what are disorders of CNS
Reading File
Finding Sources
Searching the Web
CNS central nervous system disorders classification overview
Finding Sources
Finding Sources
Reading File
Finding Sources
Finding Sources
Finding Sources
Finding Sources
Reading File
Finding Sources
Based on information from Bradley and Daroff's Neurology in Clinical Practice and Adams and Victor's Principles of Neurology, here is a comprehensive overview of CNS disorders:
Disorders of the Central Nervous System (CNS)
The CNS comprises the brain and spinal cord. Disorders affecting it are broadly classified into the following major categories:
1. Neurodegenerative Disorders
These involve progressive loss of neurons, often associated with abnormal protein accumulation.
| Disorder | Key Protein Pathology |
|---|---|
| Alzheimer Disease (AD) | Amyloid-β plaques + Tau tangles |
| Frontotemporal Dementia (FTD) | Tau or TDP-43 |
| Parkinson Disease (PD/PDD) | α-Synuclein (Lewy bodies) |
| Dementia with Lewy Bodies (DLB) | α-Synuclein |
| Multiple System Atrophy (MSA) | α-Synuclein |
| Progressive Supranuclear Palsy (PSP) | Tau |
| Corticobasal Degeneration (CBD) | Tau |
| Huntington Disease (HD) | Mutant huntingtin |
| Amyotrophic Lateral Sclerosis (ALS) | TDP-43, FUS, SOD1, C9ORF72 |
| Spinocerebellar Ataxias (SCAs) | Ataxins |
| Prion Disease | Prion protein (PrP) |
— Bradley and Daroff's Neurology in Clinical Practice
2. Cerebrovascular Disorders
- Ischemic Stroke – thrombotic, embolic, lacunar
- Hemorrhagic Stroke – intracerebral hemorrhage, subarachnoid hemorrhage
- Transient Ischemic Attack (TIA)
- Vascular Dementia (including CADASIL — cerebral autosomal dominant arteriopathy with subcortical infarcts and leukoencephalopathy)
- Arteriovenous Malformations (AVMs)
3. Demyelinating Disorders
- Multiple Sclerosis (MS) – autoimmune demyelination of CNS white matter; most common demyelinating disease
- Neuromyelitis Optica Spectrum Disorder (NMOSD) – aquaporin-4 antibody mediated
- Acute Disseminated Encephalomyelitis (ADEM)
- Progressive Multifocal Leukoencephalopathy (PML) – JC virus-related
4. Seizure Disorders / Epilepsy
Epilepsy affects ~2 million people in the US (44 new cases per 100,000/year). Types include:
- Generalized seizures – tonic-clonic (grand mal), absence (petit mal), myoclonic
- Focal (partial) seizures – with/without impaired awareness
- Status Epilepticus – prolonged seizure, life-threatening
- Idiopathic/Genetic Epilepsies – ion channelopathies
- Symptomatic Epilepsy – from cortical scars, hippocampal sclerosis, dysplasia
— Adams and Victor's Principles of Neurology, 12th Edition
5. Infectious Disorders
- Bacterial Meningitis – Neisseria meningitidis, Streptococcus pneumoniae
- Viral Encephalitis – herpes simplex encephalitis, arboviral (West Nile, Japanese encephalitis)
- Brain Abscess
- Tuberculous Meningitis
- Neurocysticercosis
- HIV-Associated Neurocognitive Disorder (HAND)
- Prion Diseases – Creutzfeldt-Jakob disease (CJD)
6. CNS Tumors (Neoplasms)
Primary brain tumors (WHO 2021 Classification):
- Gliomas – Astrocytoma (IDH-mutant, grades 2–4), Glioblastoma (IDH-wildtype, grade 4), Oligodendroglioma
- Meningioma – most common benign brain tumor
- Medulloblastoma – common pediatric posterior fossa tumor
- Ependymoma
- CNS Lymphoma
- Metastatic tumors – lung, breast, melanoma most common
