) marks the transition from a clinically silent phase to one characterized by overt complications of portal hypertension or liver insufficiency. This transition occurs at approximately 5-7% per year; the median time to decompensation is about 6 years from diagnosis of compensated cirrhosis.
The contrast in prognosis is stark:
- Compensated cirrhosis: median survival >12 years
- Decompensated cirrhosis: median survival ~1.6 years
Pathophysiology
Two main mechanisms drive decompensation: portal hypertension and liver insufficiency.
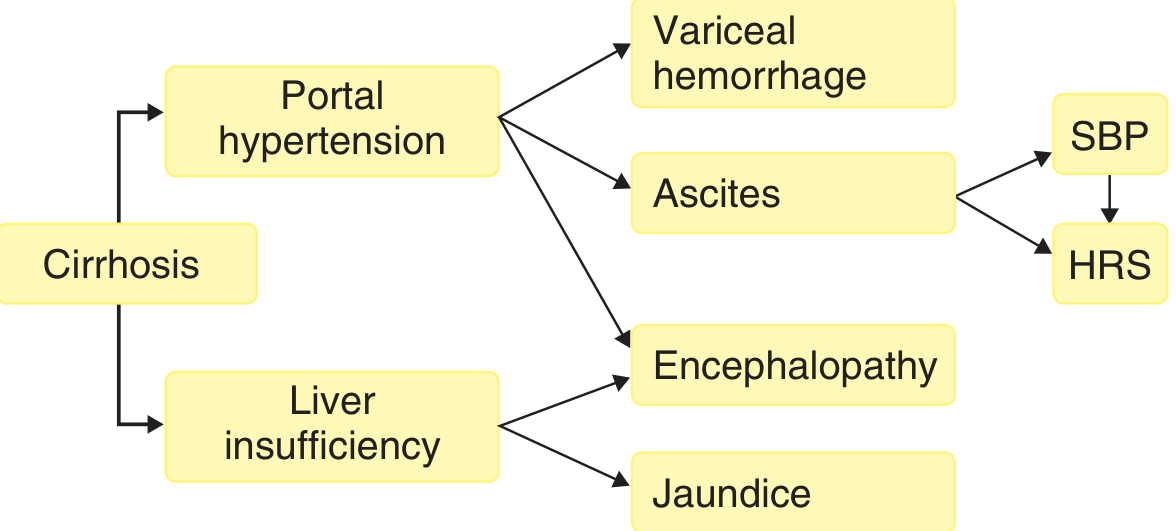
Portal Hypertension
Cirrhosis increases sinusoidal resistance via two components:
- Fixed component - fibrosis and compression from regenerative nodules
- Functional component - intrahepatic vasoconstriction from deficient nitric oxide (NO)
The paradox: intrahepatic NO deficiency causes vasoconstriction and raised resistance, while extrahepatic NO overproduction causes splanchnic and systemic vasodilation. This systemic vasodilation reduces effective arterial blood volume, activating the renin-angiotensin-aldosterone system (RAAS), causing sodium and water retention, and establishing the hyperdynamic circulatory state - which in turn maintains portal hypertension and drives all major complications.
Varices form once the hepatic venous pressure gradient (HVPG) reaches 10-12 mmHg. Ascites requires HVPG >12 mmHg.
Clinical Features of Decompensation
Decompensation is defined by the presence of one or more of:
| Feature | Frequency |
|---|---|
| Ascites | Most common - present in 80% of decompensated patients |
| Variceal hemorrhage | ~50% of cirrhotic patients have varices at diagnosis |
| Hepatic encephalopathy | Due to portosystemic shunting + liver insufficiency |
| Jaundice | Due to liver insufficiency alone |
Major Complications
1. Ascites
Ascites results from sinusoidal hypertension combined with sodium retention. Progressive vasodilation leads to refractory ascites, dilutional hyponatremia, and eventually hepatorenal syndrome (HRS).
Management:
- Sodium restriction; diuretics (spironolactone + furosemide)
- Large-volume paracentesis (>5 L): give albumin 8 g per litre removed
- Refractory ascites: consider TIPS
- Avoid ACE inhibitors and ARBs - these increase plasma drug concentrations, impair renal clearance, and worsen renal function in decompensated cirrhosis
2. Variceal Hemorrhage
Upper GI bleeding from esophageal varices carries a 10-15% mortality per episode. Variceal rupture is driven by variceal wall tension (proportional to diameter and intravariceal pressure, inversely proportional to wall thickness).
Prevalence by Child-Pugh class:
- Child A: ~40% have varices
- Child C: ~85% have varices
Growth of small varices and new varix formation each occur at 7-8% per year.
Management:
- Acute: IV terlipressin or octreotide + endoscopic band ligation; prophylactic antibiotics
- Primary prophylaxis: non-selective beta-blockers (propranolol, carvedilol) or band ligation
- TIPS for refractory/recurrent bleeding (HVPG >20 mmHg signals high risk)
3. Spontaneous Bacterial Peritonitis (SBP)
SBP is infection of ascitic fluid without a primary intra-abdominal source. Pathogenesis involves:
- Bacterial translocation from gut lumen to mesenteric lymph nodes
- Impaired hepatic Kupffer cell clearance (portosystemic shunting bypasses the liver)
- Intestinal bacterial overgrowth (reduced small-bowel motility)
Common organisms: E. coli and Klebsiella (gram-negative).
