A 45yr old female keeps getting numbness and pain on and off in her right hand. Also, she gets numbness on and off in her left hand as well. Yesterday she had pain in her right thumb. What could be the reasons and management
Reading File
Finding Sources
Finding Sources
Searching PubMed
"carpal tunnel syndrome" diagnosis management
Reading File
Reading File
Reading File
Finding Sources
Finding Sources
Reading File
Finding Sources
Finding Sources
Loading Image
Loading Image
I now have comprehensive information to provide a thorough clinical response. Here is the full analysis:
Bilateral Hand Numbness & Pain in a 45-Year-Old Female — Differential Diagnosis & Management
Most Likely Diagnosis: Carpal Tunnel Syndrome (CTS)
This presentation — intermittent numbness and pain in both hands (worse on the right), with thumb pain — is classic for bilateral CTS, the most common entrapment neuropathy. It is significantly more frequent in women and peaks in the 40–60 age group.
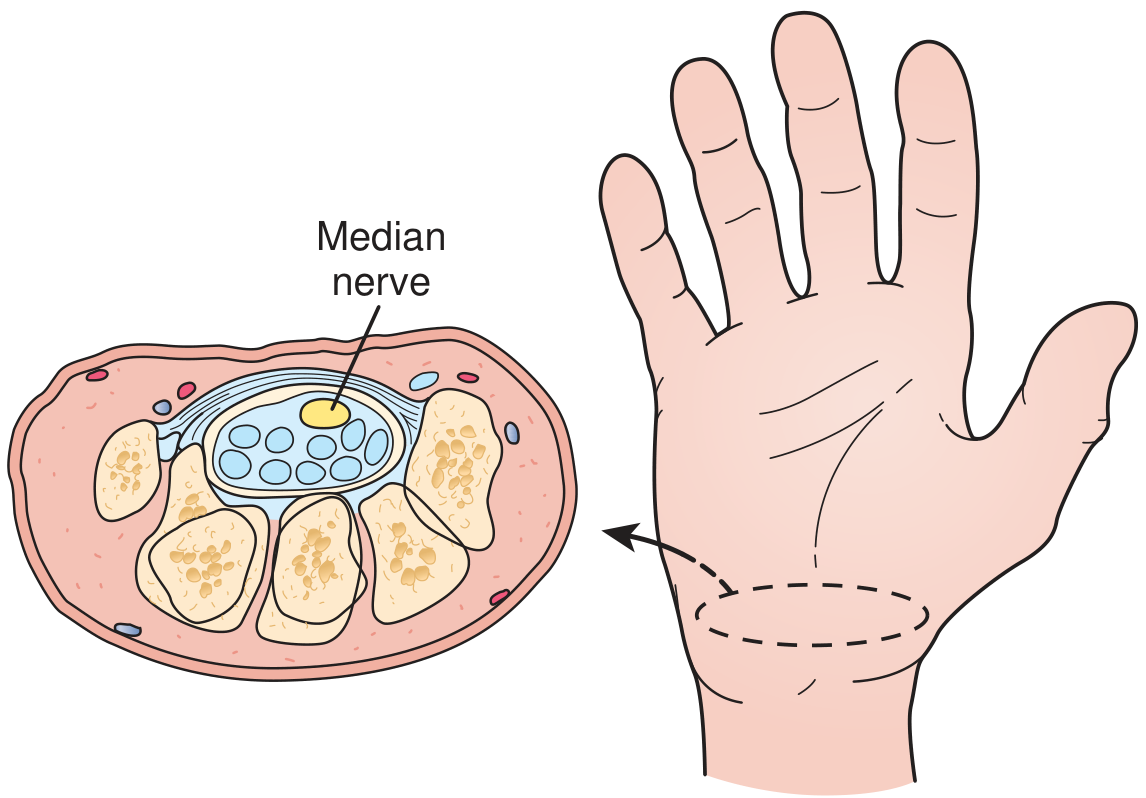
Cross-section of the carpal tunnel: the median nerve and nine flexor tendons pass through a rigid bony-ligamentous canal — any increase in canal pressure compresses the nerve — Textbook of Family Medicine 9e
1. Differential Diagnoses
🔴 Primary (Most Likely)
Carpal Tunnel Syndrome (CTS)
- Mechanism: Compression of the median nerve within the rigid carpal tunnel formed by carpal bones (floor/sides) and the transverse carpal ligament (roof)
- Classic symptoms: Numbness, paresthesia, and pain in the thumb, index, middle, and radial half of the ring finger — exactly matching this patient's right thumb pain
- Symptoms are bilateral in many cases, typically worse at night and after repetitive hand use
- Patients often report being woken at night by pain/tingling, which improves by shaking or hanging the hand down
- May radiate proximally to the forearm and shoulder
- Progressive cases develop decreased grip strength, thenar atrophy, and hand clumsiness
"The classic symptoms include a gradual onset of numbness, paresthesia, and pain in the median nerve distribution (thumb, index, long and radial aspect of the ring finger). These symptoms often are bilateral and are worse during the night and after strenuous activities." — Rosen's Emergency Medicine
Why she is at risk: Middle-aged women are at highest risk. Systemic associations to screen for include:
