A/N ratio for adenoid assess ment with respect to OSA according to standard ENT textbook
Reading File
Finding Sources
Finding Sources
Finding Sources
Finding Sources
Reading File
Reading File
Reading File
Reading File
Finding Sources
Finding Sources
Finding Sources
Finding Sources
Finding Sources
Searching the Web
A/N ratio adenoid nasopharynx OSA assessment ENT textbook lateral X-ray 0.8
Loading Image
Reading File
I now have enough information from the textbooks and web sources to give a comprehensive answer. Let me compile everything.
A/N Ratio for Adenoid Assessment in OSA
What is the A/N Ratio?
The Adenoid-Nasopharynx (A/N) ratio is a radiological measurement made on a lateral soft-tissue radiograph of the nasopharynx (lateral neck/postnasal space X-ray). It quantifies the degree of adenoid hypertrophy relative to the available nasopharyngeal airway space.
How to Measure
The measurement involves two dimensions on the lateral X-ray:
| Parameter | Definition |
|---|---|
| A (Adenoid depth) | Perpendicular distance from the anterior margin of the basiocciput (the straight portion) to the point of maximal adenoid prominence |
| N (Nasopharyngeal depth) | Distance from the posterior end of the hard palate to the anteroinferior edge of the sphenobasioccipital synchondrosis (width of the nasopharyngeal airway) |
A/N ratio = A ÷ N
Interpretation / Cut-off Values
| A/N Ratio | Interpretation |
|---|---|
| < 0.6 | Normal - no significant adenoid enlargement |
| 0.6 - 0.7 | Mild-moderate enlargement, watch and wait |
| > 0.71 - 0.73 | Pathological adenoid hypertrophy (Elwany's criterion) |
| > 0.8 | Severe obstruction - strongly associated with OSA; surgical intervention indicated |
The most widely cited threshold for clinically significant adenoid hypertrophy associated with OSA is A/N ratio > 0.8, though some sources (Elwany) use > 0.73 as the cutoff for pathological hypertrophy.
Relevance to OSA
From Bailey & Love's Short Practice of Surgery (28th ed.):
