
IMG-20260521-WA0001.jpg
Give full answers visually
Reading File
Finding Sources
Finding Sources
Finding Sources
Searching Images
therapeutic index drug concentration therapeutic window toxic level
Reading File
Reading File
Reading File
Loading Image
Loading Image
Reading File
Finding Sources
Finding Sources
Loading Image
Reading File
Finding Sources
Searching Images
aminoglycoside mechanism of action 30S ribosome protein synthesis
Searching Images
therapeutic drug monitoring peak trough concentration time curve
Loading Image
Loading Image
I now have all the information needed. Here are the complete, fully detailed answers to all five questions with textbook figures.
AIM: Therapeutic Drug Monitoring (TDM) — Mrs. Nirmala Case
Q1. Define TDM | Therapeutic Effect | Therapeutic Index | Toxic Effect (with Figures)
🔷 Therapeutic Drug Monitoring (TDM)
TDM is the clinical practice of measuring drug concentrations in a patient's blood (plasma/serum) at defined intervals to maintain concentrations within a therapeutic window — above the minimum effective concentration (MEC) and below the minimum toxic concentration (MTC). Drug level results guide individualized dose adjustments to maximize efficacy and minimize toxicity.
🔷 Therapeutic Effect
The desired pharmacological response a drug produces when its plasma concentration lies within the therapeutic range. In Mrs. Nirmala's case: elimination of Gram-negative UTI bacteria (bactericidal effect of gentamicin).
🔷 Therapeutic Index (TI)
TI = TD₅₀ / ED₅₀
| Term | Meaning |
|---|---|
| ED₅₀ | Dose effective in 50% of the population |
