Morphological chnges of mi
Reading File
Finding Sources
Finding Sources
Finding Sources
Finding Sources
Reading File
Reading File
Reading File
Reading File
Reading File
Reading File
Loading Image
Reading File
Now I have all the information needed for a complete, detailed answer. Let me compose the full response.
Morphological Changes of Myocardial Infarction (MI)
The morphological changes of MI follow a predictable, time-dependent sequence progressing from reversible ischemic injury through coagulative necrosis, inflammation, and finally fibrous scar formation. The primary mechanism of cell death is ischemic coagulative necrosis (though apoptosis also occurs). - Robbins, Cotran & Kumar Pathologic Basis of Disease
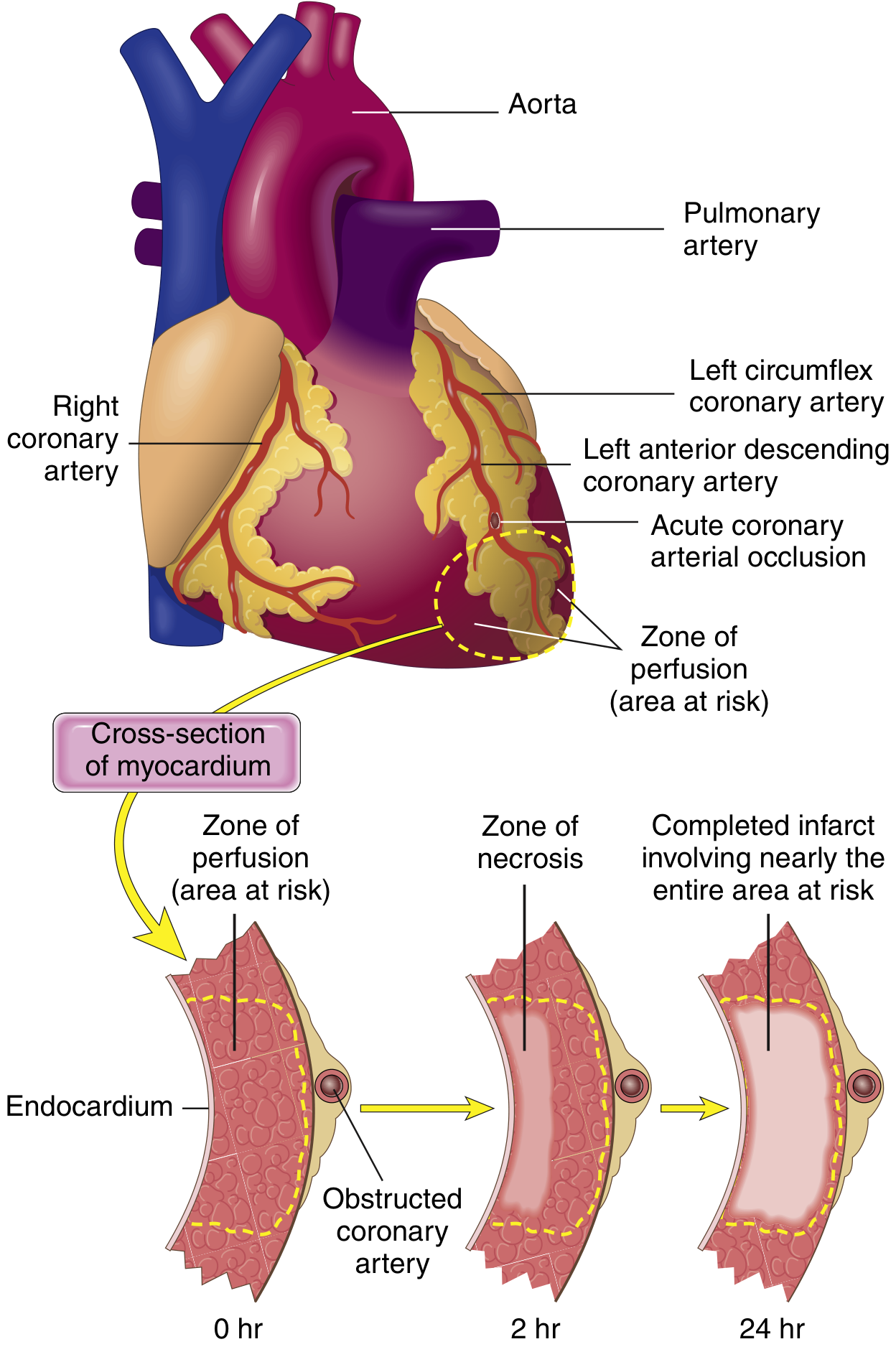
Progression of Necrosis Through the Wall
Necrosis begins in the subendocardial zone - the region most distal from epicardial vessels and exposed to the highest intramural pressures. Without intervention, a "wavefront" of necrosis expands outward, and within 3-6 hours the full infarct extent is reached (transmural infarct). A narrow rim immediately beneath the endocardium is spared because it can be oxygenated by diffusion from the ventricular cavity.
