Teach me anti depressent fron basic to research
Reading File
Finding Sources
Finding Sources
Searching PubMed
"antidepressant" AND "mechanism" AND "treatment"
Finding Sources
Finding Sources
Reading File
Reading File
Reading File
Reading File
Finding Sources
Finding Sources
Reading File
Reading File
Reading File
Reading File
Reading File
Reading File
Loading Image
Loading Image
I now have everything needed to write a comprehensive, textbook-quality guide on antidepressants. Here it is:
Antidepressants: From Basics to Research
Sources: Katzung's Basic and Clinical Pharmacology 16e, Stahl's Essential Psychopharmacology, Kaplan & Sadock's Comprehensive Textbook of Psychiatry, Harrison's 22e, The Maudsley Prescribing Guidelines 15e
PART 1 - UNDERSTANDING DEPRESSION (The "Why" Before the "What")
What is Depression?
Major Depressive Disorder (MDD) is not just "feeling sad." Per DSM-5, a major depressive episode requires at least 5 of the following symptoms for 2+ weeks, with at least one being depressed mood OR anhedonia (loss of interest):
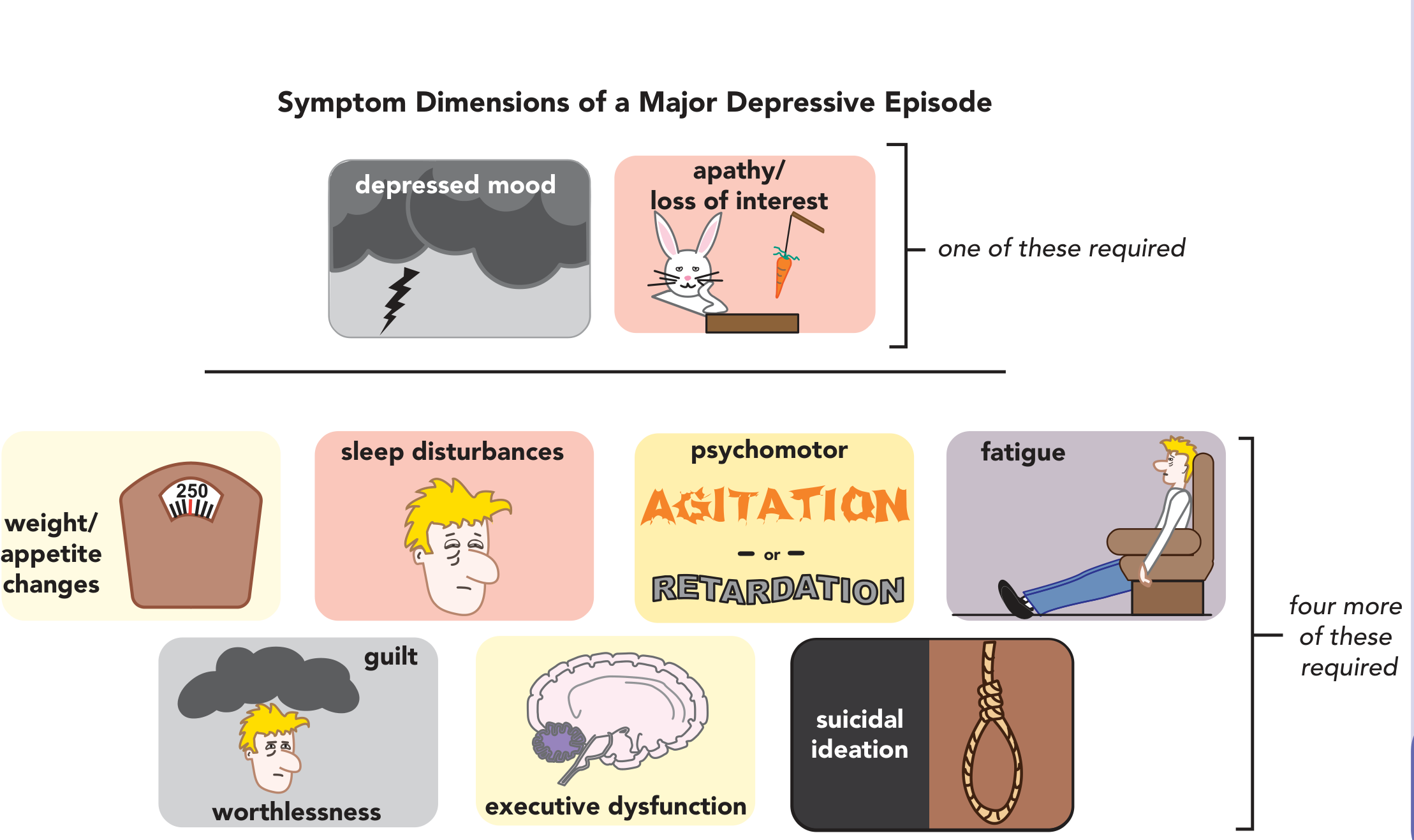
- Depressed mood most of the day
- Loss of interest or pleasure (anhedonia)
- Sleep disturbances (insomnia or hypersomnia)
- Weight/appetite changes
- Psychomotor agitation or retardation