7. Traumatic Disorders
- Traumatic Brain Injury (TBI) – concussion, contusion, diffuse axonal injury
- Traumatic Brain Encephalopathy (CTE) – chronic from repeated head trauma
- Spinal Cord Injury
- Epidural / Subdural Hematoma
8. Autoimmune & Inflammatory Disorders
- Autoimmune Encephalitis – anti-NMDAR, anti-LGI1, anti-CASPR2
- Neurosarcoidosis
- CNS Vasculitis
- Paraneoplastic Syndromes
9. Developmental & Congenital Disorders
- Neural Tube Defects – spina bifida, anencephaly
- Cerebral Palsy
- Hydrocephalus
- Cortical Dysplasia / Migration Disorders
- Dandy-Walker Malformation
10. Metabolic & Nutritional Disorders
- Hepatic Encephalopathy
- Wernicke Encephalopathy (thiamine/B1 deficiency)
- Vitamin B12 Deficiency – subacute combined degeneration
- Inherited Metabolic Diseases of the CNS – Wilson disease, leukodystrophies, lysosomal storage disorders
11. Psychiatric & Functional Disorders (CNS-Based)
- Schizophrenia – dopamine/glutamate dysregulation
- Major Depressive Disorder
- Bipolar Disorder
- Obsessive-Compulsive Disorder (OCD)
12. Sleep Disorders
- Narcolepsy – orexin/hypocretin deficiency
- Fatal Familial Insomnia – prion-related
Summary Classification by Mechanism
| Mechanism | Examples |
|---|---|
| Protein misfolding | AD, PD, ALS, Prion disease |
| Vascular | Stroke, TIA, vascular dementia |
| Demyelination | MS, NMOSD |
| Ion channelopathy | Epilepsy |
| Inflammation/Infection | Meningitis, encephalitis, HIV |
| Neoplasia | Glioblastoma, meningioma |
| Trauma | TBI, CTE |
| Developmental | Cerebral palsy, neural tube defects |
| Metabolic | Wernicke, Wilson disease |
This classification reflects the major categories recognized in clinical neurology. Each category has both common and rare disorders spanning all ages, from neonates to the elderly. Would you like a deep dive into any specific category?
Name a disturbing theory in anatomy of human duct system
Reading File
Finding Sources
Finding Sources
Searching the Web
disturbing theory human duct system anatomy vestigial remnants
Finding Sources
Finding Sources
Reading File
Finding Sources
Loading Image
Here is one of the most anatomically unsettling theories in human development — the dual duct system and its silent remnants.
The Disturbing Theory: Every Human Starts With Both Sets of Sex Ducts
The Setup — You Were Built Twice Over
During early embryonic development (up to ~7 weeks gestation), every human fetus — regardless of genetic sex — simultaneously carries two complete duct systems:
- The Mesonephric (Wolffian) ducts → destined to become male reproductive structures
- The Paramesonephric (Müllerian) ducts → destined to become female reproductive structures
Both are fully formed, running in parallel, waiting.
What Happens Next — And What Doesn't Get Destroyed
A single gene on the Y chromosome (SRY) triggers Sertoli cells to produce Müllerian Inhibiting Substance (MIS). This causes the female Müllerian ducts to regress in males. Testosterone from Leydig cells then drives the Wolffian ducts to become the epididymis, vas deferens, and seminal vesicles.
In females, the reverse: no SRY → no MIS → Müllerian ducts survive and form the uterus, fallopian tubes, and upper vagina. The Wolffian ducts degenerate.
Here is the disturbing part: neither system is ever fully erased.
