Teach me urolithiasis from scratch to pro level
Reading File
Finding Sources
Finding Sources
Searching PubMed
"kidney stones" AND "management"[MeSH Terms]
Reading File
Reading File
Reading File
Searching PubMed
"nephrolithiasis" AND "treatment"[MeSH Terms]
Reading File
Reading File
Finding Sources
Searching PubMed
"nephrolithiasis" AND "recurrence prevention"
Reading File
Reading File
Loading Image
Reading File
Finding Sources
Finding Sources
Reading File
Reading File
Reading File
Loading Image
Reading File
I now have rich, comprehensive content from multiple authoritative textbooks. Let me now compose the complete, pro-level teaching guide.
Urolithiasis: A Complete Guide from Scratch to Pro Level
Sources: Harrison's Principles of Internal Medicine 22e, Comprehensive Clinical Nephrology 7e, Campbell-Walsh-Wein Urology, Bailey & Love's Surgery 28e, National Kidney Foundation Primer 8e, Brenner & Rector's The Kidney
Part 1 - Foundations: What Is Urolithiasis?
Urolithiasis is the formation of calculi (stones) anywhere in the urinary tract. The word derives from the Greek ouron (urine) + lithos (stone). Based on location, the same condition gets different names:
| Location | Term |
|---|---|
| Kidney (renal pelvis / calyces) | Nephrolithiasis |
| Ureter | Ureterolithiasis |
| Bladder | Cystolithiasis |
| Urethra | Urethrolithiasis |
Part 2 - Epidemiology
- Up to 20% of men and 10% of women will develop at least one stone during their lifetime (NHANES 2007-2016)
- Prevalence is rising globally, driven by Westernization of diet, increasing BMI, and metabolic syndrome
- Prevalence is ~50% lower in Black individuals compared to white individuals
- Peak incidence in white men: ~3.5 cases/1000/year at age 40
- Peak incidence in white women: ~2.5 cases/1000/year in their thirties
- Recurrence is the rule, not the exception - without intervention, 50% recur within 5 years
- Stone disease has a major economic impact because those affected are often of working age
- Harrison's Principles of Internal Medicine 22e
Part 3 - Stone Types and Their Distribution
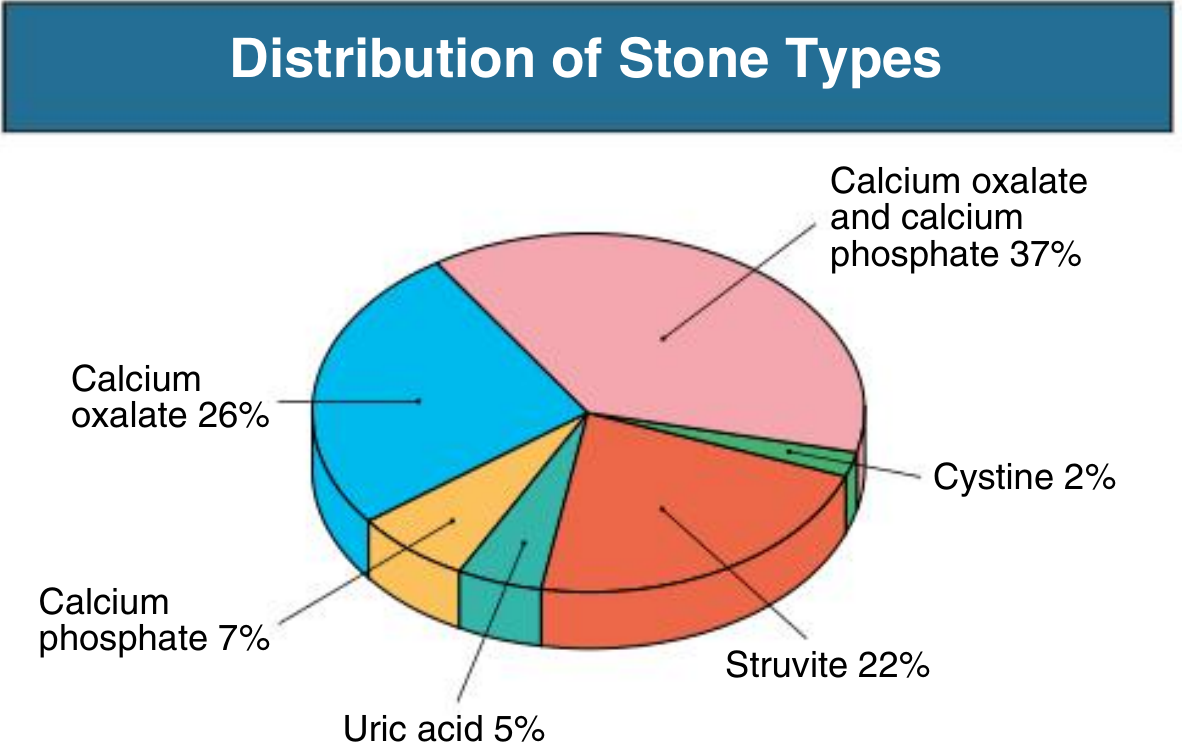
Fig. 1: Distribution of urinary stone types - Comprehensive Clinical Nephrology 7e
| Stone Type | Frequency | Urine pH | Radiopacity | Key Feature |
|---|---|---|---|---|
| Calcium oxalate | ~75% (pure + mixed) | Acidic | Radiopaque | Most common; two forms: monohydrate (harder) and dihydrate |
| Calcium phosphate | ~15% | Alkaline | Radiopaque | Associated with renal tubular acidosis, hyperparathyroidism |
| Calcium oxalate + phosphate (mixed) | ~37% | Variable | Radiopaque | Most recurrent type |
| Uric acid | ~8% | Acidic (<5.5) | Radiolucent | Only stone invisible on plain X-ray |