- Fatigue or loss of energy
- Feelings of guilt or worthlessness
- Executive dysfunction / poor concentration
- Suicidal ideation
About 85% of patients who have a single episode of MDD will have at least one recurrence in their lifetime. - Katzung's, p. 851
PART 2 - PATHOPHYSIOLOGY (The Neuroscience)
The Monoamine Hypothesis
The dominant (though incomplete) theory of depression centers on three monoamine neurotransmitters:
| Monoamine | Synthesis | Transporter | Linked Symptoms if Deficient |
|---|---|---|---|
| Serotonin (5-HT) | Tryptophan → 5-HTP → 5-HT | SERT | Mood, anxiety, sleep, appetite |
| Norepinephrine (NE) | Tyrosine → DOPA → NE | NET | Energy, concentration, alertness |
| Dopamine (DA) | Tyrosine → DOPA → DA | DAT | Motivation, reward, pleasure |
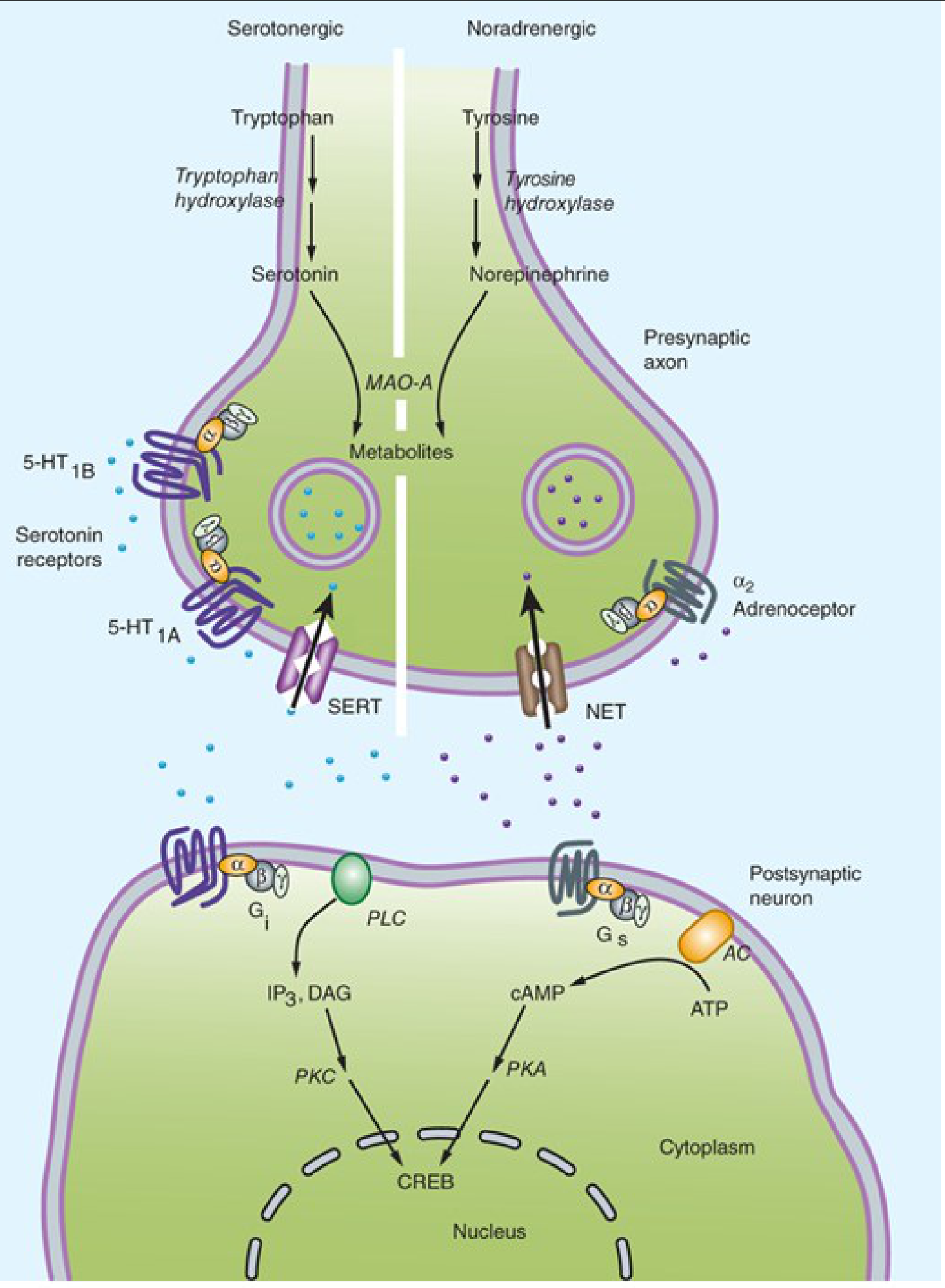
The diagram above shows serotonin (left) and norepinephrine (right) synapses. Both are synthesized from amino acids, released into the synapse, and recaptured via SERT and NET transporters. MAO-A breaks them down inside the neuron. Antidepressants work primarily by blocking SERT/NET or MAO-A. - Katzung's, p. 836
Evidence for the monoamine hypothesis:
- Reserpine (depletes monoamines) causes depression in a subset of patients
- Tryptophan-free diets cause rapid relapse in patients responding to serotonergic antidepressants
- A functional polymorphism in the SERT gene promoter (short "s" allele) increases vulnerability to depression under stress and reduces SSRI response
- All currently available antidepressants enhance synaptic monoamine availability - this is the strongest indirect evidence
Beyond Monoamines
The monoamine hypothesis is incomplete. Key evidence:
- Monoamine changes happen within hours, but antidepressant effects take 2-4 weeks - suggesting downstream changes matter more
- The neurotrophic hypothesis: antidepressants upregulate BDNF (Brain-Derived Neurotrophic Factor), which promotes neuroplasticity and neurogenesis in the hippocampus
- The neuroplasticity/neuroprogression hypothesis (Stahl's): depression is associated with progressive structural changes in the brain; effective treatment may halt or reverse this
- The NMDA/glutamate hypothesis (newer): ketamine's rapid antidepressant effect via NMDA receptor blockade points to glutamate as a critical player
PART 3 - CLASSIFICATION OF ANTIDEPRESSANTS
Here are all major classes, organized from first-line to specialized:
CLASS 1: SSRIs - Selective Serotonin Reuptake Inhibitors
Mechanism: Block SERT → increase synaptic serotonin. Very selective - minimal effects on other receptors.