Timeline of Morphological Changes
The classic table (Table 12.5, Robbins & Cotran) is the standard reference:
Phase 1: Reversible Injury
| Time | Gross | Light Microscope | Electron Microscope |
|---|---|---|---|
| 0 - 0.5 hr | None | None | Relaxation of myofibrils; glycogen loss; mitochondrial swelling |
Phase 2: Irreversible Injury - Early (0.5 hr - 3 days)
| Time | Gross Features | Light Microscope (H&E) | EM |
|---|---|---|---|
| 0.5 - 4 hr | None | Usually none; variable waviness of fibers at border | Sarcolemmal disruption; mitochondrial amorphous densities |
| 4 - 12 hr | Occasionally dark mottling | Coagulative necrosis beginning; wavy fibers; early contraction band necrosis; early neutrophilic infiltrate | - |
| 12 - 24 hr | Dark mottling | Coagulative necrosis; pyknosis of nuclei; cytoplasmic hypereosinophilia; marginal contraction band necrosis; interstitial edema; neutrophilic infiltrate begins | - |
| 1 - 3 days | Mottling with yellow-tan infarct center | Coagulative necrosis with loss of nuclei and striations; brisk neutrophilic infiltrate in interstitium | - |
Key microscopic hallmarks of this phase:
- Wavy fibers - the stretching and buckling of dead, non-contractile fibers pulled by adjacent viable contracting myocardium
- Cytoplasmic hypereosinophilia - loss of cytoplasmic RNA → brighter pink on H&E
- Nuclear pyknosis, karyorrhexis, then karyolysis - progressive nuclear death
- Contraction bands - dense transverse bands of hypercontracted sarcomeres seen especially at borders and with reperfusion
Phase 3: Progressive Necrosis and Early Repair (3 days - 3 weeks)
| Time | Gross Features | Light Microscope |
|---|---|---|
| 3 - 7 days | Hyperemic border; central yellow-tan softening | Macrophage infiltration begins (replacing neutrophils); beginning disintegration of dead myofibers; granulation tissue starts at margins |
| 7 - 10 days | Maximally yellow-tan and soft; depressed borders | Well-developed granulation tissue with neovascularization at margins; progressive loss of necrotic debris |
| 10 - 14 days | Red-gray depressed infarct borders | Established granulation tissue (macrophages + fibroblasts + new vessels); collagen begins depositing |
| 2 - 8 weeks | Gray-white fibrous tissue | Fibrosis progressively replaces granulation tissue; collagen deposition advancing |
Phase 4: Healed Scar (>2 months)
| Time | Gross | Histology |
|---|---|---|
| >2 months | Firm, white fibrous scar | Dense collagenous scar - pale, acellular, avascular; no viable myocytes |
Early Detection Techniques
Because MIs less than 12 hours old are often not visible on gross examination alone, a histochemical trick is used: Triphenyl tetrazolium chloride (TTC) stain. Intact myocardium with preserved lactate dehydrogenase (LDH) stains brick-red; infarcted tissue (where LDH has leaked out) appears as an unstained pale zone. This test works if the infarct is at least 2-3 hours old. - Robbins, Cotran & Kumar
Gross Appearance Summary
| Time | Gross Appearance |
|---|---|
| 0 - 12 hr | No visible change (TTC needed) |
| 12 - 24 hr | Reddish-blue discoloration (congestion, extravasated blood) |
| 1 - 3 days | Dark mottling; yellow-tan center begins |
| 3 - 7 days | Yellow-tan, soft, surrounded by hyperemic border |
| 1 - 3 weeks | Yellow-tan, soft, depressed; granulation tissue at edges |
| >2 months | Gray-white firm fibrous scar |
Special Feature: Reperfusion Injury Morphology
When blood flow is restored (by thrombolysis or PCI), reperfused infarcts show additional/modified changes:
- Contraction band necrosis is greatly accentuated - a hallmark of reperfused MI
- Mitochondria show large amorphous densities
- Cell membranes are disrupted
- Large hemorrhagic areas due to vascular damage from returning blood
- Despite this, reperfusion is still beneficial as it limits overall infarct size
Complications Visible Morphologically
| Complication | Timing | Morphology |
|---|---|---|
| Fibrinous pericarditis | 2-3 days | Roughened, dark epicardial surface over infarct |
| Ventricular free wall rupture | 3-7 days | Tear through softened necrotic wall |
| Septal rupture | 3-7 days | Perforation of interventricular septum |
| Papillary muscle rupture | 3-5 days | Necrotic papillary muscle head detaches |
| Mural thrombus | Days to weeks | Thrombus overlying endocardium of infarct zone |
| Ventricular aneurysm | Weeks to months | Outward bulging of thinned fibrous scar |
Sources:
- Robbins, Cotran & Kumar Pathologic Basis of Disease (Table 12.5 - Evolution of Morphologic Changes in MI)
- Robbins & Kumar Basic Pathology (Chapter 9: Myocardial Response to Ischemia)
This is a shared conversation. Sign in to Orris to start your own chat.