| Struvite | ~1-22%* | Alkaline | Radiopaque | Infection stones; form staghorn calculi |
| Cystine | <2% | Acidic | Mildly opaque (sulfur) | Genetic (cystinuria); young patients |
Note: Struvite prevalence varies by population and referral bias (higher in surgical series).
Part 4 - Pathophysiology: How Stones Form
The Core Concept: Supersaturation
Urine is a complex solution. Stone formation begins when the concentration of stone-forming ions exceeds their solubility product - this is called supersaturation. However, supersaturation alone is not enough because most people's urine is supersaturated with calcium oxalate at some point - what prevents stones in most people is the presence of crystallization inhibitors.
Think of it in 3 steps:
Supersaturation → Nucleation → Crystal Growth/Aggregation → Stone
Randall's Plaques - The Modern Understanding
Recent studies changed the paradigm. Renal biopsies of stone formers show calcium phosphate deposits in the renal interstitium (Randall's plaques). These deposits begin at the thin limb of the loop of Henle, extend to the papilla, and erode through the papillary epithelium - providing a nidus for calcium oxalate stone formation at the papillary surface.
- Harrison's Principles of Internal Medicine 22e
Key Inhibitors of Stone Formation
The most important inhibitors of calcium-containing stones:
- Urinary citrate - most clinically important; chelates calcium, prevents nucleation
- Magnesium - competes with oxalate binding
- Pyrophosphate - inhibits crystal growth
- Nephrocalcin (glycoprotein) - inhibits crystal aggregation
- Tamm-Horsfall protein (uromodulin) - inhibits crystal aggregation
- Osteopontin
Low citrate ("hypocitraturia") is one of the most treatable risk factors for stones.
Risk Factors for Stone Formation
Urinary factors:
- Low urine volume (< 1.5 L/day) - most correctable factor
- Hypercalciuria (Ca > 250 mg/day women, >300 mg/day men)
- Hyperoxaluria (Ox > 40 mg/day)
- Hyperuricosuria (UA > 750 mg/day women, >800 mg/day men)
- Hypocitraturia (Cit < 320 mg/day)
- Alkaline urine (promotes calcium phosphate, struvite)
- Acidic urine (promotes uric acid, calcium oxalate)
Systemic conditions:
- Primary hyperparathyroidism (elevated Ca)
- Renal tubular acidosis type 1 (distal) - alkaline urine, hypocitraturia
- Gastrointestinal disease (Crohn's, gastric bypass) - enteric hyperoxaluria
- Gout / hyperuricemia
- Obesity and metabolic syndrome - acid urine, hyperuricosuria
- Type 2 diabetes mellitus
- Medullary sponge kidney
Part 5 - Stone-by-Stone Deep Dive
5A. Calcium Oxalate Stones
The most common stone. Forms in acidic to neutral urine.
