Indications for LTOT in ILD
Reading File
Finding Sources
Finding Sources
Searching PubMed
"interstitial lung disease" AND "long-term oxygen therapy"
Reading File
Finding Sources
Finding Sources
Reading File
Finding Sources
Reading File
Finding Sources
Reading File
I now have all the information needed for a comprehensive, well-cited answer. Let me compile it.
Indications for LTOT in ILD
Long-term oxygen therapy (LTOT) in ILD follows the same physiologic thresholds established for COPD (since ILD-specific RCT evidence is still limited), but with ILD-specific considerations given the common pattern of exertional desaturation and progressive hypoxemia.
1. Resting Hypoxemia (Absolute Indication)
| PaO2 | SpO2/SaO2 | Indication |
|---|---|---|
| < 55 mmHg | ≤ 88% at rest | Absolute - LTOT ≥15 h/day |
| 55-59 mmHg | ~89% | Relative - if any qualifier present |
Qualifiers for the 55-59 mmHg group (relative indication):
- Dependent edema (signs of cor pulmonale / right heart failure)
- Polycythemia (hematocrit > 55%)
- P pulmonale on ECG (P wave > 3 mm in leads II, III, or aVF)
(From Fishman's Pulmonary Diseases and Disorders, Table 143-4; based on the ATS Clinical Practice Guideline 2020)
2. Exertional/Exercise-Induced Hypoxemia
ILD patients commonly develop worsening oxygenation with exercise - unlike COPD patients where PaO2 changes unpredictably. Fishman's notes:
"Portable oxygen tanks and battery-powered portable oxygen concentrators are often prescribed for ILD patients with exertional hypoxemia to encourage mobility."
-
Indication: SpO2 ≤ 88% (or PaO2 ≤ 55 mmHg) during exercise/ambulation, even if resting SpO2 is preserved
-
Assessment: formal 6-minute walk test (6MWT) with oximetry, or simple hallway ambulation oximetry
-
Use: ambulatory (portable) oxygen prescribed specifically for activity
-
Fishman's Pulmonary Diseases and Disorders, p. 917
3. Nocturnal Hypoxemia
- Isolated nocturnal desaturation (SpO2 < 88% during sleep) can occur in ILD patients
- Evidence for benefit in this setting is less well-established than for resting hypoxemia
- Fishman's notes: "clinical judgment should be exercised before instituting such therapy" for isolated nocturnal desaturation
- Often assessed with overnight pulse oximetry, especially in patients with co-existing OSA (prevalence is high in ILD/IPF even without classic risk factors)
4. ILD-Specific Considerations
| Feature | Clinical Relevance |
|---|---|
| Mechanism of hypoxemia | V/Q mismatch + impaired diffusion (reduced DLCO) + alveolar destruction - responds well to supplemental O2 |
| Exertional desaturation is near-universal | Even patients with near-normal resting SpO2 may desaturate severely on exertion |
| Pulmonary hypertension | Group 3 PH develops in ILD from chronic hypoxia; LTOT may slow PH progression |
| Threshold target | Maintain SpO2 ≥ 90% (with some guidelines targeting ≥ 92%) |
| Duration | ≥ 15 hours/day for resting hypoxemia (continuous); ambulatory O2 for exertional hypoxemia |
| LOTT trial | The 2016 LOTT trial enrolled mainly COPD patients with moderate resting desaturation (89-93%) or exertional desaturation and found no survival benefit - relevance to ILD is uncertain; ILD-specific RCTs are ongoing |
5. Air Travel
ILD patients are at increased risk of hypoxemia at altitude. The ATS recommends supplemental O2 during air travel if:
-
Resting SpO2 is 92-95% with additional risk factors (ILD is itself a risk factor)
-
Resting SpO2 is < 92% (supplemental O2 recommended regardless)
-
Fishman's Pulmonary Diseases and Disorders, p. 1269
Summary Table
| Situation | Threshold | LTOT Indication |
|---|---|---|
| Resting hypoxemia | PaO2 < 55 mmHg / SpO2 ≤ 88% | Absolute (≥15 h/day) |
| Resting + cor pulmonale signs | PaO2 55-59 mmHg / SpO2 ~89% | Relative (≥15 h/day) |
| Exertional desaturation | SpO2 ≤ 88% on 6MWT or walking | Ambulatory/portable O2 |
| Nocturnal desaturation | SpO2 < 88% on overnight oximetry | Clinical judgment; oxygen during sleep |
| Air travel | SpO2 < 92% or 92-95% + ILD risk | In-flight supplemental O2 |
Key caveat: The established LTOT criteria were derived primarily from COPD trials (MRC and NOTT trials). The ATS 2020 guideline applies them broadly to "adults with chronic lung disease," including ILD. However, Fishman's notes that "future randomized controlled trials assessing the impact of oxygen therapy in fibrotic ILD patients are underway," meaning the survival benefit seen in COPD has not been definitively replicated in ILD. The primary current rationale in ILD is prevention of PH progression, maintenance of mobility, and symptom relief.
