AI in General surgery long Question 30 marks with images
Asking for Preferences
Reading File
Finding Sources
Searching PubMed
artificial intelligence general surgery
Searching the Web
AI in general surgery 2025 robotic imaging diagnosis outcomes review
Reading File
Searching PubMed
AI robotic surgery laparoscopy outcomes
Reading Web Page
AI in general surgery diagnosis imaging robotics outcomes
Reading File
Loading Image
Loading Image
Reading File
Loading Image
Loading Image
Reading File
Searching PubMed
AI machine learning surgical risk prediction postoperative complications
Reading File
Loading Image
I now have comprehensive material from the textbook and recent literature to compose a thorough 30-mark exam answer. Let me write it up.
Artificial Intelligence in General Surgery
Exam Question (30 Marks):
"Discuss the role of Artificial Intelligence in General Surgery, covering its applications in preoperative planning, intraoperative guidance, robotics, endoscopy, radiology, surgical training, and postoperative care. Include the ethical and regulatory challenges associated with its implementation."
Model Answer
1. Introduction and Foundational Concepts (3 marks)
Artificial intelligence (AI) refers to the simulation of human cognitive functions - learning, reasoning, and problem-solving - by computational systems. In medicine, AI exists across a spectrum of technologies:
- Machine Learning (ML): Algorithms that improve through experience by analyzing training datasets, without being explicitly programmed for each task.
- Deep Learning (DL): A subset of ML using multi-layered artificial neural networks (ANNs) capable of recognizing complex patterns in large datasets.
- Computer Vision (CV): AI interpretation of visual information - central to surgical video analysis.
- Natural Language Processing (NLP): AI processing of written/spoken text, used in automated clinical notes and referral triage.
AI is applicable across all phases of surgical care: preoperative, intraoperative, and postoperative. The specialties at the forefront of AI adoption are those that are already digitalized or heavily data-driven.
2. Preoperative Applications (5 marks)