Causes of hypercalciuria (3 types):
- Absorptive hypercalciuria - excess intestinal calcium absorption; suppresses PTH; normal/low serum Ca; normal fasting urine Ca
- Resorptive hypercalciuria - primary hyperparathyroidism (elevated PTH, serum Ca, urine Ca)
- Renal leak hypercalciuria - renal tubular defect leaking Ca into urine; high PTH secondary response; normal serum Ca
Causes of hyperoxaluria:
- Primary hyperoxaluria - autosomal recessive enzyme defects (AGXT, GRHPR, HOGA1); severe, early-onset, can cause oxalosis
- Enteric hyperoxaluria - fat malabsorption (Crohn's, bariatric surgery) → increased colonic oxalate absorption (fat binds Ca, leaving oxalate free to be absorbed)
- Dietary hyperoxaluria - excessive intake of spinach, nuts, chocolate, tea, rhubarb (see Box 60.4 from CCN)
Crystal morphology: bipyramidal (dihydrate) or dumbbell-shaped (monohydrate)
5B. Calcium Phosphate Stones
Predominantly hydroxyapatite or brushite. Form in alkaline urine.
Associated with:
- Distal renal tubular acidosis (type 1) - inability to acidify urine below pH 5.5; classic triad: nephrocalcinosis + alkaline urine + hypocitraturia
- Primary hyperparathyroidism
- Pregnancy (most common stone type in pregnancy)
- Topiramate use (carbonic anhydrase inhibitor → urinary alkalinization)
Brushite stones are SWL-resistant (hard).
5C. Uric Acid Stones
The only radiolucent stone. This is a classic exam fact.
Uric acid is the end product of purine metabolism. Solubility is pH-dependent - below pH 5.5, uric acid precipitates readily.
Three conditions produce uric acid stones:
- Hyperuricosuria - gout, high purine diet, tumor lysis syndrome, uricosuric drugs
- Persistently acidic urine (pH < 5.5) - most important factor; seen in obesity, metabolic syndrome, diabetes type 2 (insulin resistance impairs ammoniagenesis → low NH3 to buffer urine)
- Low urine volume
Key point: Many uric acid stone formers have normal serum uric acid. The problem is urine pH, not hyperuricemia.
Treatment by alkalization: Raising urine pH to 6.0-6.5 can dissolve existing uric acid stones (chemolysis) - the only stone type amenable to medical dissolution.
5D. Struvite Stones (Infection/Triple Phosphate Stones)
Composition: Magnesium ammonium phosphate (MgNH4PO4) + calcium carbonate apatite.
Formation mechanism:
Urease-producing bacteria → hydrolyze urea → NH4+ (ammonium) + OH- → urine becomes very alkaline → phosphate precipitates with Mg, Ca, ammonium
Key urease-producing organisms:
- Proteus mirabilis (most common)
- Klebsiella
- Pseudomonas
- Staphylococcus epidermidis
- Haemophilus, Yersinia
- Ureaplasma urealyticum (doesn't grow on routine media - request specifically!)
- NOT E. coli (does not produce urease)
Staghorn calculi: Large stones filling the renal pelvis and calyces - most are struvite. These are also called "stone cancer" because of their high morbidity.
Diagnosis: Alkaline urine (pH ≥7.0) + positive urine culture for urease-producer + large/staghorn stone
Treatment: Requires complete stone removal - bacteria persist in stone interstices. PCNL ± ESWL is the preferred approach. Antibiotics alone do not cure.
5E. Cystine Stones
Genetic disorder: Autosomal recessive (or dominant with incomplete penetrance) defect in tubular transport of dibasic amino acids (COLA mnemonic: Cystine, Ornithine, Lysine, Arginine). The SLC3A1 or SLC7A9 gene is mutated.
Cystine is the only one of the four amino acids that is poorly soluble at normal urine pH, so only cystine crystallizes.
