PROTEIN IN URINE (PROTEINURIA) Normal Protein Excretion * Normal urinary protein excretion = ≤150 mg/day * Proteins with MW <50,000–60,000 Da pass through GBM and are reabsorbed by proximal tubules * Only very small amount of albumin (MW 69,000 Da) is filtered * Tamm-Horsfall glycoprotein (uromucoid) * Secreted by: * Distal tubular cells * Ascending loop of Henle * Forms ≥1/3 of normal urinary protein ⸻ Proteinuria Definition * Presence of detectable protein in urine * Indicates renal disease, especially glomerular injury * If urine is turbid → filter or centrifuge before testing ⸻ Methods for Detection of Proteinuria 1. Reagent Strip Method 2. Heat & Acetic Acid Test 3. Sulfosalicylic Acid Test 4. Heller’s Test Note * Reagent strip → mainly detects albumin * Acid precipitation methods → detect all proteins ⸻ 1. Reagent Strip Method Principle * Based on protein error of pH indicators * Proteins carry charge at physiologic pH → produce pH change * Color change of indicator indicates presence of protein Reagent * Tetrabromophenol blue OR * Tetrachlorophenol-tetrabromosulfophthalein * Buffered at pH 3.0 Reaction * No protein → strip remains yellow * Protein present → indicator-protein complex forms * Color changes to green/bluish-green * Shade depends on type & concentration of protein Result * Color develops in 30–60 seconds * Reported as: * Negative * Trace * 1+ * 2+ * 3+ * 4+ Sensitivity * Detects 5–20 mg albumin/dL ⸻ 2. Heat & Acetic Acid Test Principle * Heat causes protein coagulation & precipitation * Acetic acid enhances coagulation Procedure * Take 5 mL test tube * Fill 2/3 with urine * If urine alkaline → add few drops of 3% acetic acid * Boil upper portion for 2 minutes * Lower portion acts as control * If turbidity appears → add few drops of 3% acetic acid Interpretation * Turbidity disappears after acetic acid → Phosphates present * Turbidity persists after acetic acid → Proteins present Nature of Test * Semiquantitative * Graded from: * Trace * 1+ * 2+ * 3+ * 4+ ⸻ Acetic Acid Test for Bence-Jones Protein Procedure * 5 mL clear urine * Add 1 mL acetate buffer * Heat in water bath with thermometer Characteristic Finding * Starts precipitating at 40°C * Complete precipitation at 58°C * Dissolves when heated >60°C * Reappears on cooling to 40–60°C Best Detection Method * Protein electrophoresis ⸻ 3. Sulfosalicylic Acid Test Detects * Albumin * Globulin * Glycoproteins * Bence-Jones proteins Principle * Cold precipitation of proteins by strong acid Advantage * More sensitive & reliable than heat-acetic acid test Procedure * Take 2.5 mL urine * Add 2.5 mL of 3% sulfosalicylic acid slowly * Wait 10 minutes Interpretation * Cloudy precipitate → proteins present Limitation * Also precipitates: * Mucus * Bence-Jones proteins ⸻ 4. Heller’s Test Principle * Cold precipitation of proteins by strong acid Procedure * Take 5 mL urine * Add few drops of concentrated nitric acid Interpretation * White ring at urine-acid junction → Protein present Precaution * Filter turbid urine before testing ⸻ Quantitative Estimation of Urinary Protein Esbach’s Albuminometer Indications * Nephrotic syndrome * Protein >3.5 g/24 hr * Orthostatic/Postural proteinuria Principle * Cold precipitation of proteins by strong acid Procedure * Fill urine up to mark U * Add Esbach’s reagent up to mark R * Contains: * Picric acid * Citric acid * Stopper and mix * Keep for 24 hours * Read precipitate level * Divide reading by 10 Result * Gives percentage of total urinary proteins ⸻ Categories of Proteinuria According to Amount Heavy * 4 g/day Moderate * 1–4 g/day Mild * <1 g/day ⸻ According to Site/Cause 1. Renal * Glomerular * Tubular 2. Prerenal 3. Postrenal ⸻ Types of Glomerular Proteinuria Selective Proteinuria * Leakage of intermediate-sized proteins (<100 kDa) * Examples: * Albumin * Transferrin Nonselective Proteinuria * Leakage of proteins of different sizes * Includes larger proteins * Example: * Immunoglobulins ⸻ Bence-Jones Protein Definition * Light chains of immunoglobulins Seen In * Multiple myeloma * Macroglobulinemia * Lymphoma Characteristic Property * Precipitates at 40–60°C * Dissolves near 100°C * Reappears on cooling to 40–60°C ⸻ Microalbuminuria Definition Albumin in urine: * Above normal level * Below detection limit of routine tests Diagnostic Criteria Persistent urinary albumin excretion: * 20–200 mg/L OR * 20–200 µg/min * In early morning urine sample Significance * Indicates early and potentially reversible glomerular damage Detection Methods * Immunologic methods (antibodies) * Nephelometry * Immunoassay * Protein strip electrophoresis * HPLC ⸻ Causes of Microalbuminuria Diabetes Mellitus * Associated with ↑ cardiovascular mortality * Risk factor for renal mortality * Early predictor of diabetic nephropathy Essential Hypertension * Predicts cardiovascular morbidity * Predicts cardiovascular mortality ⸻ Causes of Proteinuria 1. Renal Causes A. Glomerular Damage Mechanism * Increased permeability of glomerular capillary wall Heavy Proteinuria * Nephrotic syndrome Moderate–Heavy Proteinuria * Rapidly progressive glomerulonephritis * Chronic glomerulonephritis * Malignant hypertension * SLE Mild–Moderate Proteinuria * Acute glomerulonephritis * Nephrosclerosis ⸻ B. Tubular Damage Mechanism * Failure of tubules to reabsorb low-MW proteins Moderate Proteinuria * Heavy metal intoxication * Vitamin D intoxication Mild Proteinuria * Acute pyelonephritis * Chronic pyelonephritis * Acute tubular necrosis * Polycystic kidney disease * Hypokalemia ⸻ 2. Prerenal Causes A. Overflow Proteinuria Mechanism * Excess protein in blood exceeds tubular reabsorptive capacity Causes Immunoglobulins * Plasma cell dyscrasias * Bence-Jones proteinuria Hemoglobin * Intravascular hemolysis Myoglobin * Skeletal muscle trauma Lysozyme * Acute myeloid leukemia (M4, M5) ⸻ B. Hemodynamic Proteinuria Mechanism * Altered glomerular blood flow Causes * Excessive exercise * Postural (orthostatic) albuminuria * Congestive cardiac failure * High fever * Exposure to cold * Dehydration Usually * Mild * Asymptomatic ⸻ 3. Postrenal Causes Due To Inflammatory or neoplastic lesions of: * Renal pelvis * Ureter * Bladder * Prostate * urethra.” Create one page image of masterchart of this topic protein Uris, including everything.