Drugs: Fluoxetine, Sertraline, Paroxetine, Citalopram, Escitalopram, Fluvoxamine
| Drug | Key Features |
|---|---|
| Fluoxetine | Longest half-life (active metabolite norfluoxetine ~3x longer); needs 4-week washout before MAOI; inhibits CYP2D6 |
| Sertraline | Fewest drug interactions; preferred in cardiac patients; safest in pregnancy |
| Paroxetine | Highest sexual dysfunction; strongly anticholinergic; significant CYP2D6 inhibition; most discontinuation syndrome |
| Escitalopram | Most selective SSRI; fewest side effects; slight QTc prolongation risk |
| Citalopram | Dose-dependent QTc prolongation (max 40 mg); avoid in cardiac disease |
| Fluvoxamine | Used mainly for OCD; inhibits CYP3A4 and CYP1A2 |
Uses: MDD, all major anxiety disorders (PTSD, OCD, social anxiety, GAD, panic disorder), PMDD, eating disorders
Side effects: GI upset (nausea, diarrhea), sexual dysfunction (reduced libido, anorgasmia), insomnia/agitation, weight gain (long-term), discontinuation syndrome (especially paroxetine), serotonin syndrome risk
Critical safety: Risk of serotonin syndrome if combined with MAOIs, tramadol, triptans, linezolid - Katzung's, p. 855
CLASS 2: SNRIs - Serotonin-Norepinephrine Reuptake Inhibitors
Mechanism: Block both SERT and NET. Unlike TCAs, minimal affinity for other receptors (histamine, muscarinic, alpha-1).
Drugs: Venlafaxine, Desvenlafaxine, Duloxetine, Levomilnacipran, Milnacipran
| Drug | Key Features |
|---|---|
| Venlafaxine | At low doses = SSRI-like; NE effects emerge at higher doses; dose-dependent BP elevation; lowest protein binding |
| Desvenlafaxine | Active metabolite of venlafaxine; 45% excreted unchanged in urine; fewer drug interactions |
| Duloxetine | Strong evidence for pain (diabetic neuropathy, fibromyalgia, musculoskeletal); 97% protein bound; hepatotoxicity risk |
| Milnacipran | Greater NE selectivity; approved for fibromyalgia (not depression) in USA |
| Levomilnacipran | Approved for MDD; predominantly NE reuptake inhibition |
Uses: MDD, all anxiety disorders, pain syndromes (duloxetine), fibromyalgia, stress urinary incontinence (duloxetine)
SNRIs bind SERT and NET as do TCAs, but unlike TCAs do not have much affinity for other receptors. - Katzung's, p. 840
CLASS 3: TCAs - Tricyclic Antidepressants
Mechanism: Block both SERT and NET (like SNRIs) BUT also block: H1 (antihistamine → sedation), muscarinic (anticholinergic effects), alpha-1 adrenergic (orthostatic hypotension), and sodium channels (cardiac toxicity in overdose).
Drugs: Imipramine, Amitriptyline, Clomipramine, Desipramine, Nortriptyline, Doxepin, Trimipramine, Protriptyline, Amoxapine
| Drug | Profile |
|---|---|
| Imipramine | Prototype; balanced 5-HT + NE; highly anticholinergic |
| Desipramine | Less anticholinergic; more selective for NE; better tolerated |
| Amitriptyline | Very sedating; strong anticholinergic; used for chronic pain, migraine prevention |
| Clomipramine | Most serotonergic TCA; first-line for OCD |
| Nortriptyline | Best tolerated TCA; least orthostatic hypotension; preferred in elderly |
Uses now: Depression unresponsive to SSRIs/SNRIs, chronic pain (neuropathic, fibromyalgia), migraine prophylaxis, enuresis (imipramine), insomnia
Loss of popularity is due to poorer tolerability, difficult dosing, and extreme lethality in overdose (as little as 10x daily dose can be fatal - cardiac arrhythmias from Na-channel blockade). - Katzung's, p. 841
Anticholinergic side effects: Dry mouth, constipation, urinary retention, blurred vision, cognitive impairment, tachycardia - contraindicated in BPH, narrow-angle glaucoma.
CLASS 4: MAOIs - Monoamine Oxidase Inhibitors
Mechanism: Inhibit MAO-A (degrades 5-HT and NE) and/or MAO-B (degrades DA), increasing all three monoamines.