Diagnosis: Ascitic fluid neutrophil (PMN) count >250 cells/mm³.
Treatment: Cefotaxime 2 g IV every 8 hours for 5 days. Gram-negative infections can precipitate renal dysfunction (HRS) by worsening the hyperdynamic state.
4. Hepatorenal Syndrome (HRS)
HRS results from progressive renal vasoconstriction in the setting of systemic vasodilation. It is heralded by a rising creatinine and carries high mortality.
- Type 1 (HRS-AKI): Rapid deterioration (creatinine doubles to >2.5 mg/dL in <2 weeks); poor prognosis
- Type 2 (HRS-CKD): Slower, associated with refractory ascites
Treatment: Vasoconstrictors (terlipressin or norepinephrine) + albumin; liver transplant is definitive.
5. Hepatic Encephalopathy (HE)
HE is a spectrum of neuropsychiatric dysfunction caused by:
- Ammonia accumulation (from portosystemic shunting and reduced hepatic metabolism)
- Ammonia damages astrocytes → Alzheimer type II astrocytosis
- Upregulation of peripheral-type benzodiazepine receptors → neurosteroid production → GABA-mediated cortical depression
- Manganese accumulation in the globus pallidus → impaired motor function
Note: Severity of HE does not directly correlate with measured serum ammonia.
Precipitants: GI bleeding, infection, hypokalemia, dehydration, constipation, sedatives.
Management:
- Correct precipitants
- Lactulose 30-60 g/day
- Rifaximin 400 mg PO every 8 hours
- Branched-chain amino acid infusion (shown benefit without increased mortality)
6. Cardiopulmonary Complications
- Cirrhotic cardiomyopathy: High-output heart failure with decreased peripheral O₂ utilization
- Hepatopulmonary syndrome (HPS): Pulmonary capillary dilation (up to 500 µm, normal 8 µm) → functional right-to-left shunt → hypoxemia. Corrects with liver transplant.
- Portopulmonary hypertension (POPH): Vasoconstrictive splanchnic substances bypass hepatic metabolism → pulmonary vasoconstriction → if untreated, irreversible obliterative pulmonary hypertension
Prognostic Scoring
Child-Pugh Score
Incorporates bilirubin, albumin, PT/INR, ascites, and encephalopathy. Divides into Class A/B/C.
MELD Score
MELD = 3.78 × ln(bilirubin) + 11.2 × ln(INR) + 9.57 × ln(creatinine) + 6.43
- Used for liver transplant allocation and to predict 90-day mortality
- MELD >15: transplant benefit exceeds surgical risk
- MELD >20 with varices: high risk of post-TIPS decompensation
- Mean arterial pressure (MAP) is an independent predictor of mortality in cirrhosis
Acute-on-Chronic Liver Failure (ACLF)
ACLF is a distinct syndrome of acute decompensation of cirrhosis associated with organ failure(s) and high short-term mortality. It is characterized by systemic inflammatory response (fever, tachycardia, leukocytosis) plus one or more organ failures:
| Organ | Failure Manifestation |
|---|---|
| Brain | Hepatic encephalopathy grade 3-4 |
| Kidneys | Type 1 HRS or need for RRT |
| Circulation | Need for vasopressor support |
| Lungs | ARDS requiring ventilation |
| Liver | Hypoglycemia, lactic acidosis, hyperammonemia, coagulopathy |
| Adrenal | Hypotension |
| Bone marrow | Suppression |
Prognosis by number of organ failures:
- 2 organ failures: 27% in-hospital mortality
- 3 organ failures: 65% in-hospital mortality
- 4 organ failures: 97% in-hospital mortality
Precipitants: Alcohol-associated hepatitis, bacterial infection, HBV reactivation, GI bleeding.
Management: Multidisciplinary ICU-based team; treat the precipitant (corticosteroids for alcoholic hepatitis, antivirals for HBV); organ support; early listing for liver transplant (most effective intervention).
Key Drugs to Avoid in Decompensated Liver Disease
- ACE inhibitors / ARBs - impair renal function
- NSAIDs - precipitate HRS
- Protease inhibitor-based HCV regimens - associated with accelerated hepatic decompensation and death
- Obeticholic acid (OCA) - associated with accelerated hepatic decompensation in cirrhotic patients
Coagulopathy Considerations
- Thrombocytopenia and elevated INR are not contraindications to paracentesis
- Platelet count should be >50,000/mm³ before invasive procedures
- For active bleeding: cryoprecipitate (1 unit/10 kg) is preferred over fresh-frozen plasma
Sources: Goldman-Cecil Medicine, p. 1615-1619 | Rosen's Emergency Medicine, p. 2494-2535 | Sleisenger & Fordtran's GI and Liver Disease, p. 3483-3512 | Miller's Anesthesia, 10e | Yamada's Textbook of Gastroenterology, 7e
This is a shared conversation. Sign in to Orris to start your own chat.