Proximal LAD ECG criteria
Finding Sources
Finding Sources
Finding Sources
Finding Sources
Finding Sources
Reading File
Reading File
Reading File
Reading File
Reading File
Reading File
Loading Image
Loading Image
I now have all the content and images needed for a complete, well-organized answer.
ECG Criteria for Proximal LAD Occlusion
Proximal LAD occlusion produces several distinct ECG patterns depending on whether it is an acute total occlusion (STEMI or STEMI-equivalent) or a high-grade subtotal stenosis (pre-infarction warning patterns). Recognizing all patterns is critical because some are STEMI-equivalents requiring immediate reperfusion.
1. Classic Anterior STEMI (Acute Occlusion)
The baseline pattern with acute proximal LAD occlusion:
| Leads | Finding |
|---|---|
| V1-V4 | ST elevation (primary) |
| I, aVL | ST elevation if occlusion is proximal to D1 (anterolateral extension) |
| V5-V6 | ST elevation may extend if large LAD territory |
| II, III, aVF | Reciprocal ST depression |
| aVR | May show ST elevation |
-
ST elevation is typically obliquely straight or convex morphology
-
The more proximal the occlusion, the more leads are involved (V1-V6 + I + aVL = proximal; V3-V5 only = more distal)
-
Rosen's Emergency Medicine, Fig. 64.6/64.7
2. aVR ST Elevation - Proximal LAD vs. Left Main
A key distinguishing feature for proximal LAD occlusion:
"If ST segment elevation occurs in leads aVR and V1, greater elevation in aVR favors left main disease, whereas greater elevation in V1 favors left anterior descending occlusion."
| aVR STE pattern | Likely culprit |
|---|---|
| STE in aVR > STE in V1 | Left main |
| STE in aVR < STE in V1, + widespread precordial changes | Proximal LAD |
| STE in aVR (>0.5 mV) + widespread ST depression elsewhere | Left main OR proximal LAD (sensitivity 78%, specificity 83%) |
The de Winter pattern (see below) also features STE in aVR.
- Rosen's Emergency Medicine, p. 1004
3. Wellens Syndrome (Pre-infarction / Critical Stenosis Warning)
Wellens syndrome represents reperfusion after transient occlusion of the proximal LAD - a critical stenosis that will progress to anterior STEMI without intervention.