| TD₅₀ | Dose toxic in 50% of the population |
| Large TI | Wide safety margin (e.g. penicillin) |
| Narrow TI | Small safety margin → requires TDM (e.g. gentamicin, digoxin, warfarin, lithium) |
Gentamicin has a narrow TI — toxic levels are close to therapeutic levels, which is exactly why TDM is mandatory.
Figure: Wide vs. Narrow Therapeutic Ratio (Harrison's Principles of Internal Medicine)
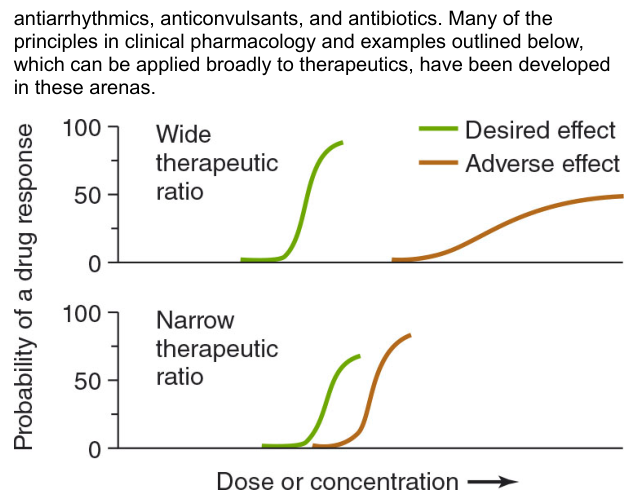
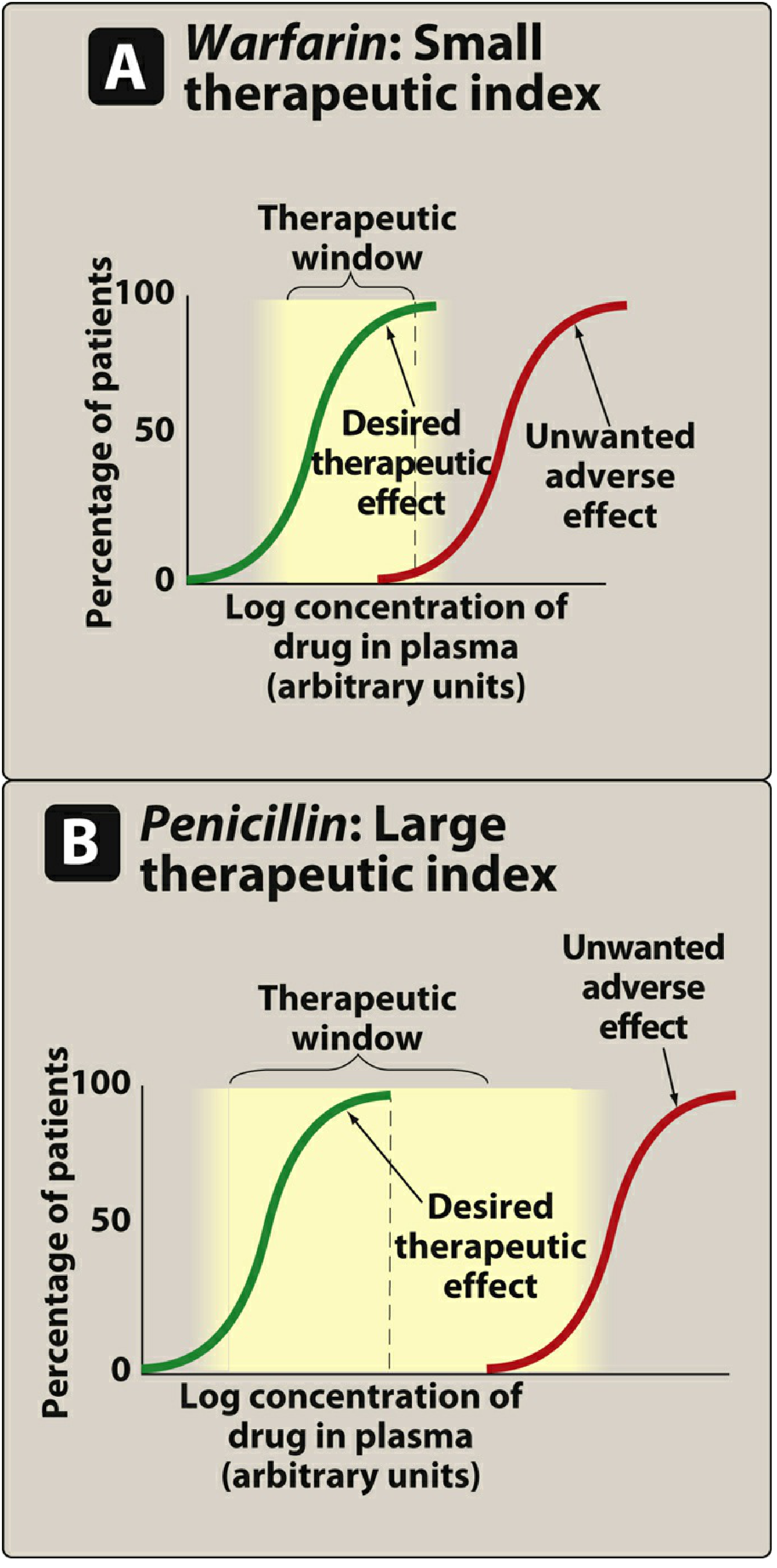
Figure: Small TI (Warfarin) vs Large TI (Penicillin) (Lippincott Illustrated Reviews: Pharmacology)
🔷 Toxic Effect
The adverse pharmacological response occurring when plasma drug concentration exceeds the MTC. In Mrs. Nirmala: tinnitus, dizziness (ototoxicity) + rising creatinine, decreased urine output (nephrotoxicity) — both classic signs of gentamicin toxicity at supratherapeutic concentrations.
Q2. Usefulness of TDM | Drugs Requiring TDM vs Not
Usefulness of TDM
- Individualizes dosing — accounts for patient variability in pharmacokinetics
- Detects toxicity early — especially for narrow TI drugs
- Monitors compliance/adherence
- Guides dose adjustments during renal/hepatic impairment, pregnancy, drug interactions
- Establishes individual therapeutic range when a patient is well-controlled
- Distinguishes drug failure from sub-therapeutic levels
- Monitors during formulation changes or interacting drug additions
In Mrs. Nirmala: GFR = 50 mL/min (mild renal impairment) → gentamicin is renally eliminated → reduced clearance → drug accumulation → toxicity. TDM would have detected rising trough levels before toxicity developed.