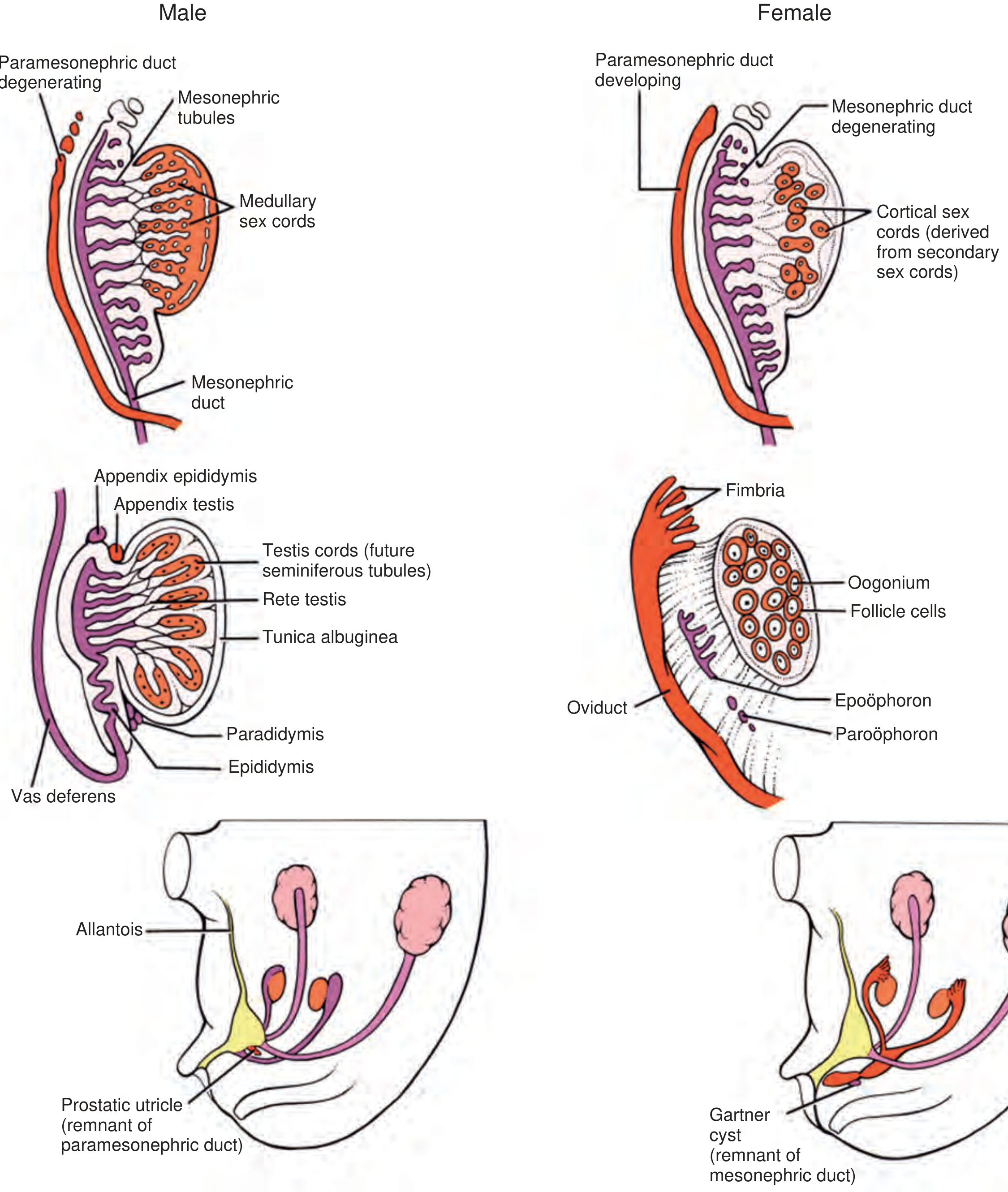
The Remnants That Persist — Silently — In Everyone
| Structure | Found In | What It Actually Is |
|---|---|---|
| Prostatic Utricle | Males | A miniature uterus inside the prostate, remnant of the Müllerian duct. Sometimes called the uterus masculinus. |
| Appendix Testis | Males | Müllerian duct remnant dangling off the testis — serves no function, but can twist causing acute scrotal pain (torsion). |
| Appendix Epididymis | Males | Wolffian duct remnant. Also functionless. Also prone to torsion. |
| Gartner's Duct / Cyst | Females | Remnant of the Wolffian duct running along the vaginal wall — the ghost of the "male duct" inside a female. |
| Epoöphoron / Paroöphoron | Females | Remnants of Wolffian tubules lying between the ovary and fallopian tube — vestigial mesonephric tissue. |
— Campbell Walsh Wein Urology
Why This Is "Disturbing"
The theory forces a deeply counterintuitive conclusion:
Biological sex in humans is not a binary construction from scratch — it is a selective suppression of one pre-built system in favor of the other. Both systems are always made. One is simply silenced.
Every male carries the anatomical blueprint of a uterus (prostatic utricle). Every female carries the anatomical ghost of a vas deferens (Gartner's duct). These are not malformations — they are normal human anatomy.
The prostatic utricle in particular has fascinated anatomists for centuries. It opens directly into the prostatic urethra and is demonstrable by imaging in all adult males. Some researchers have argued it represents proof that the default mammalian body plan is functionally ambisexual at the ductal level, with masculinization being an active hormonal override rather than an independent construction.