A comprehensive one-page medical masterchart/infographic on PROTEINURIA (Protein in Urine) for medical students. The chart should be highly detailed, organized, and visually clear with a clean clinical style. Include all the following sections with clear headings, subheadings, and organized layout: TITLE: PROTEINURIA - MASTER CHART (large bold header) SECTION 1 - NORMAL PROTEIN EXCRETION (top-left box): • Normal ≤150 mg/day • Proteins MW <50,000–60,000 Da: pass GBM, reabsorbed by proximal tubules • Albumin MW 69,000 Da: only very small amount filtered • Tamm-Horsfall glycoprotein (uromucoid): secreted by distal tubular cells & ascending loop of Henle; forms ≥1/3 of normal urinary protein SECTION 2 - DETECTION METHODS (top-center, 4 columns): 1. Reagent Strip: Protein error of pH indicators | Tetrabromophenol blue, pH 3.0 | No protein=yellow; Protein=green/bluish-green | Detects albumin only | Sensitivity: 5–20 mg albumin/dL | Reports: Neg, Trace, 1+–4+ 2. Heat & Acetic Acid: Boil upper 2/3 urine | Add 3% acetic acid | Turbidity persists=protein; Disappears=phosphates | Semiquantitative Trace–4+ 3. Sulfosalicylic Acid: 2.5 mL urine + 2.5 mL 3% SSA | Wait 10 min | Detects albumin, globulin, glycoproteins, BJP | More sensitive than heat test 4. Heller's Test: 5 mL urine + conc. HNO3 | White ring at junction = protein SECTION 3 - BENCE-JONES PROTEIN (small box): • Light chains of immunoglobulins • Seen in: Multiple myeloma, Macroglobulinemia, Lymphoma • Precipitates at 40–60°C, dissolves >60°C, reappears on cooling • Best detection: Protein electrophoresis SECTION 4 - QUANTITATIVE: ESBACH'S ALBUMINOMETER (small box): • Fill to U, add Esbach's reagent (picric acid + citric acid) to R • Stand 24 hrs | Read ÷ 10 = % total urinary protein • Used in: Nephrotic syndrome (>3.5 g/24hr), Orthostatic proteinuria SECTION 5 - MICROALBUMINURIA (box): • Above normal, below routine detection limit • Diagnostic: 20–200 mg/L OR 20–200 µg/min (early morning sample) • Causes: Diabetes Mellitus (↑CV & renal mortality, early predictor of diabetic nephropathy), Essential Hypertension (predicts CV morbidity/mortality) • Detection: Immunologic methods, Nephelometry, Immunoassay, HPLC, Electrophoresis SECTION 6 - CATEGORIES BY AMOUNT (small table): Heavy: >4 g/day | Moderate: 1–4 g/day | Mild: <1 g/day SECTION 7 - TYPES (Glomerular Proteinuria): • Selective: <100 kDa proteins (albumin, transferrin) • Nonselective: All sizes including immunoglobulins SECTION 8 - CAUSES OF PROTEINURIA (large central flowchart with 3 main branches): RENAL: A. Glomerular Damage (↑ permeability of GCW): - Heavy: Nephrotic syndrome - Moderate-Heavy: RPGN, Chronic GN, Malignant HTN, SLE - Mild-Moderate: Acute GN, Nephrosclerosis B. Tubular Damage (failure to reabsorb low-MW proteins): - Moderate: Heavy metal intox, Vit D intox - Mild: Acute/Chronic pyelonephritis, ATN, Polycystic kidney, Hypokalemia PRERENAL: A. Overflow (excess protein exceeds tubular capacity): - Immunoglobulins: Plasma cell dyscrasias, BJP - Hemoglobin: Intravascular hemolysis - Myoglobin: Skeletal muscle trauma - Lysozyme: AML (M4, M5) B. Hemodynamic (altered glomerular blood flow): - Exercise, Postural/orthostatic, CCF, High fever, Cold exposure, Dehydration - Usually mild, asymptomatic POSTRENAL: - Inflammatory/neoplastic lesions of renal pelvis, ureter, bladder, prostate, urethra Use a color-coded layout: blue for headings, light yellow for normal values, light green for detection methods, light orange for causes, light purple for microalbuminuria, white background. Use small icons, arrows, and clear typography. Make it dense but readable, suitable for a single A4 page study chart for MBBS students.