Drugs Requiring TDM (Narrow Therapeutic Index)
| Category | Examples |
|---|---|
| Aminoglycosides | Gentamicin, tobramycin, amikacin |
| Anticonvulsants | Phenytoin, carbamazepine, phenobarbital, valproate |
| Cardiac drugs | Digoxin, lidocaine, procainamide |
| Immunosuppressants | Cyclosporine, tacrolimus |
| Anticoagulants | Warfarin (INR monitoring) |
| Mood stabilizers | Lithium |
| Antifungals | Voriconazole |
| Anti-TB | Isoniazid (in specific populations) |
| Antibiotics | Vancomycin |
Drugs NOT Requiring TDM (Wide TI)
- Penicillins, cephalosporins, macrolides (azithromycin, erythromycin)
- Most NSAIDs, antacids, antihistamines
- Vitamins, iron supplements
- Most beta-blockers at standard doses
Q3. Methods of TDM
| Method | Principle | Use |
|---|---|---|
| Immunoassay (EMIT, FPIA, CLIA) | Antibody-antigen interaction; most widely used | Routine clinical labs; rapid results |
| HPLC (High-Performance Liquid Chromatography) | Separation by polarity/size | Gold standard; highly accurate; detects metabolites |
| LC-MS/MS (Liquid Chromatography–Mass Spectrometry) | Mass-to-charge ratio identification | Most sensitive; multiple drugs simultaneously |
| GC-MS (Gas Chromatography–Mass Spectrometry) | Volatile compounds | Toxicology screening |
| Fluorescence Polarization Immunoassay (FPIA) | Polarized light absorption | Aminoglycoside monitoring |
| Radioimmunoassay (RIA) | Radiolabeled antigen competition | Less common now; radiation hazard |
Sampling Timing (Critical for TDM Accuracy)
Figure: Pharmacokinetic model — Peak (Cmax), Trough, AUC/MIC (Harrison's Principles of Internal Medicine)
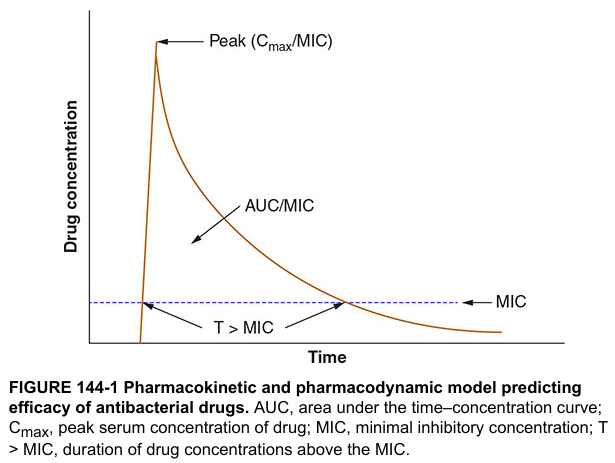
- Peak — drawn 30–60 min after IV infusion ends; reflects maximum concentration (target: 5–10 mcg/mL for gentamicin)
- Trough — drawn just before next dose; reflects minimum/residual concentration (target: <2 mcg/mL, ideally <1 mcg/mL)
