What is anaphylaxis
Reading File
Finding Sources
Searching PubMed
"anaphylaxis"[MeSH Terms] AND "management"[MeSH Terms]
Reading File
Reading File
Reading File
Reading File
Reading File
Reading File
Searching Images
anaphylaxis pathophysiology mechanism diagram
I now have comprehensive information from the textbooks. Let me compile the full answer:
Anaphylaxis
Definition
Anaphylaxis is a severe, acute, and potentially life-threatening systemic hypersensitivity reaction that occurs when mast cells (and possibly basophils) are activated and release potent inflammatory mediators. These mediators exert effects on the vasculature, smooth muscle, mucous glands, and nerves, producing a rapid systemic response. The principal target organs are the cardiovascular, cutaneous, respiratory, and gastrointestinal systems, where mast cells are most abundant. — Goldman-Cecil Medicine
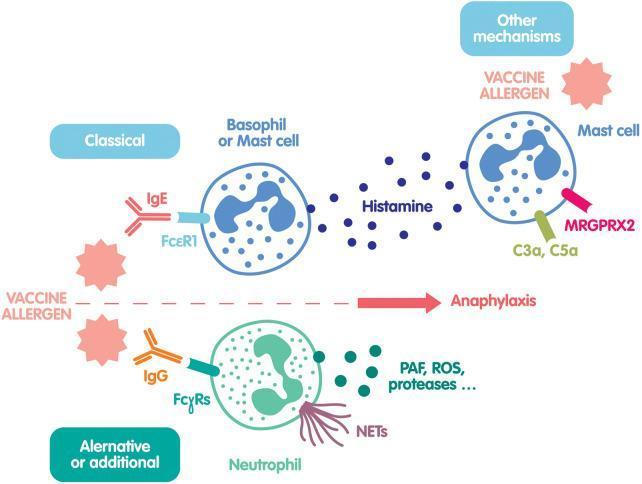
Pathophysiology
The classical mechanism is IgE-mediated (Type I hypersensitivity):
- Sensitization: On first exposure, allergen triggers B-cell production of allergen-specific IgE antibodies
- IgE binding: IgE binds to high-affinity IgE receptors (FcεRI) on mast cells and basophils
- Re-exposure: A subsequent allergen exposure cross-links surface IgE molecules
- Degranulation: Cross-linking triggers mast cell degranulation, releasing:
- Preformed mediators: Histamine, tryptase, heparin
- Newly synthesized mediators: Prostaglandin D₂, leukotriene C₄, platelet-activating factor (PAF)
- Systemic effects: Vasodilation, increased vascular permeability, smooth muscle contraction, mucus secretion
Non-IgE mechanisms also cause anaphylaxis (termed "anaphylactoid" reactions, though now classified together):
- Direct mast cell activation (radiocontrast media, opioids, vancomycin)
- Complement-mediated (C3a/C5a activation)
- NSAIDs — via disruption of arachidonic acid metabolism
Causes / Triggers
| IgE-Mediated | Non-IgE-Mediated |
|---|---|
| Insect stings (Hymenoptera) | Aspirin / NSAIDs |
| Foods: peanut, tree nut, shellfish, milk, egg, soy, mammalian meat (alpha-gal) | Radiocontrast media |
| Drugs: antibiotics (penicillin, cephalosporins) | Opioids |
| Latex | Exercise |
| Allergen extracts (immunotherapy) | Blood products |
Most common triggers: medications (antibiotics, NSAIDs, radiocontrast, chemotherapy agents, monoclonal antibodies), insect stings, and foods. — Goldman-Cecil Medicine
Risk Factors
For developing anaphylaxis:
- Atopy (genetic predisposition to allergic disease)
- Prior sensitization / previous anaphylaxis episode
- Parenteral > oral drug administration
- Summer/fall season (outdoor allergen exposure)
For severe/fatal reactions:
- Extremes of age (infants, elderly)
- Poorly controlled asthma
- Cardiovascular disease
- Mastocytosis or hereditary α-tryptasemia
- Concurrent use of β-blockers (impair epinephrine response) or ACE inhibitors
- Delayed epinephrine administration — the single most important modifiable risk factor
- Upright posture at onset
— Rosen's Emergency Medicine
Clinical Features
Anaphylaxis typically presents within minutes of exposure (the faster the onset, the more severe the reaction). Symptoms involve multiple organ systems:
| Organ System | Symptoms & Signs |
|---|---|
| Skin | Urticaria, flushing, pruritus (often scalp/palms), angioedema |
| Respiratory | Bronchospasm (wheeze, dyspnoea), laryngeal edema (stridor, hoarseness), rhinorrhoea |
| Cardiovascular | Hypotension, tachycardia, arrhythmia, circulatory collapse |
| GI | Nausea, vomiting, diarrhoea, abdominal cramping |
| Neurological | Anxiety, sense of impending doom, dizziness, syncope |
Skin manifestations occur in ~90% of cases and are often the first sign. Biphasic reactions (recurrence 1–72 hours after apparent resolution) occur in ~5–20% of cases.