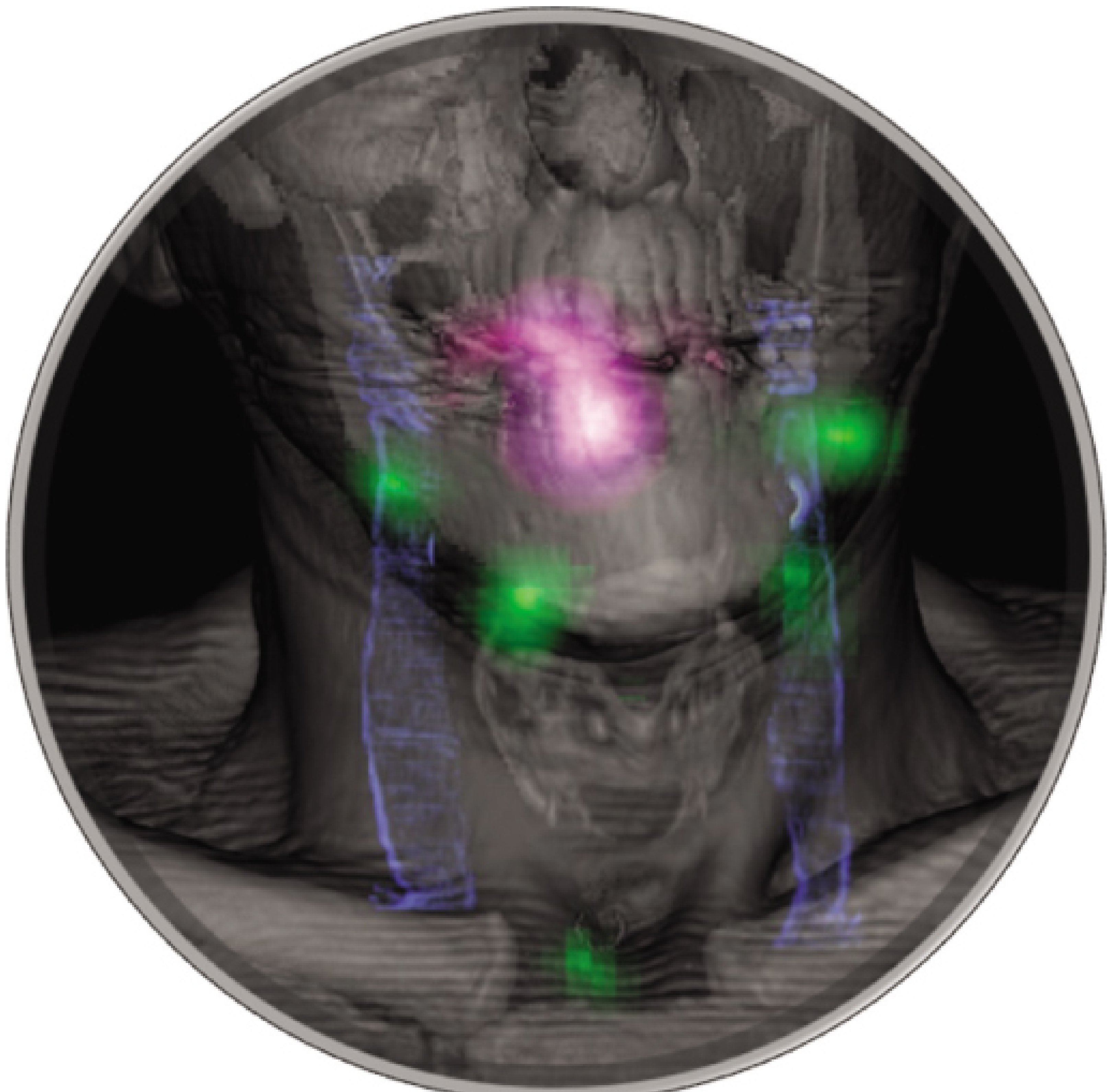
2a. Diagnostic Imaging and 3D Reconstruction
As surgery becomes increasingly complex and moves toward minimally invasive techniques, full understanding of surgical anatomy prior to operation is essential. AI enables the processing of CT/MRI scans - which may contain dozens of individual cross-sectional images - to generate 3-dimensional anatomical reconstructions in hours rather than days.
- FDA-approved tools include Visible Patient (Strasbourg, France) and Oxirix MD (Pixmeo SARL, Geneva).
- 3D printing of AI-reconstructed models is used in colorectal surgery (anal fistula anatomy), vascular surgery (endovascular planning), and orthopedic trauma (fracture fixation).
- These models enhance multidisciplinary team discussions and surgical training.
2b. Risk Stratification
AI-based preoperative risk tools analyze patient demographics, comorbidities, imaging, and laboratory data to predict mortality and postoperative complication rates. This enables personalized perioperative planning and allows surgeons to identify which patients require optimization before surgery. Systematic reviews confirm that ML models for surgical site infection and general postoperative complications outperform traditional scoring systems such as the P-POSSUM (PMID: 39666725).
2c. Pathology and NLP
AI-enhanced digital pathology allows automated cell counting and tumor classification. NLP automates the screening and prioritization of outpatient referrals, reducing administrative burden and improving workflow in surgical departments.
3. Intraoperative Applications (6 marks)
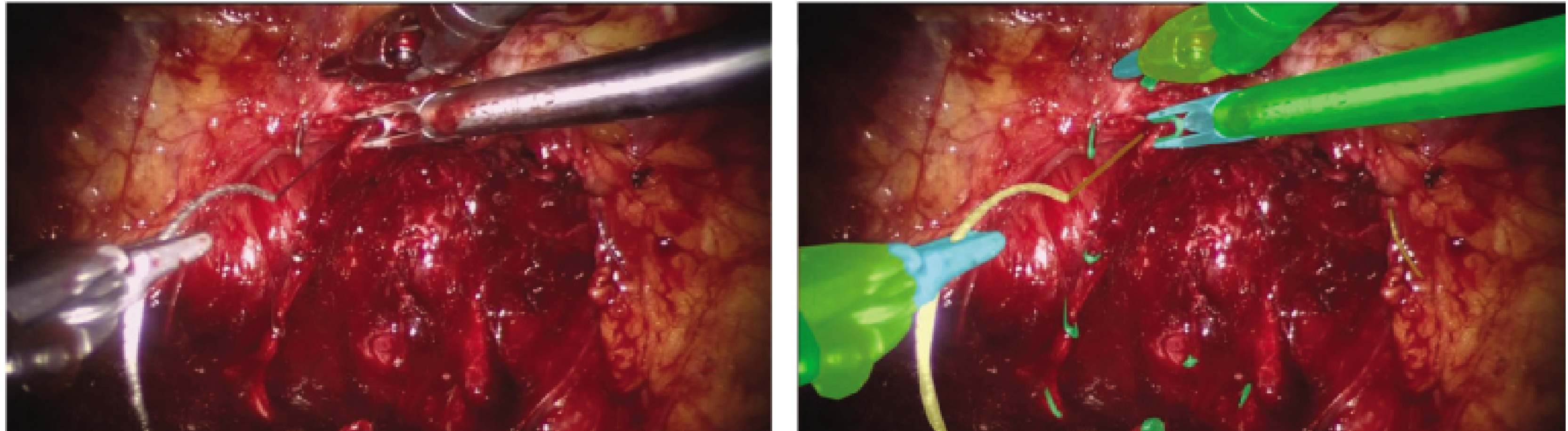
3a. Anatomical Identification and Safety
Computer vision combined with surgical video analysis allows AI systems to identify anatomical structures in real time during minimally invasive procedures. The most studied application is laparoscopic cholecystectomy, where bile duct injury remains a serious complication of a technically routine procedure. AI-driven object detection systems trained on video datasets can identify the cystic duct, common bile duct, and the critical view of safety in real time.