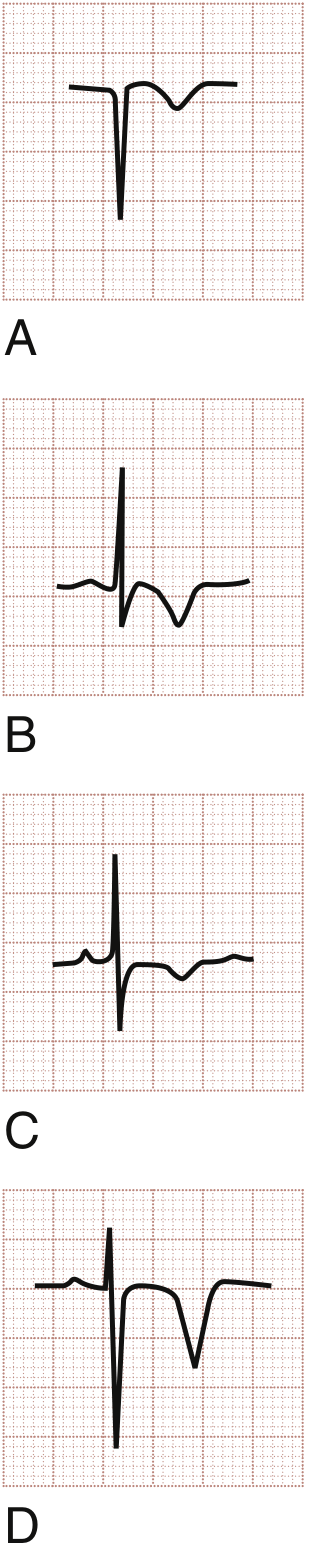
T-wave patterns: (A) T-wave inversion in ACS, (B/C) T-wave inversions in NSTEMI, (D) Deep symmetric T-wave inversion - Wellens syndrome (proximal LAD stenosis)
Criteria (from Tintinalli's Table 49-7):
| Criterion | Detail |
|---|---|
| Clinical context | History of episodic chest pain (unstable angina) |
| Timing | Abnormal T waves appear when pain free (not during pain) |
| Leads affected | Most prominent V2-V3; often V1-V3; occasionally V4-V6 |
| Type A (75%) | Deep symmetric T-wave inversion (>5 mm) |
| Type B (25%) | Biphasic T waves (positive-negative deflection) |
| Q waves | Absent - no pathologic Q waves or loss of R wave |
| ST segment | Isoelectric or minimally elevated (<1 mm) |
| Biomarkers | Normal or minimally elevated |
Key teaching point: During active pain the ECG may look normal or show only subtle changes. The dramatic T-wave pattern appears in the pain-free state. About 15% of unstable angina presentations show Wellens sign. Natural history = progression to anterior STEMI if untreated.
- Tintinalli's Emergency Medicine, Table 49-7; Rosen's Emergency Medicine, p. 1001
4. de Winter Pattern (STEMI-Equivalent)
The de Winter pattern is a STEMI-equivalent associated with acute proximal LAD occlusion, occurring in ~2% of anterior STEMIs. Unlike classic STEMI, the ECG does not show ST elevation in precordial leads.
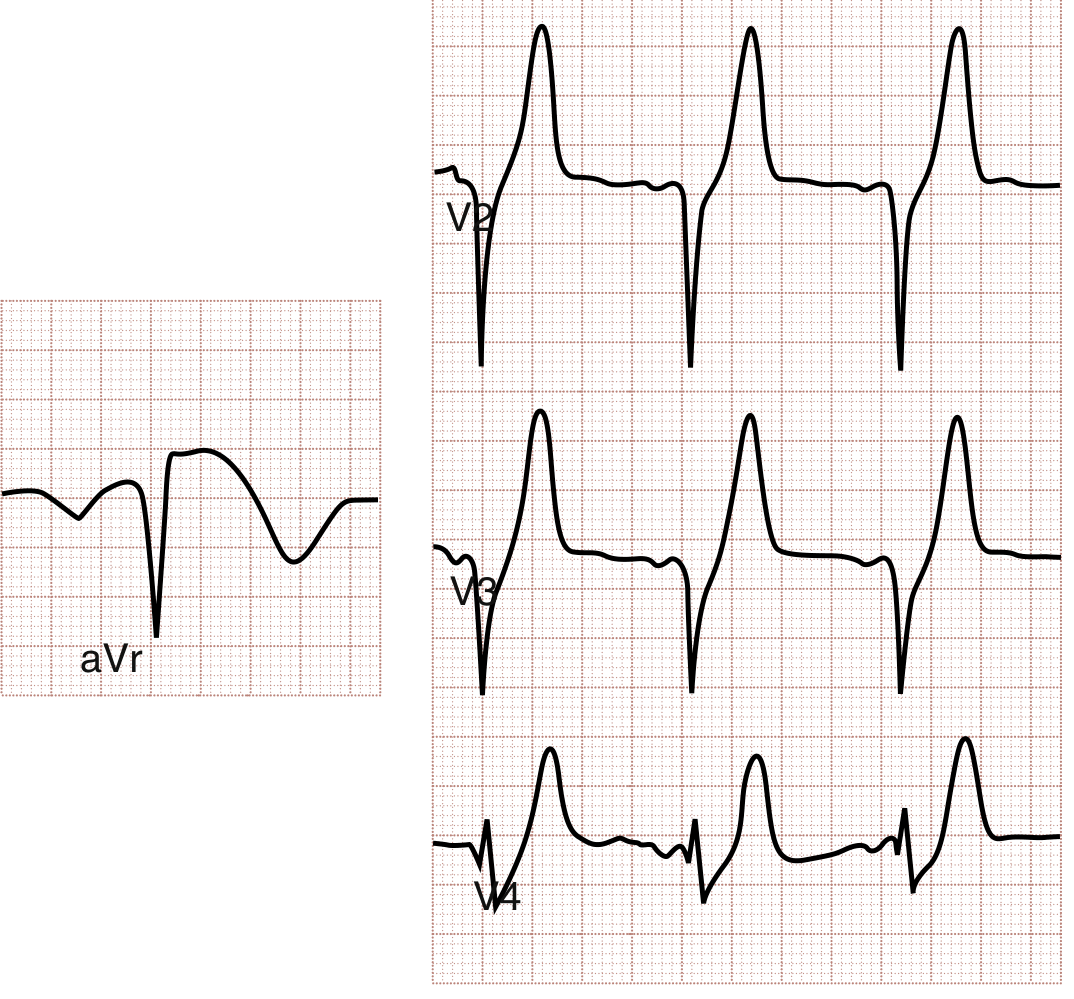
de Winter pattern: aVR shows ST elevation (left panel); V2-V4 show J-point depression with upsloping ST depression and tall symmetric T waves (right panel)
Criteria:
| Finding | Detail |
|---|---|
| Precordial leads (V1-V6) | J-point depression (1-3 mm) with upsloping ST depression |
| T waves | Tall, prominent, symmetric (hyperacute T waves) |