- Hypothyroidism
- Rheumatoid arthritis
- Diabetes mellitus
- Menopause (hormonal changes)
- Repetitive occupational hand activity
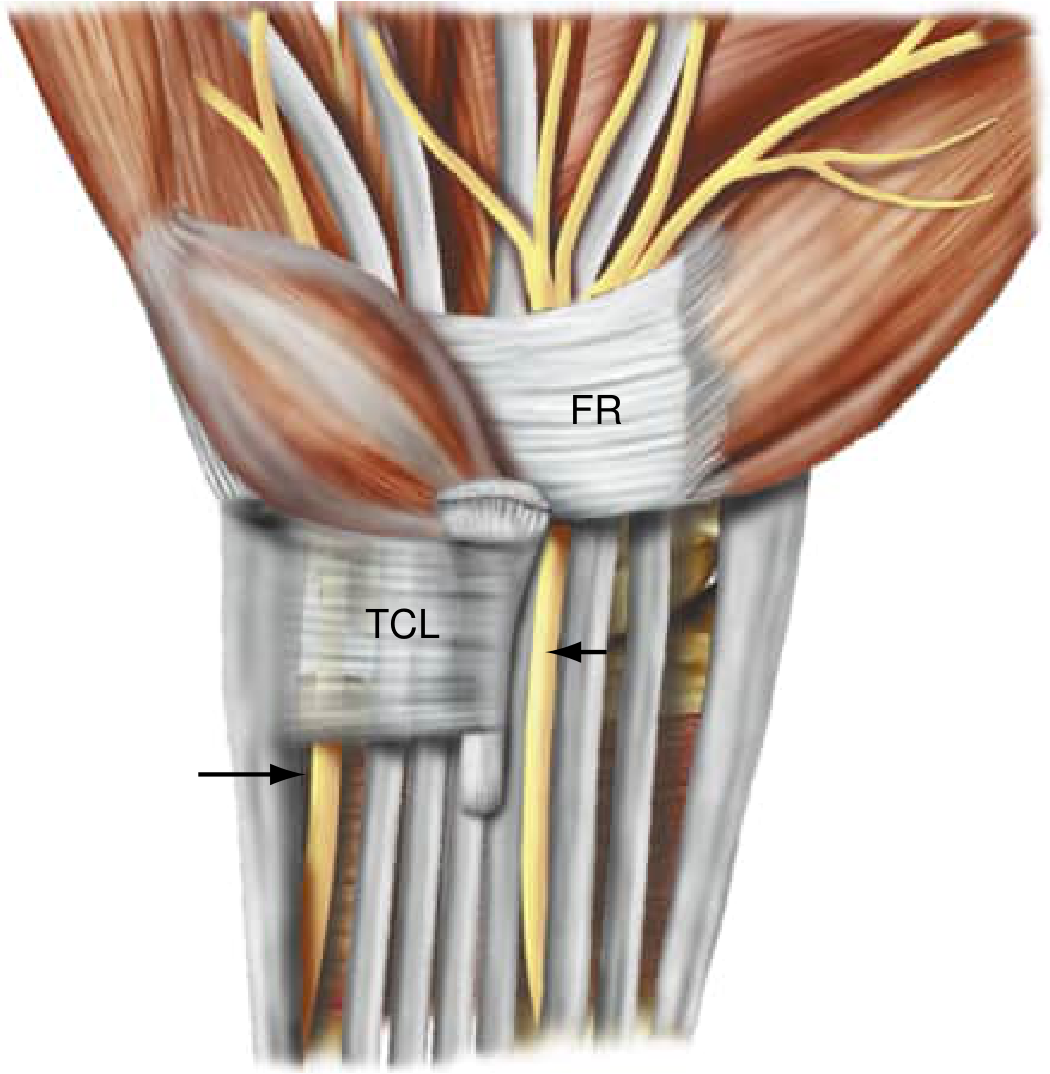
The median nerve enters the carpal canal under the TCL; the palmar cutaneous branch exits proximally, which is why thenar skin sensation is spared in CTS — Bradley and Daroff's Neurology
🟡 Important Differentials
Cervical Radiculopathy (C6–C7)
- Herniated cervical disc at C6 (supplies thumb, index finger) or C7 can mimic CTS precisely
- Bilateral hand numbness is common with cervical disc disease
- Distinguished by: neck pain, symptoms worsened by neck movement, positive Spurling test, reflexes may be reduced
- "Bilateral hand numbness, paresthesia, or similar altered sensation is common [with cervical disc herniation]. Failure to consider a protruded cervical disc in patients with obscure symptoms is a common error." — Adams & Victor's Principles of Neurology
De Quervain's Tenosynovitis
- Specifically explains her right thumb pain
- Involves the abductor pollicis longus and extensor pollicis brevis tendons in the first dorsal compartment at the radial styloid
- Pain radiates proximally up the forearm and distally down the thumb
- Diagnosed by Finkelstein's test (passive ulnar deviation with thumb enclosed in fist = pain over radial styloid)
- Common in middle-aged women, often associated with repetitive pinching/gripping
Thoracic Outlet Syndrome (TOS)
- Compression of the brachial plexus (C8–T1) or subclavian vessels as they pass through the scalene triangle
- Presents with brachialgia, hand numbness/tingling — often bilateral or dominant-side predominant
- Symptoms worsen with arm elevation or overhead activities
- Roos test: arm elevation with repeated hand exercise provokes symptoms
Ulnar Nerve Entrapment (Cubital Tunnel Syndrome)
- Numbness involves the little and ring fingers (ulnar distribution), not the thumb
- Can be distinguished by distribution: CTS = radial 3½ digits; ulnar = ulnar 1½ digits
- Positive Tinel sign at the elbow over the ulnar groove
Peripheral Neuropathy
- Diabetic or other metabolic neuropathies can cause bilateral symmetric hand numbness
- Usually has a "glove-and-stocking" pattern; less episodic
- Thyroid-related neuropathy is another consideration in a 45-year-old woman
Raynaud's Phenomenon