Drugs:
- Phenelzine - irreversible, non-selective (MAO-A + B); oral
- Tranylcypromine - irreversible, non-selective; oral; stimulant-like
- Isocarboxazid - irreversible, non-selective; oral
- Selegiline - selective MAO-B at low doses, becomes non-selective at antidepressant doses; available as transdermal patch (avoids dietary tyramine restriction at lowest dose)
Critical interactions:
- Tyramine crisis ("cheese reaction"): Normally, gut MAO-A breaks down tyramine in aged cheese, wine, cured meats. MAOIs block this → tyramine floods circulation → hypertensive crisis. Patients must follow a tyramine-restricted diet.
- Serotonin syndrome: Cannot combine with any serotonergic drug (SSRIs, SNRIs, TCAs, triptans, meperidine, tramadol). Washout period: 14 days after stopping MAOI before starting another serotonergic drug; 14 days after stopping most SSRIs, but 5 weeks after stopping fluoxetine (due to long half-life of norfluoxetine).
Use: Atypical depression, treatment-resistant depression, social anxiety disorder. Third or fourth line due to dangerous interactions.
CLASS 5: Atypical / Newer Antidepressants
5-HT2 Receptor Modulators
- Trazodone: 5-HT2 antagonist + weak SERT inhibitor. Highly sedating. Rarely used as antidepressant - now used primarily as a hypnotic (off-label). Risk of priapism. No dependence/tolerance. - Katzung's, p. 841
- Nefazodone: Related to trazodone. Black box warning for hepatotoxicity (lethal hepatic failure reported). Rarely prescribed.
Tetracyclic/Unicyclic
- Bupropion: Unicyclic aminoketone. Unique mechanism - inhibits DAT and NET (dopamine + norepinephrine reuptake). No sexual dysfunction. No weight gain. Lowers seizure threshold (dose-dependent). Used for MDD, smoking cessation, ADHD. Contraindicated in eating disorders and seizure history. Resembles amphetamine structurally.
- Mirtazapine: Alpha-2 adrenergic antagonist (increases NE/5-HT release) + blocks 5-HT2 and 5-HT3 + strong H1 antagonist. Very sedating. Significant weight gain. Good for depression with insomnia, weight loss, or severe nausea. "NaSSA" = noradrenergic and specific serotonergic antidepressant.
- Vilazodone: SSRI + 5-HT1A partial agonist. Minimal weight gain and sexual dysfunction.
- Vortioxetine: Multimodal - SERT inhibitor + 5-HT3/5-HT7/5-HT1D antagonist + 5-HT1B partial agonist + 5-HT1A agonist. Evidence for improving cognitive dysfunction associated with depression. Not simply classified as SSRI. - Katzung's, p. 842
PART 4 - PHARMACODYNAMICS SUMMARY
All antidepressants enhance monoamine neurotransmission by one of these mechanisms:
| Mechanism | Drug Classes |
|---|---|
| Block SERT | SSRIs, SNRIs, TCAs |
| Block NET | SNRIs, TCAs, bupropion |
| Block DAT | Bupropion |
| Inhibit MAO | MAOIs |
| Block presynaptic alpha-2 autoreceptors (increase NE/5-HT release) | Mirtazapine |
| Block postsynaptic 5-HT2 receptors | Trazodone, nefazodone, mirtazapine |
| Multimodal serotonin effects | Vortioxetine, vilazodone |
| NMDA antagonism | Ketamine, esketamine |
| GABA-A positive modulation | Brexanolone, zuranolone |
The cascade from increased monoamine availability → upregulation of BDNF, glucocorticoid receptors, beta-adrenoreceptors → altered gene transcription via CREB is what likely determines the delayed 2-4 week clinical response. - Katzung's, p. 848
PART 5 - PHARMACOKINETICS
Key principles:
- Most antidepressants are highly protein bound (except venlafaxine/desvenlafaxine at 27-30%)
- Most undergo hepatic CYP450 metabolism
- Fluoxetine + paroxetine: potent CYP2D6 inhibitors (many drug interactions)
- Fluvoxamine: potent CYP3A4 + CYP1A2 inhibitor
- Citalopram/escitalopram/sertraline: modest CYP interactions - preferred when polypharmacy is a concern