- AUC monitoring — increasingly preferred for aminoglycosides to correlate with both efficacy and toxicity
Q4. Classify Gentamicin | Mechanism | Toxicity | Uses | Nephrotoxicity & Ototoxicity Mechanisms
Classification
Gentamicin → Aminoglycoside antibiotic → Bactericidal → Active against aerobic Gram-negative bacilli
Naturally derived from Micromonospora purpurea (Note: hence "-micin" not "-mycin")
Mechanism of Action
Figure: Aminoglycoside mechanism on 30S ribosome (Protein synthesis inhibitors diagram)
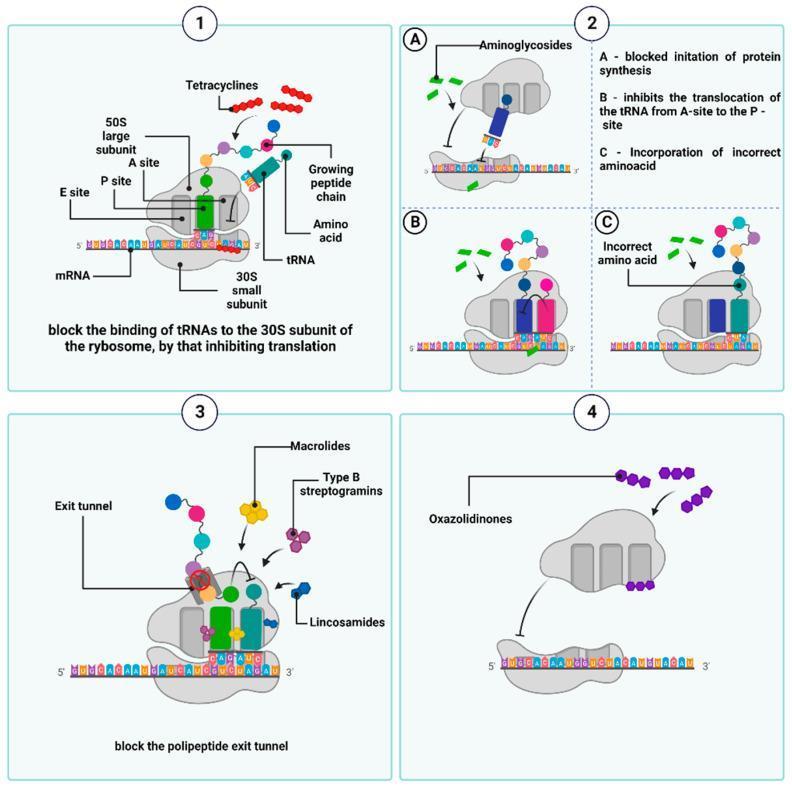
Step-by-step:
- Gentamicin is actively transported into bacteria via an oxygen-dependent uptake mechanism (requires electrochemical gradient — therefore inactive in anaerobes and acidic/hypoxic environments)
- Binds irreversibly to the 30S ribosomal subunit (16S rRNA)
- Results in:
- (A) Blocks initiation of protein synthesis
- (B) Inhibits translocation of tRNA from A-site to P-site
- (C) Causes mRNA misreading → incorporation of wrong amino acids → abnormal/toxic proteins → cell membrane disruption → cell death (bactericidal)
Spectrum of Activity
- Aerobic Gram-negative: E. coli, Klebsiella, Pseudomonas aeruginosa, Proteus, Enterobacter, Serratia
- Synergy with β-lactams for: Enterococcus (endocarditis), Staphylococcus (severe infections)
- NOT effective against: anaerobes, streptococci (alone), MRSA
Clinical Uses
- Serious UTI (pyelonephritis, sepsis)
- Gram-negative bacteremia/septicemia
- Pneumonia (nosocomial, Gram-negative)
- Endocarditis (synergistic combination)
- Meningitis (intrathecal route)
- Pelvic infections
Adverse Effects (Toxicity)
Figure: Aminoglycoside adverse effects (Lippincott Illustrated Reviews: Pharmacology)
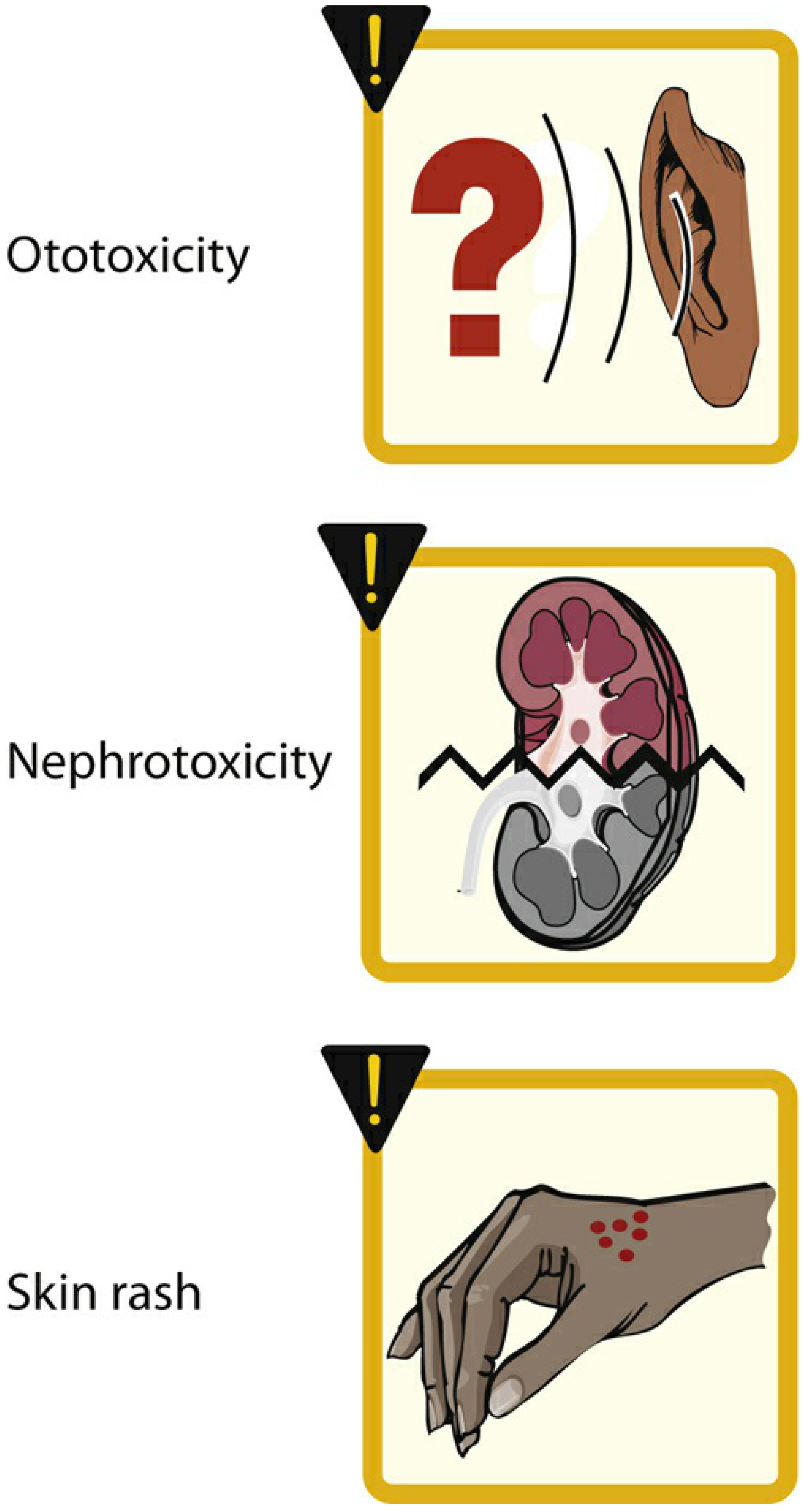
Mechanism of Nephrotoxicity
Gentamicin is filtered by glomeruli and reabsorbed by proximal tubular cells (megalin receptor–mediated endocytosis). Once inside:
- Accumulates in lysosomes and mitochondria of proximal tubular cells
- Disrupts calcium-mediated transport processes
- Causes release of lysosomal enzymes → phospholipidosis
- Leads to cell death → Acute Tubular Necrosis (ATN)
- Clinically: ↑ creatinine, ↓ GFR, ↓ urine output, electrolyte wasting (Mg²⁺, K⁺, Ca²⁺)
- Usually reversible if drug stopped early; can be irreversible with prolonged exposure
Risk factors in Mrs. Nirmala: Pre-existing mild renal impairment (GFR 50 mL/min) + standard dosing without dose adjustment + elderly female
Mechanism of Ototoxicity
- Aminoglycosides accumulate in the endolymph and perilymph of the inner ear
- Preferentially damage outer hair cells of the cochlea (basal turn → high-frequency hearing loss first) and vestibular hair cells
- Mechanism: Formation of reactive oxygen species (ROS) → lipid peroxidation → hair cell apoptosis
- Cochlear damage → auditory ototoxicity: tinnitus (as in Mrs. Nirmala), high-frequency hearing loss, deafness
- Vestibular damage → vestibulotoxicity: vertigo, ataxia, loss of balance
- Gentamicin is predominantly vestibulotoxic (also nephrotoxic)
- Damage is often irreversible — cochlear hair cells do not regenerate
- Potentiated by: concurrent loop diuretics (furosemide), cisplatin, pre-existing hearing loss
Q5. Outline the Management of Mrs. Nirmala
Immediate Actions
| Priority | Action |
|---|---|
| 1. Stop gentamicin immediately | Prevent further nephro- and ototoxic accumulation |
| 2. Obtain gentamicin levels | Peak + trough to confirm supratherapeutic concentrations |
| 3. Assess renal function | Repeat serum creatinine, BUN, urine output, GFR, urinalysis |
| 4. Audiometric evaluation | Assess degree of hearing loss/tinnitus |
Supportive/Medical Management
Renal (ATN Management):
- IV fluid hydration (isotonic saline) to maintain adequate renal perfusion
- Strict input/output monitoring