- Episodic vasospasm causing color changes (white → blue → red) + numbness/pain in hands, triggered by cold or stress
- Can coexist with CTS or be a feature of connective tissue disease (lupus, scleroderma)
- Distinguish by characteristic color changes and triggers
2. Clinical Examination
| Test | Positive Finding | Suggests |
|---|---|---|
| Phalen test | Wrist flexion ×60 sec → numbness/tingling in median distribution | CTS (sensitivity ~74%) |
| Tinel sign | Tapping wrist flexor retinaculum → paresthesias in radial digits | CTS |
| Durkan (carpal compression) test | Direct pressure over carpal tunnel → symptoms | CTS (highest sensitivity & specificity) |
| Finkelstein test | Thumb enclosed in fist, ulnar deviation → radial pain | De Quervain's |
| Spurling test | Neck extension + lateral flexion + axial load → arm pain | Cervical radiculopathy |
| Roos test | Arms elevated, repeated hand opening/closing → symptoms | TOS |
| Thumb abduction weakness, thenar atrophy | Abductor pollicis brevis weak/wasted | Advanced CTS |
3. Investigations
| Test | Purpose |
|---|---|
| Nerve conduction studies (NCS) + EMG | Gold standard to confirm CTS; localize entrapment; assess severity. Prolonged distal motor and sensory latencies confirm median nerve compression. Must be done before any surgery. |
| Wrist/hand ultrasound | Measures median nerve cross-sectional area; identifies structural causes (ganglion, synovitis) |
| Cervical spine X-ray / MRI | If cervical radiculopathy suspected (neck pain, bilateral symptoms, reflex changes) |
| Blood tests | FBS/HbA1c (diabetes), TSH (hypothyroidism), RF/anti-CCP (RA), ANA (connective tissue disease), renal function |
| Wrist X-ray | If bony pathology, trauma, or arthritis considered |
4. Management
Conservative (First-Line)
| Intervention | Details |
|---|---|
| Activity modification | Avoid repetitive wrist flexion/extension; ergonomic adjustments (keyboard wrist supports) |
| Wrist splinting | Neutral-position splints worn at night — reduces nocturnal symptoms by preventing wrist flexion. Most effective initial measure. |
| Nerve gliding exercises | Gentle tendon and nerve gliding exercises provide symptom relief and improve nerve mobility |
| NSAIDs | Short-term pain relief; however, studies show no better efficacy than placebo for long-term CTS management |