Diagnosis
Anaphylaxis is a clinical diagnosis. The NIAID/FAAN diagnostic criteria require one of three scenarios:
- Acute onset of skin/mucosal symptoms plus respiratory compromise OR hypotension/organ dysfunction
- Two or more systems involved (skin, respiratory, CVS, GI) after likely allergen exposure
- Hypotension after exposure to a known allergen for that patient
Laboratory tests (not for acute management, but useful later):
- Serum tryptase: Elevated within 1–3 hours of onset; supports mast cell activation. May be normal in food-induced anaphylaxis.
- Allergen-specific IgE testing (skin prick tests or serum IgE) — done after recovery
- IgE anti-alpha-gal (for mammalian meat/tick bite allergy)
Management
Immediate (First-Line)
Epinephrine is the sole first-line treatment. Every other intervention is secondary.
-
Epinephrine (adrenaline) IM into the lateral thigh (vastus lateralis):
- Adults: 0.3–0.5 mg (1 mg/mL concentration), repeat every 5–10 minutes as needed
- Children: 0.01 mg/kg (1:1000 concentration), max 0.5 mg
- IM thigh achieves peak plasma concentration in ~8 minutes vs. 34 minutes for subcutaneous route
- ~30% of patients require more than one dose
-
Remove the trigger (remove stinger, stop IV infusion)
-
Position: supine + legs elevated (if hypotensive); left lateral decubitus (if pregnant)
-
IV access, cardiac monitoring, pulse oximetry, supplemental oxygen
Airway Management
- High-flow O₂; early intubation if laryngeal edema is imminent
- Be prepared for surgical airway (cricothyrotomy) if intubation fails
Volume Resuscitation
- Large volumes of IV crystalloid (e.g., 1–2 L bolus) for hypotension refractory to epinephrine
Secondary (Adjunctive — Not First-Line)
- Antihistamines (H1 blocker: diphenhydramine; H2 blocker: ranitidine) — relieve skin symptoms, do not prevent cardiovascular collapse
- Corticosteroids (methylprednisolone IV) — may reduce biphasic reactions; no proven benefit in acute phase
- Glucagon — for patients on β-blockers who are refractory to epinephrine (0.1 mg/kg IV bolus)
- Vasopressors (noradrenaline, dopamine) — for refractory shock
Observation
Minimum 4–6 hours observation after resolution; longer (12–24 hours) for severe reactions due to biphasic risk.
Discharge
- Prescription of self-injectable epinephrine (e.g., EpiPen) for all patients
- Allergy/immunology referral
- Medical alert identification
- Education on trigger avoidance
Epidemiology
- Lifetime incidence: 2–8% in adults; higher in children (food allergy more common)
- ~1,500–2,000 deaths per year in the United States
- ~50% of reactions occur at home; ~15% in medical facilities
- Fatal anaphylaxis is rare (<1% of cases), but increasing in frequency
Key teaching point: The most common cause of anaphylaxis death is delayed or failure to administer epinephrine — antihistamines and steroids are adjuncts and must never substitute for epinephrine. — Rosen's Emergency Medicine, Goldman-Cecil Medicine, Andrews' Diseases of the Skin
This is a shared conversation. Sign in to Orris to start your own chat.