Future systems may allow a surgeon to highlight an unclear anatomical area on screen, with AI identifying the structures within it.
3b. Surgical Phase Recognition
ML algorithms recognize defined stages of an operation (e.g., completion of pneumoperitoneum, clipping of the cystic duct). Phase recognition:
- Enables automatic display of reference materials at the appropriate operative stage.
- Ensures instrument preparedness and improves operating theatre efficiency.
- Forms the foundation for semi-autonomous and ultimately fully autonomous robotic surgery.
- Systems performing sutured bowel anastomosis in animal models have already been demonstrated.
3c. Intraoperative Decision Support
AI can provide information not directly available through the limitations of a laparoscopic view:
- Hyperspectral imaging: Measures blood flow and oxygenation at the tissue level in real time, enabling perfusion assessment to guide bowel resection margins.
- Optical biopsy (probe confocal laser endomicroscopy - pCLE): AI-assisted tissue classification that may identify tumor margins intraoperatively, improving lymph node yield and reducing positive resection margins.
- Bleeding detection: Real-time AI alerts for vascular injury.
4. Robotic Surgery and AI (5 marks)
The da Vinci Surgical System (Intuitive Surgical Inc., USA) received initial FDA approval in 2000. Robotic-assisted procedures have increased annually across all surgical specialties. AI is a fundamental component of robotic surgery and enables:
- Robot kinematics: Continuous recording of the position and motion of robotic arms, providing spatial data absent in conventional laparoscopy.
- 3D localization and mapping: Combining CV with robot kinematics to reconstruct the operative field in three dimensions.
- Image overlay (augmented reality): Fusion of preoperative radiologic reconstructions with real-time 3D maps, enabling the robot to display tumor margins from preoperative MRI or limit movement near critical anatomical structures.
A 2026 meta-analysis of robotic vs. laparoscopic cholecystectomy demonstrated comparable complication rates with potential advantages of robotics in non-elective settings (PMID: 41417656). A 2025 systematic review demonstrated validated AI tools for objective assessment of robotic surgical skill (PMID: 37951600).
The ultimate goal is autonomous robotic surgery, where AI systems perform defined surgical tasks without direct human control. This remains investigational but is technically achievable for isolated tasks.
5. AI in Radiology (3 marks)
Medical imaging is ideally suited to AI due to existing large, digitized, labeled datasets. Key applications include:
| Application | Detail |
|---|---|
| Computer-aided detection (CAD) | Lung, colorectal, and breast cancer screening |
| Image segmentation | Automated organ detection, volumetric analysis |
| Liver resection planning | Patient-specific anatomical models |
| Radiotherapy planning | Organ-at-risk delineation (e.g., prostate radiotherapy) |
| Radiation dose optimization | Tailored dose based on patient characteristics and prior exposure |
| Artifact reduction | AI post-processing removes movement artifacts |

Limitations in radiology AI include: non-standardized radiology reports, the large computing power required for real-time analysis, and the ethical issues surrounding large datasets used for model training.
6. AI in Endoscopy (3 marks)
The rate of missed lesions at colonoscopy is approximately 15%. AI in endoscopy centers on:
- CADe (Computer-Aided Detection): Real-time polyp identification during colonoscopy; detection of bleeding lesions in wireless capsule endoscopy. A 2024 meta-analysis (PMID: 39531400) confirmed AI-assisted colonoscopy significantly increases polyp detection rates.
- CADx (Computer-Aided Diagnosis / Optical Biopsy): Real-time classification of polyp histology, potentially avoiding unnecessary polypectomy.
- Quality assurance: AI monitors visualization completeness (e.g., cecal intubation confirmation, adequate bowel preparation assessment).
The American Society of Gastrointestinal Endoscopy (ASGE) has identified priority AI research areas: colonic polyp detection, Barrett's esophagus dysplasia, early gastric cancer, and IBD-related dysplasia.
7. Surgical Training and Performance Analytics (2 marks)
AI enables objective, data-driven assessment of surgical performance:
- C-SATS (USA): Cloud-based system providing AI-assisted qualitative and quantitative feedback across multiple performance domains from uploaded operative videos.