Clinical features:
- Presents in 2nd-3rd decade of life
- Stones are mildly radiopaque (sulfur content) - described as "ground glass"
- Hexagonal crystals on urinalysis - pathognomonic
- Often recurrent, bilateral, staghorn-forming
Diagnosis: Urine sodium nitroprusside test (turns purple with cystine) + 24-hr urine cystine level
Treatment:
- High fluid intake (target urine volume > 3 L/day)
- Alkalinize urine to pH > 7.5 (potassium citrate, acetazolamide)
- Reduce dietary sodium and protein (reduces cystine excretion)
- Thiol drugs for refractory cases: D-penicillamine or tiopronin - these form soluble disulfide complexes with cystine
Part 6 - Urinary Crystals Under the Microscope
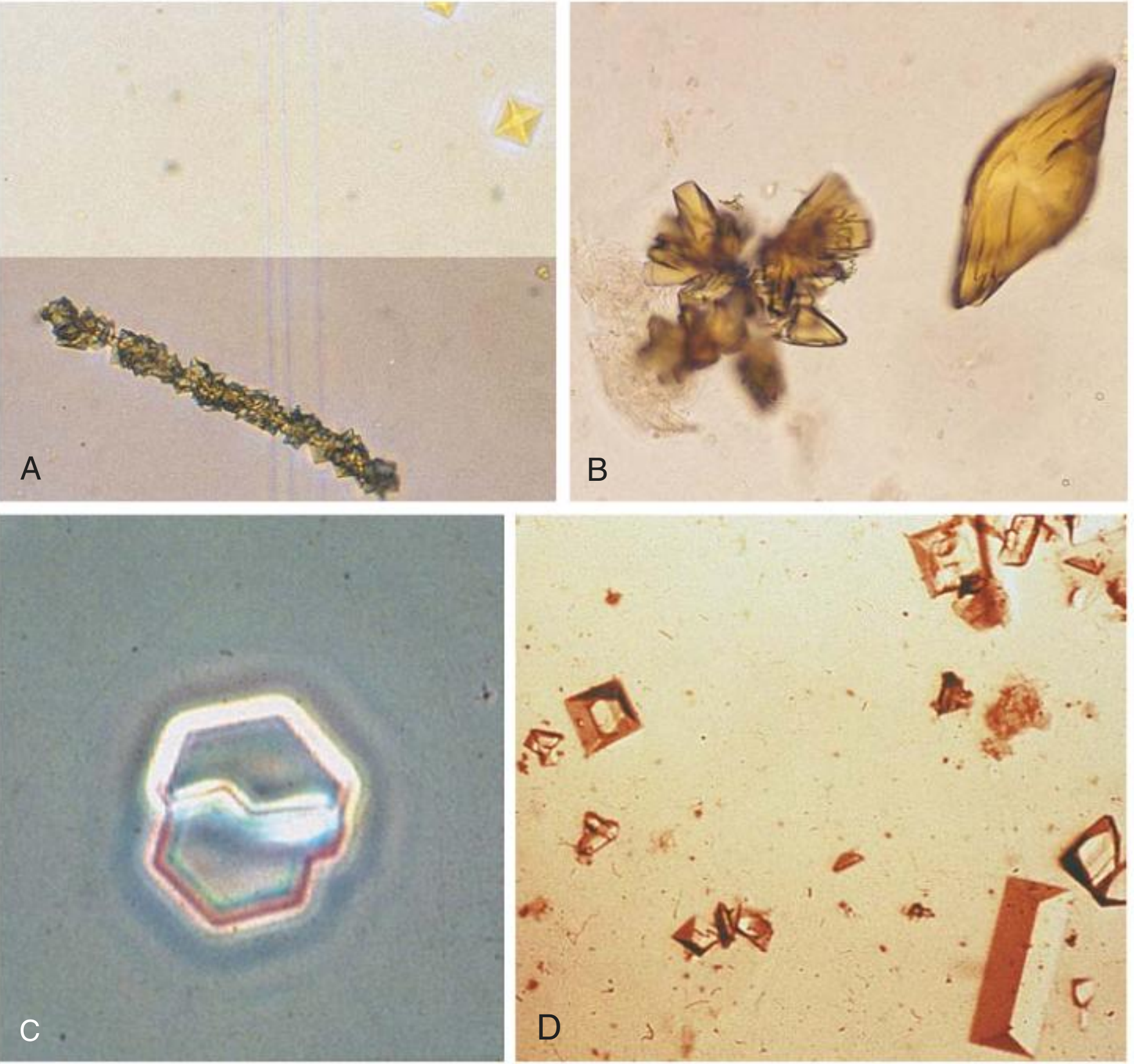
Fig. 2: Urinary crystals - A: calcium oxalate monohydrate (elongated/dumbbell); top shows dihydrate bipyramidal (yellow squares). B: uric acid (rosette and rhomboid). C: cystine (hexagonal). D: struvite "coffin-lid" rectangular. - Comprehensive Clinical Nephrology 7e
| Crystal | Appearance | pH |
|---|---|---|
| Calcium oxalate dihydrate | Bipyramidal ("envelope") | Acidic |
| Calcium oxalate monohydrate | Dumbbell / elongated | Acidic |
| Calcium phosphate | Amorphous or wedge-shaped prisms | Alkaline |
| Uric acid | Rhomboids, rosettes, yellow-brown | Acidic |
| Struvite | "Coffin-lid" rectangles | Alkaline |
| Cystine | Hexagonal plates | Acidic |
Part 7 - Clinical Presentation
The Classic Presentation
Renal colic: Sudden-onset, severe, cramping flank pain that radiates to the groin, labia, or testicle (following the path of the ureter). The pain is typically:
- Colicky - comes in waves as the ureter peristaltically contracts against the stone
- Unilateral
- Associated with nausea and vomiting
- Associated with gross or microscopic hematuria (90% of cases)
- Patient is typically restless and cannot find a comfortable position (vs. peritonitis where patients lie still)
Location-Specific Features
| Stone Location | Symptoms |
|---|---|
| Renal pelvis/calyces | Dull flank ache; often asymptomatic |
| Upper/mid-ureter | Flank pain ± radiation to lower abdomen |
| Ureterovesical junction (UVJ) | Severe pain + frequency, urgency, dysuria (mimics UTI) |
| Bladder | Suprapubic pain, frequency, hematuria |
Key Clinical Points
- "Pus under pressure" = infected obstructed kidney (UTI + obstructing stone) = urologic emergency requiring urgent drainage (ureteral stent or nephrostomy)