- Electrolyte correction (Mg²⁺, K⁺, Na⁺)
- Avoid all other nephrotoxic drugs (NSAIDs, contrast agents, vancomycin if possible)
- Dialysis if progressive oliguria/severe azotemia develops
Auditory/Vestibular:
- No specific reversal agent exists for ototoxicity
- Antioxidant agents (N-acetylcysteine, aspirin) — some evidence but not standard practice
- Audiological follow-up; hearing aids if permanent loss
Alternative Antibiotic for UTI (Replacing Gentamicin)
Renal-dose adjusted alternatives for Gram-negative UTI:
- Ceftriaxone 1–2g IV once daily (dose adjustable for GFR)
- Piperacillin-tazobactam (renal dose adjusted)
- Meropenem (if resistant organism suspected, renal dose adjusted)
- Fluoroquinolone (ciprofloxacin, if susceptible — oral transition appropriate for UTI)
Dose Adjustment Principle (For Future Reference)
For aminoglycosides in renal impairment:
Adjusted dose = Normal dose × (Patient's GFR / Normal GFR)
Or equivalently, extend the dosing interval proportional to reduced creatinine clearance. Mrs. Nirmala's GFR of 50 mL/min means the 8-hour interval should have been extended to ~16 hours minimum, with dose reduction.
Monitoring After Switching
- Renal function tests daily (creatinine, GFR, urine output)
- Repeat audiometry at 2–4 weeks
- Blood cultures + urine cultures to confirm organism susceptibility
- Clinical response (fever, WBC, symptoms)
- Repeat TDM if aminoglycosides are unavoidable in the future
Sources: Katzung's Basic & Clinical Pharmacology (16th ed.), Lippincott Illustrated Reviews: Pharmacology, Harrison's Principles of Internal Medicine (22nd ed.), Medical Microbiology (Murray 9th ed.)
Explain competitive and noncompetitive enzyme inhibition and reversible and irreversible binding visually
Your credits are exhausted. Your daily credits reset tomorrow, or you can purchase a top-up for more.
This is a shared conversation. Sign in to Orris to start your own chat.