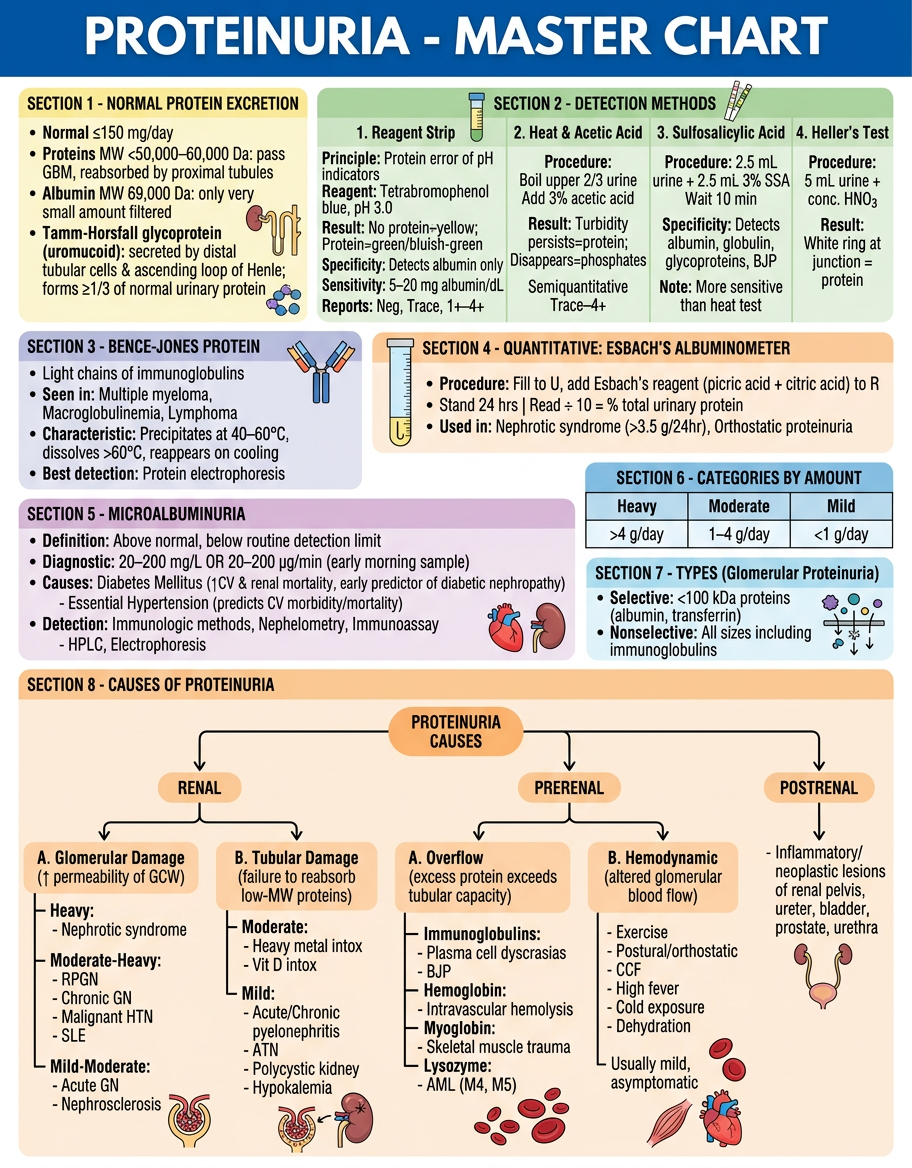
- Normal excretion values and Tamm-Horsfall protein details (top-left)
- 4 Detection methods side by side - Reagent Strip, Heat & Acetic Acid, SSA, Heller's - with principles, procedures, and interpretations
- Bence-Jones Protein box with characteristic thermal precipitation behavior
- Esbach's Albuminometer procedure summary
- Microalbuminuria - diagnostic criteria, causes (DM, HTN), and detection methods
- Categories by amount (Heavy/Moderate/Mild)
- Selective vs. Nonselective glomerular proteinuria
- Full causes flowchart - Renal (Glomerular + Tubular), Prerenal (Overflow + Hemodynamic), and Postrenal - all color-coded