- Stones in the UVJ are the most painful because the UVJ is the narrowest point of the ureter
- Most stones (up to 80% of stones ≤ 4 mm) pass spontaneously
- A fever in a patient with an obstructing stone demands urgent intervention, not just antibiotics
Three Natural Narrowings of the Ureter
Stones preferentially get stuck at:
- Ureteropelvic junction (UPJ) - pelvis narrows to upper ureter
- Pelvic brim - ureter crosses the iliac vessels
- Ureterovesical junction (UVJ) - most narrow point; most stones impact here
Part 8 - Diagnosis
Initial Workup
Urinalysis: Hematuria (90%), crystals, pH, pyuria if infected
Urine culture: Always if infection suspected
Serum labs:
- BMP (creatinine - assess renal function, electrolytes)
- Calcium, uric acid, phosphate
- PTH if hypercalcemia present
Imaging Hierarchy
1. Non-contrast CT (NCCT) abdomen/pelvis - Gold Standard
- Sensitivity 96-100%, specificity 92-100%
- Identifies ALL stone types including radiolucent uric acid stones (except indinavir stones)
- Shows size, location, degree of obstruction, hydronephrosis, perinephric stranding
- Detects alternate diagnoses (appendicitis, aortic aneurysm)
- Low-dose CT protocols reduce radiation by 50-75% with ~96-97% sensitivity/specificity and are now preferred for initial workup
- Look for "soft-tissue rim sign" around UVJ stones = edema of ureteral wall confirms it's a true stone vs. phleboliths
2. Ultrasound
- No radiation; first-line in pregnancy and children
- Good at detecting hydronephrosis
- Sensitivity 29-69% for ureteral stones (lower than CT)
- Absence of ureteral jets on contralateral decubitus position suggests obstruction
3. KUB (kidney-ureter-bladder plain X-ray)
- Only shows radiopaque stones
- Used to monitor known calcium stones
- Cannot see uric acid stones
4. Intravenous urography (IVU/IVP)
- Historical gold standard; largely replaced by CT
- Still useful in pregnancy (limited IVU: ~93% accuracy)
5. MR urography
- Pregnancy option if ultrasound non-diagnostic
- Findings: signal void at stone, perinephric/periureteral edema, abrupt ureteral termination
- Campbell-Walsh-Wein Urology
Part 9 - Metabolic Evaluation (24-Hour Urine)
This is the "stone prevention workup" - identifies the underlying metabolic abnormality driving stone formation.
When to order: First-time stone formers with strong family history, pediatric patients, solitary kidney, recurrent stones (> 1 stone), or any complex stone disease.