- Touch Surgery Enterprise (Medtronic): Automated post-operative video upload with AI-based surgical phase recognition, enabling personal procedure banks for self-reflection, mentoring, and collaborative research.
- Metric analysis: Range of instrument motion, force applied, time per operative stage, and procedural completion rates.
Robotic surgery is particularly suited to this technology as kinematics and instrument data are already digitized. Systematic review evidence supports AI tools for objective assessment of robotic technical skill (PMID: 37951600).
8. Postoperative Applications (1 mark)
Postoperatively, AI contributes through:
- Predictive models for complications: ML models predicting 30-day readmission, surgical site infection, and anastomotic leak using electronic health record (EHR) data.
- Remote monitoring: Wearable sensor data integrated with AI for early detection of deterioration (sepsis alerts, wound monitoring).
- Natural language processing: Automated coding of operative notes and discharge summaries, reducing administrative workload.
9. Ethical and Regulatory Challenges (2 marks)
Data Privacy and Consent
- AI training requires large volumes of confidential patient data; patients are rarely consented for data inclusion in training sets.
- Risk of systemic bias when ethnic minorities are under-represented in registry datasets.
- High-profile cyberattacks on health systems have eroded public trust.
Accountability and the "Black Box" Problem
- Many deep learning models cannot explain their reasoning (the "black box" problem), making informed consent by patients and accountability by clinicians problematic.
- If an AI system contributes to a clinical decision that causes harm, it is unclear whether the responsible party is the clinician, hospital, or AI manufacturer.
Regulatory Framework
The FDA, Health Canada, and the UK's MHRA have jointly published 10 Guiding Principles for AI/ML in Medical Devices, summarized in Table 1 below:
| Principle | Principle |
|---|---|
| Multidisciplinary expertise across the total product lifecycle | Good software engineering and security practices |
| Representative clinical study participants | Independent training and test datasets |
| Best available reference datasets | Model design tailored to data and intended use |
| Focus on human-AI team performance | Testing under clinically relevant conditions |
| Clear user information | Deployed model monitoring and retraining risk management |
Table 1 - FDA/Health Canada/MHRA 10 Guiding Principles of AI in Medical Devices. (Fischer's Mastery of Surgery, 8th ed., p.829)
The FDA's AI/ML-based Software as a Medical Device (SaMD) action plan adopts a total product lifecycle approach, allowing real-world performance monitoring and safety signal detection post-approval.
Marking Summary
| Section | Marks |
|---|---|
| Introduction - AI types (ML, DL, CV, NLP) | 3 |
| Preoperative: imaging, 3D reconstruction, risk stratification, NLP | 5 |
| Intraoperative: anatomy identification, phase recognition, decision support | 6 |
| Robotics: kinematics, AR overlay, autonomous surgery | 5 |
| Radiology: CAD, segmentation, dose optimization | 3 |
| Endoscopy: CADe, CADx, quality assurance | 3 |
| Surgical training and performance analytics | 2 |
| Postoperative applications | 1 |
| Ethical and regulatory challenges | 2 |
| Total | 30 |
Key References
- Fischer's Mastery of Surgery, 8th Edition - Chapter 24: AI in Surgery, pp. 818-829
- Soleymanjahi S et al. AI-Assisted Colonoscopy for Polyp Detection: Systematic Review and Meta-analysis. Ann Intern Med. 2024 Dec (PMID: 39531400)
- Boal MWE et al. Evaluation of AI in robotic surgery technical skills assessment: systematic review. Br J Surg. 2024 (PMID: 37951600)
- van Boekel AM et al. ML models for postoperative surgical site infection prediction: systematic evaluation. PLoS One. 2024 (PMID: 39666725)
- Camarotti TAF et al. Robotic vs laparoscopic cholecystectomy in non-elective procedures: systematic review and meta-analysis. J Trauma Acute Care Surg. 2026 (PMID: 41417656)
- Negahi A et al. Precision Medicine and AI in Next-Generation Cancer Surgery. Asian Pac J Cancer Prev. 2025 (PMID: 41459844)
Examiner's Tips:
- Always organize the answer by perioperative phase (pre/intra/post) plus robotics, endoscopy, radiology, training, and ethics.
- Include specific examples (laparoscopic cholecystectomy bile duct safety, colonoscopy polyp detection) - these attract marks.
- The ethics section is frequently under-answered: address the black box problem, data consent, bias, and the FDA/MHRA regulatory framework explicitly.
- Use named tools where known: da Vinci System, Visible Patient, C-SATS, Touch Surgery Enterprise, CADe/CADx.
This is a shared conversation. Sign in to Orris to start your own chat.