"If excessive adenoidal hypertrophy causes blockage of the nasopharynx in association with tonsil hypertrophy, the upper airway may become compromised during sleep causing obstructive sleep apnoea (OSA)."
- Bailey & Love shows a plain lateral radiograph demonstrating a large pad of adenoid tissue in the postnasal space (see Figure 52.17 below), which is the standard image used for A/N ratio measurement:
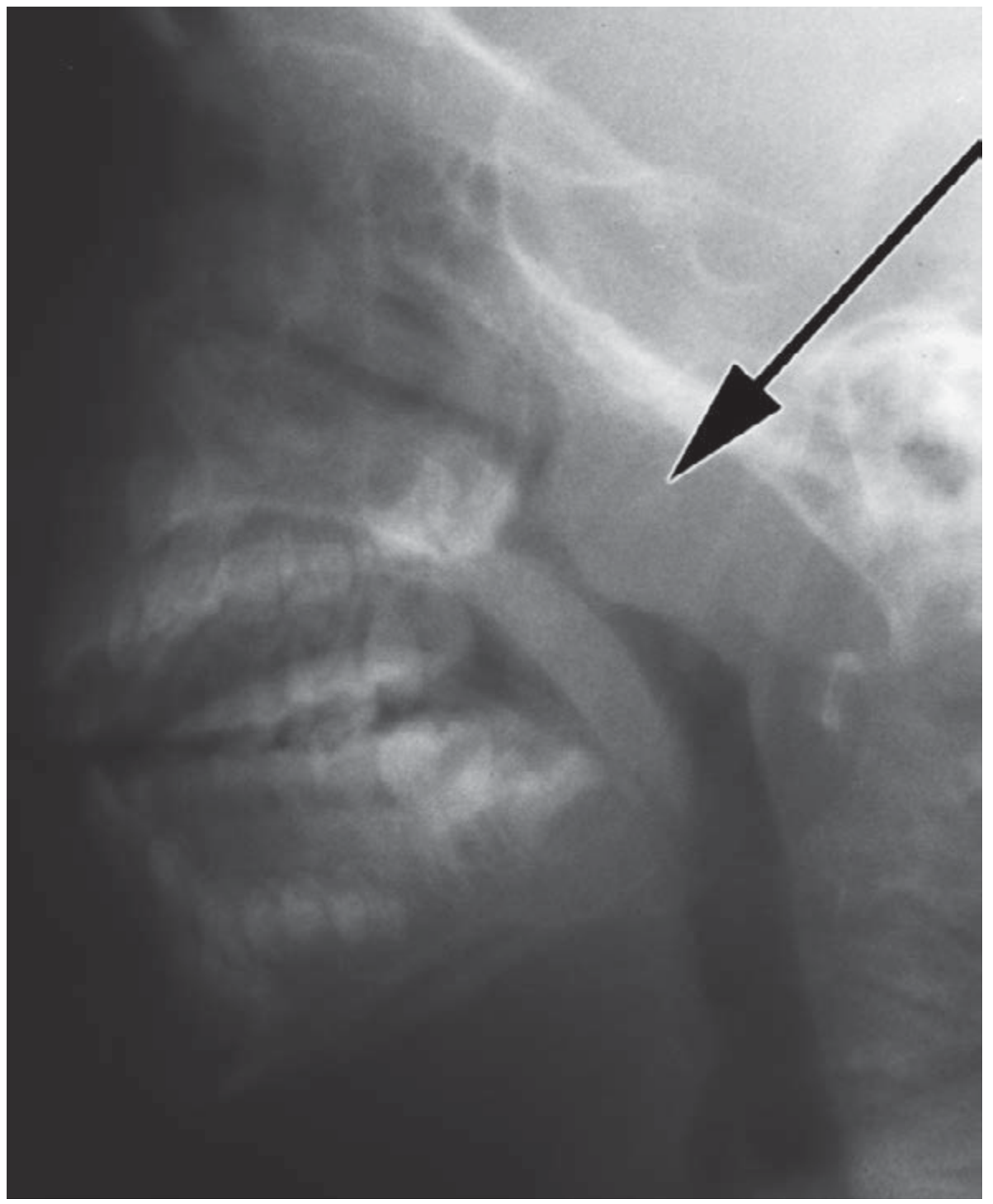
Figure 52.17 from Bailey & Love's - Plain lateral radiograph showing a large pad of adenoid tissue (arrow) in the postnasal space.
- Adenoid hypertrophy most commonly occurs between ages 4 and 10, and usually regresses at puberty.
- The size alone is NOT an indication for surgery; it is the consequence (e.g., OSA, nasal obstruction) that determines surgical need.
Role in Surgical Decision-Making
Adenoidectomy is indicated when:
- OSA associated with postnasal obstruction (most important indication)
- Recurrent/prolonged serous otitis media
- Recurrent rhinosinusitis
The A/N ratio on lateral X-ray, combined with flexible nasal endoscopy (FNE), forms the objective basis for surgical decision-making. FNE is actually considered superior for direct visualization; lateral X-ray is used when the child cannot cooperate with endoscopy.
Scott-Brown's Otorhinolaryngology (Vol 2) also references the correlation between adenoid-nasopharynx ratio and endoscopic findings (Cavlakli et al., Int J Pediatr Otorhinolaryngol, 2009), confirming the radiological measure's clinical validity.
Summary Table
| Feature | Detail |
|---|---|
| X-ray view used | Lateral soft-tissue nasopharynx |
| Numerator (A) | Maximal adenoid soft tissue depth from basiocciput line |
| Denominator (N) | Nasopharyngeal depth (hard palate to skull base) |
| Normal | < 0.6 |
| Pathological hypertrophy | > 0.73 (Elwany) |
| OSA-associated threshold | > 0.8 |
| Standard ENT texts | Bailey & Love's 28th ed., Scott-Brown's Vol 2 |
- Bailey and Love's Short Practice of Surgery 28th Edition, p. 803
- Scott-Brown's Otorhinolaryngology Head & Neck Surgery Vol 2, References (Cavlakli et al. 2009)
This is a shared conversation. Sign in to Orris to start your own chat.