24-Hour Urine Collection Measures:
- Volume (target >2 L)
- Calcium (>250 mg/day women, >300 mg/day men = hypercalciuria)
- Oxalate (>40 mg/day = hyperoxaluria)
- Uric acid (>750/800 mg/day = hyperuricosuria)
- Citrate (<320 mg/day = hypocitraturia)
- Sodium (marker of dietary salt intake - drives calciuria)
- pH (average and range throughout the day)
- Creatinine (validates completeness of collection: ~20-25 mg/kg/day)
- Supersaturation indices (calculated for CaOx, CaP, uric acid)
Part 10 - Acute Management of Renal Colic
Step-by-Step Approach
1. Analgesia (most important immediate goal)
- NSAIDs (ketorolac, diclofenac) - first-line; most effective for renal colic
- Mechanism: reduce ureteral prostaglandin-mediated spasm and renal pelvis pressure
- As effective as opioids with fewer side effects
- Opioids (morphine, hydromorphone) - if NSAIDs contraindicated or insufficient
- Antispasmodics (e.g., hyoscine) - adjunctive
2. Antiemetics - nausea/vomiting is nearly universal in acute colic
3. Hydration - IV fluids if patient cannot tolerate oral intake
4. Medical Expulsive Therapy (MET)
- Alpha-1 blockers (tamsulosin 0.4 mg daily) - relax ureteral smooth muscle, increase stone passage rates, especially for distal ureteral stones 5-10 mm
- Calcium channel blockers (nifedipine) - alternative; used in pregnancy for tocolysis at doses similar to MET doses
- Most beneficial for stones 5-10 mm; less evidence for smaller or larger stones
5. Monitoring
- Strain urine to capture the stone for analysis
- Re-imaging at 2-4 weeks if stone has not passed
- If no passage in 4-6 weeks → consider urologic intervention
Indications for Urgent/Emergency Intervention
- Infected obstructed kidney (fever + obstruction = emergency)
- Bilateral obstruction
- Obstruction of solitary kidney
- Uncontrolled pain
- Renal function deterioration
- Complete obstruction
Part 11 - Surgical Management
The introduction of ESWL, ureteroscopy (URS), and PCNL has made open stone surgery a last resort.
Extracorporeal Shock Wave Lithotripsy (ESWL)
- High-energy shock waves focused on stone under fluoroscopy/ultrasound guidance
- Works best for: stones < 2 cm, upper ureter, kidney (non-lower pole)
- Done under general/IV sedation
- Contraindications: pregnancy, coagulopathy, aortic aneurysm, distal obstruction, pacemaker
- Shock wave-resistant stones: calcium oxalate monohydrate, brushite, cystine (avoid ESWL, prefer URS/PCNL)
- Lower-pole stones have poor ESWL outcomes if: steep infundibular-pelvic angle, long lower-pole calyx (>10 mm), narrow infundibulum (<5 mm), skin-to-stone distance >10 cm
- Fragments ("steinstrasse") can obstruct - risk with large stones
Ureteroscopy (URS)
- Flexible or semi-rigid scope passed up the ureter
- Allows direct visualization + fragmentation (holmium laser) + stone basket retrieval
- Stone-free rates ~91-93% for stones up to 2 cm
- First-line for distal ureteral stones
- Preferred over ESWL for stones > 10 mm (higher stone-free rate)
- Can reach anywhere in the ureter and kidney (flexible URS)
- Risks: ureteral injury, stricture, UTI, ureteral avulsion (rare)
Percutaneous Nephrolithotomy (PCNL)
- Dilated tract percutaneously through the flank directly into the renal collecting system
- Nephroscope passed through tract; stone fragmented and removed
- Indications:
- Stones > 2 cm (in kidney)
- Staghorn / struvite stones
- Lower-pole stones > 10 mm
- ESWL-refractory stones < 2 cm
- Multiple stones
- Cystine stones
- Higher morbidity (bleeding, sepsis, adjacent organ injury) but highest stone-free rates
- Mini-PCNL / micro-PCNL - smaller tracts for pediatric patients or smaller stones
Surgical Decision Summary (AUA/EAU Guidelines)
| Stone Size | Location | Preferred Approach |
|---|---|---|
| < 10 mm | Ureter (any) | Observe (MET) / URS / ESWL |