| aVR | ST elevation |
| Clinical appearance | Patient usually ill-appearing with ongoing chest pain |
| Progression | May evolve to classic anterior STEMI, or produce large MI without classic evolution |
Management: Treat as STEMI-equivalent - immediate reperfusion (cath lab activation).
- Rosen's Emergency Medicine, p. 1004; Tintinalli's Emergency Medicine, p. 381
5. Summary: Lead Pattern by Occlusion Site
| ECG Pattern | Occlusion Level | Key Leads |
|---|---|---|
| STE V1-V6 + I + aVL | Proximal LAD (before D1 and septal perforators) | V1-V6, I, aVL |
| STE V1-V4 only | LAD (after D1) | V1-V4 |
| Wellens (Type A/B) | Proximal LAD critical stenosis (subtotal, reperfused) | V2-V3 T-wave changes |
| de Winter pattern | Proximal LAD acute occlusion (STEMI-equivalent) | J-point depression + tall T in V1-V4; STE in aVR |
| STE aVR > V1 + diffuse STD | Left main or proximal LAD + multivessel | aVR, diffuse |
Clinical Pearls
- RBBB + anterior STE: New right bundle branch block with anterior ST elevation suggests proximal LAD occlusion with septal involvement - poor prognostic sign.
- Reciprocal changes: ST depression in II, III, aVF is a reciprocal change supporting anterior STEMI from proximal LAD.
- High lateral involvement (I, aVL STE): Indicates the occlusion is proximal to the first diagonal branch (D1). Isolated high lateral STE without anterior changes points more to the diagonal or circumflex.
- Wellens ≠ safe: These patients must NOT be stress tested (can precipitate complete occlusion). They need urgent angiography.
- de Winter = cath lab now: Static pattern that does not evolve to STE - do not wait for "classic" changes.
This is a shared conversation. Sign in to Orris to start your own chat.