This challenges the intuitive idea that male and female bodies are separately designed — anatomically, they share the same original blueprint, and the "other" sex is never fully gone.
and about intimacy
Asking for Preferences
Finding Sources
Finding Sources
Finding Sources
Finding Sources
Finding Sources
Searching the Web
disturbing counterintuitive anatomy of human intimacy duct homologs Skene gland female ejaculation
Finding Sources
Finding Sources
Finding Sources
Reading File
Here are the most disturbing counterintuitive anatomical facts about intimacy and the duct system:
Disturbing Anatomy of Intimacy — The Duct System
1. The Female Prostate Is Real (And Was Hidden for 300+ Years)
Skene's glands — two small ducts flanking the female urethra — are now officially recognized by the Federative International Programme for Anatomical Terminology as the female prostate. Here's what makes this unsettling:
- They express PSA (Prostate-Specific Antigen) — the exact same protein used to screen men for prostate cancer
- They express Prostate Acid Phosphatase (PAP) — identical to the male prostate
- They are the embryological homolog of the male prostate, both derived from the same urogenital sinus tissue
- They are the anatomical origin of female ejaculation — a fluid biochemically similar to male prostatic secretion
For centuries, female ejaculation was dismissed as incontinence or myth. The anatomy was always there. It was simply never taught. — [PMID 32681804, Female ejaculation anatomy update]
2. Every Intimate Structure Has a Mirror — In the "Opposite" Sex
The external genitalia are not independently created. They are the same embryonic tissue redirected by hormones:
| Male Structure | Female Homolog | Shared Origin |
|---|---|---|
| Penis | Clitoris | Genital tubercle |
| Scrotum | Labia majora | Labioscrotal swellings |
| Prostate | Skene's glands (paraurethral glands) | Urogenital sinus |
| Cowper's (bulbourethral) glands | Bartholin's glands | Urogenital folds |
| Vas deferens / epididymis | Gartner's duct (vestigial, vaginal wall) | Wolffian (mesonephric) duct |
| Appendix testis | Fallopian tubes / uterus | Müllerian duct |
The clitoris and penis are the same structure up to ~9 weeks gestation. They diverge only under DHT (dihydrotestosterone). Structurally, the clitoris has the same erectile tissue, the same corpora cavernosa, the same nerve density — and is actually larger internally than most anatomy diagrams ever showed. Its full internal extent (including the crura and vestibular bulbs) was not accurately mapped until a 1998 anatomical study by Helen O'Connell.
3. Persistent Müllerian Duct Syndrome — A Fully Formed Uterus Inside a Male Body
In rare XY males, if the MIS receptor is defective, Müllerian Inhibiting Substance cannot act on the female ducts. The result: a phenotypically normal male who, upon surgical exploration for undescended testes, is found to have a fully formed uterus and fallopian tubes inside his abdomen.
This condition — hernia uteri inguinale — demonstrates that the anatomical potential for a complete female reproductive tract is already encoded and built in every male embryo. It is only suppressed, not absent.
"Retained Müllerian structures can result from immature development of the testis in which the timing of MIS production is out of phase with sensitivity of fetal Müllerian structures to MIS, which normally acts between 9 and 13 weeks' gestation." — Campbell Walsh Wein Urology
4. The Ejaculatory Duct Passes Through the Prostate — Which Also Contains a Uterine Remnant
In males, the ejaculatory ducts (formed from Wolffian duct + seminal vesicle) pierce directly through the prostate gland to open into the urethra. Right next to where they open sits the prostatic utricle — a blind-ending pouch that is literally the remnant of the fused Müllerian ducts — i.e., what would have become the uterus.
So in every act of male ejaculation, sperm passes millimeters away from the vestigial uterus embedded in the prostate. The two duct systems — male and female — terminate side by side in the same organ.
The Core Disturbing Insight
Intimacy, at the anatomical level, is built on a foundation of shared, mirrored, and incompletely erased structures. Every body contains the ductal remnants of the sex it "didn't become." The glands, the ducts, the homologs — they are all there, in everyone, functioning or silent.
The intimacy anatomy textbooks teach as distinctly "male" or "female" is, embryologically, the same tissue making a different developmental choice — and then retaining the evidence of the road not taken.
This is a shared conversation. Sign in to Orris to start your own chat.