| > 10 mm | Ureter | URS preferred over ESWL |
| < 20 mm | Non-lower-pole kidney | ESWL or URS |
| < 10 mm | Lower pole | ESWL or URS |
| 10-20 mm | Lower pole | URS preferred (or PCNL) |
| > 20 mm | Kidney | PCNL |
| Staghorn / struvite | Kidney | PCNL ± ESWL |
| Cystine, brushite | Any | URS or PCNL (ESWL-resistant) |
- Campbell-Walsh-Wein Urology; Comprehensive Clinical Nephrology 7e
Part 12 - Long-Term Prevention (Medical Management)
Universal Measures (All Stone Types)
- Increased fluid intake - target urine output > 2 L/day (ideally 2.5 L)
- This single intervention reduces recurrence risk by ~50%
- Optimal fluids: water, citrus juice (lemon/orange juice), coffee, tea, beer, wine
- Avoid: sugar-sweetened sodas (high fructose → vasopressin-dependent urine concentration, lower pH, uricosuria)
- Dietary sodium restriction - < 2 g/day sodium (reduces calciuria)
- Dietary protein moderation - animal protein increases calciuria, uricosuria, and lowers citrate
- Normal calcium intake - Do NOT restrict dietary calcium; this is a critical point
- Low dietary calcium increases intestinal oxalate absorption → more oxalate in urine
- Target 1000-1200 mg/day from diet (not supplements)
Stone-Specific Medical Prevention
| Stone Type | Medical Therapy | Mechanism |
|---|---|---|
| Hypercalciuric CaOx | Thiazide diuretics (HCTZ, chlorthalidone, indapamide) | Reduce urinary Ca by increasing renal Ca reabsorption; must replace K+ |
| Hypocitraturic CaOx | Potassium citrate | Increases urinary citrate; alkalinizes urine; chelates Ca |
| Hyperuricosuric CaOx | Allopurinol | Reduces uric acid production; reduces CaOx stone formation (mechanism not fully clear) |
| Uric acid stones | Potassium citrate (urine pH 6.0-6.5) | Alkalinizes urine → dissolves existing stones; prevents new ones |
| Uric acid stones | Allopurinol | Reduces uric acid production |
| Hyperoxaluria - dietary | Low-oxalate diet, pyridoxine (B6) | B6 is cofactor for AGXT (primary hyperoxaluria type 1) |
| Primary hyperoxaluria type 1 | Lumasiran (RNA interference drug) | Reduces hepatic oxalate production (new therapy) |
| Struvite stones | Complete stone removal + antibiotics | Must remove all stone material; bacteria in interstices |
| Cystine stones | High fluids, alkalinization, tiopronin or D-penicillamine | Thiol drugs form soluble cystine disulfide complexes |
| Absorptive hypercalciuria | Low-calcium diet (if type II) or cellulose phosphate | Binds intestinal calcium |
| Resorptive (primary HPT) | Parathyroidectomy | Removes source of excess PTH |
| Distal RTA | Potassium citrate | Corrects hypocitraturia + acidosis |
High-Oxalate Foods to Avoid:
Spinach, rhubarb, beets, Swiss chard, kale, nuts/peanut butter, chocolate, black tea, berries, tofu
High-Purine Foods to Avoid (for Uric Acid/Hyperuricosuric Stones):
Organ meats (liver, kidney, sweetbreads), shellfish, anchovies, sardines, beef, pork, meat extracts/gravies
Part 13 - Associated Conditions and Systemic Implications
Nephrolithiasis is not just a kidney problem. The following systemic associations are important:
| Condition | Mechanism |
|---|---|
| Hypertension | Shared metabolic risk; CKD from obstruction |
| Cardiovascular disease | Shared metabolic risk factors |
| Gout | Hyperuricemia; shared purine dysmetabolism |
| Reduced bone density | Especially in absorptive/resorptive hypercalciuria |
| Chronic kidney disease | Recurrent obstruction, infection, parenchymal damage |
| Cholelithiasis | Shared metabolic tendency |
| Type 2 diabetes / obesity | Acidic urine → uric acid stones; metabolic syndrome |
A UTI in the setting of an obstructing stone is a urologic emergency - "pus under pressure" requires immediate drainage before antibiotic levels can penetrate a bacteria-harboring stone.