| Oral corticosteroids | Short course (prednisolone) provides temporary relief but symptoms often recur |
| Local corticosteroid injection | Injection into the carpal tunnel provides good short-to-medium-term relief; better than placebo. Majority of patients experience significant improvement, though recurrence within 1 year is common |
"A majority of patients will experience good relief of symptoms if these conservative measures are followed. Unfortunately, most of these patients will have a return of symptoms in 1 year." — Textbook of Family Medicine 9e
Surgical (When Conservative Fails)
- Carpal tunnel release — dividing the transverse carpal ligament to decompress the median nerve
- Indicated when: symptoms recur despite adequate conservative treatment, motor weakness/thenar atrophy, abnormal NCS
- Both open and endoscopic techniques have equivalent long-term outcomes
- A 2024 meta-analysis (PMID 38768022) confirmed endoscopic vs. open CTR have equivalent outcomes, with endoscopic offering faster recovery
- Newer: Ultrasound-guided nerve hydrodissection — a 2025 systematic review (PMID 39894044) shows this as an effective minimally invasive option
Treat Underlying Causes
- If hypothyroid → thyroid replacement
- If diabetic → optimise glycaemic control
- If RA → disease-modifying therapy
- If menopausal → hormonal considerations
5. Summary Approach for This Patient
45F + bilateral intermittent hand numbness + right thumb pain
↓
Most likely: Bilateral CTS ± De Quervain's (right thumb)
↓
Screen: Phalen, Tinel, Durkan, Finkelstein, Spurling tests
↓
Labs: TSH, FBS, RF, ANA, renal function
NCS/EMG: Confirm CTS, exclude radiculopathy/plexopathy
↓
Start: Night wrist splints + activity modification + nerve gliding
If no improvement at 6–8 weeks: corticosteroid injection
If recurrence or motor signs: surgical carpal tunnel release
Key clinical point: Bilateral CTS in a 45-year-old woman warrants a systematic screen for hypothyroidism and early menopause — both are common in this demographic, frequently overlooked, and directly treatable causes of CTS that resolve with hormonal correction.
Sources: Rosen's Emergency Medicine; Bradley and Daroff's Neurology in Clinical Practice; Textbook of Family Medicine 9e; Adams and Victor's Principles of Neurology 12e; Tintinalli's Emergency Medicine
This is a shared conversation. Sign in to Orris to start your own chat.