Part 14 - Special Populations
Pregnancy
- Incidence similar to non-pregnant women (~1:200-4600)
- Calcium phosphate stones most common (unlike non-pregnant: CaOx predominates)
- Pregnancy is a state of relative urinary stasis + increased Ca/uric acid excretion - BUT also increased inhibitors (magnesium, citrate, nephrocalcin), which balance stone risk
- Diagnosis: Ultrasound first-line (radiation-free); sensitivity 29-69%; add transvaginal ultrasound for distal ureteral stones
- If US non-diagnostic: MR urography or limited IVU (93% accuracy)
- CT should be avoided but fetal radiation from abdominal CT is below malformation threshold
- Management: 64-84% pass spontaneously with conservative care
- Conservative: hydration, analgesia, antiemetics, antibiotics if infected; lie with symptomatic side up
- Nifedipine for MET (safe; comparable doses used for tocolysis)
- Surgical: ureteral stent or nephrostomy for persistent obstruction; ureteroscopy if needed
Children (Pediatrics)
- Prevalence: 1-5% in Asia, 5-10% in Europe, 15% in North America
- Metabolic evaluation is mandatory in all pediatric stone patients
- Common metabolic risk factors: hypercalciuria, hyperoxaluria, hypocitraturia
- ~25% are infection stones (urease-producing bacteria)
- Always evaluate for anatomic anomalies (UPJ obstruction, polycystic kidney, neurogenic bladder)
- Imaging: US preferred (radiation avoidance)
- PCNL available for stones > 2 cm; URS generally avoided < 5 years
- ESWL effective and safe under general anesthesia
- Bailey & Love's Surgery 28e; Creasy & Resnik's Maternal-Fetal Medicine
Part 15 - Pro-Level Pearls and Exam Traps
| Concept | Key Point |
|---|---|
| Only radiolucent stone | Uric acid (also: indinavir drug stones) |
| Only stone amenable to dissolution | Uric acid (alkalize urine to pH 6.0-6.5) |
| Most common staghorn stone | Struvite |
| Bacteria that do NOT make urease | E. coli (trick! most common UTI organism but does not cause struvite stones) |
| Hexagonal crystals on UA | Cystine - pathognomonic |
| ESWL-resistant stones | Calcium oxalate monohydrate, brushite (calcium phosphate), cystine |
| Randall's plaque | Calcium phosphate deposit at papillary tip - initiates CaOx stone formation |
| Most treatable single risk factor | Low urine volume - increase fluids to > 2 L/day |
| Restricting dietary calcium | INCREASES stone risk (increases enteric oxalate absorption) |
| Stone type in distal RTA | Calcium phosphate (alkaline urine + hypocitraturia) |
| Urease-producing but not grown on routine culture | Ureaplasma urealyticum - request specifically |
| "Pus under pressure" | Infected obstructed kidney = urologic emergency = drain first |
| Uric acid stone without hyperuricemia | Common! The problem is persistently acidic urine (pH < 5.5) from insulin resistance / metabolic syndrome |
| Gauging 24-hr urine collection adequacy | Urine creatinine ~20-25 mg/kg/day |
| Primary hyperoxaluria new treatment | Lumasiran (siRNA; targets hepatic LDHA) |
| Stone-free rate: URS vs. ESWL | URS > ESWL, but more invasive |
| Soft-tissue rim sign on CT | Confirms UVJ stone vs. phlebolith |
| Low-dose CT sensitivity | ~96-97%; reduces radiation by 50-75% |
Quick Summary Table
| Stone | pH | Radiopacity | Key Cause | Specific Treatment |
|---|---|---|---|---|
| Calcium oxalate | Acid | Opaque | Hypercalciuria, hyperoxaluria | Thiazides, K-citrate, hydration |
| Calcium phosphate | Alkaline | Opaque | RTA type 1, HPT, topiramate | K-citrate, treat RTA/HPT |
| Uric acid | Acid (<5.5) | Lucent | Metabolic syndrome, gout | Alkalinize urine, allopurinol |
| Struvite | Alkaline | Opaque | Urease-producing bacteria | Complete removal (PCNL) + abx |
| Cystine | Acid | Slightly opaque | Autosomal cystinuria | Tiopronin, alkalinize, fluids |
References:
- Harrison's Principles of Internal Medicine 22e, Chapter on Nephrolithiasis
- Comprehensive Clinical Nephrology 7e, Chapter 60 (Kidney Stones) and Chapter 61 (Obstructive Uropathy)
- Campbell-Walsh-Wein Urology, Urolithiasis/Upper Tract Endoscopy chapters
- Bailey and Love's Short Practice of Surgery 28e, Chapter 20
- Creasy & Resnik's Maternal-Fetal Medicine, Chapter on Urolithiasis in Pregnancy
- National Kidney Foundation Primer on Kidney Diseases 8e, Chapter on Nephrolithiasis
- Bargagli M et al. Nat Rev Nephrol. 2025 Nov [PMID 40790363]
- Tamborino F et al. Int J Mol Sci. 2024 Mar [PMID 38474319]
- Veronese N et al. Minerva Urol Nephrol. 2025 Aug [PMID 40891477]
This is a shared conversation. Sign in to Orris to start your own chat.