- Fluoxetine has the longest half-life (norfluoxetine t1/2 ~5-7 days) - least discontinuation syndrome, slowest washout needed before MAOI
PART 6 - CLINICAL USE
When to Use Which Drug
| Situation | Preferred Drug |
|---|---|
| First episode MDD | Any SSRI (sertraline, escitalopram most used) |
| MDD + anxiety | SSRI or SNRI |
| MDD + pain (neuropathic, fibromyalgia) | Duloxetine or TCA |
| MDD + insomnia | Mirtazapine, trazodone add-on |
| MDD + smoking cessation | Bupropion |
| MDD + sexual dysfunction concern | Bupropion, mirtazapine, vortioxetine |
| MDD + weight gain concern | Bupropion |
| Atypical depression | MAOIs (phenelzine) or SSRIs |
| OCD | Clomipramine, SSRIs (high dose, longer duration) |
| PTSD | Sertraline, paroxetine (FDA approved) |
| Panic disorder | Paroxetine, sertraline, venlafaxine |
| Postpartum depression | Sertraline (first-line), brexanolone (IV, rapid) |
Duration of Treatment
- Acute phase: 6-12 weeks (assess response)
- Continuation phase: 4-9 months after remission (prevents relapse)
- Maintenance: Long-term if 2+ serious MDD episodes in 5 years, or 3+ lifetime episodes - Katzung's, p. 851
Bipolar Depression - Important Warning
Antidepressants in bipolar disorder may precipitate mania or rapid cycling even when combined with mood stabilizers. Antidepressant monotherapy is generally not recommended in bipolar depression. - Katzung's, p. 851
PART 7 - SIDE EFFECTS COMPARISON
| Drug Class | Sexual Dysfunction | Weight Gain | Sedation | Anticholinergic | Cardiac Risk |
|---|---|---|---|---|---|
| SSRIs | High | Mild | Low | None | Low |
| SNRIs | Moderate | Mild | Low | None | Low |
| TCAs | Moderate | High | High | High | High (overdose) |
| MAOIs | Moderate | Moderate | Variable | Low | Hypertensive crisis |
| Bupropion | None | None | Low (activating) | None | Low |
| Mirtazapine | Low | High | High | Low | Low |
| Trazodone | Low (priapism risk) | Low | High | Low | Low |
From Kaplan & Sadock's side effect comparison table:
- Paroxetine has the highest sexual dysfunction among SSRIs
- Bupropion has no anticholinergic or sexual side effects
- Citalopram has the most QTc prolongation among SSRIs
PART 8 - SEROTONIN SYNDROME
A potentially life-threatening toxicity from excess serotonergic activity.
Triad: Hyperthermia + Neuromuscular abnormalities (clonus, hyperreflexia, tremor) + Altered mental status
Causes: MAOI + SSRI; SSRI + tramadol; SSRI + linezolid; SSRI + triptans; overdose
Treatment: Discontinue offending drugs, cyproheptadine (5-HT2 antagonist), supportive care, benzodiazepines for agitation
PART 9 - NOVEL AND RESEARCH-FRONTIER TREATMENTS
Ketamine and Esketamine (NMDA Antagonists)
The most significant advance in antidepressant pharmacology in decades:
- Racemic IV ketamine (off-label): produces antidepressant effects within hours - vs. weeks for conventional drugs
- Esketamine (Spravato) intranasal: FDA-approved for Treatment-Resistant Depression (TRD) and for depression with acute suicidal ideation
- Mechanism: NMDA receptor (glutamate) blockade, rapid AMPA activation, BDNF release, synaptogenesis
- Esketamine: 48% bioavailable intranasally, t1/2 of 7-12 hours; administered in clinic under observation due to dissociation risk
- Dextromethorphan + Bupropion (Auvelity): FDA-approved 2022; bupropion inhibits CYP2D6 to increase dextromethorphan levels (another NMDA antagonist); faster onset than SSRIs - Katzung's, p. 847
Brexanolone and Zuranolone (GABA-A Modulators)
- Brexanolone (Zulresso): IV neuroactive steroid; positive allosteric modulator of GABA-A; FDA-approved for postpartum depression; 60-hour infusion; 99% protein bound
- Zuranolone (Zurzuvae): Oral version; FDA-approved 2023 for postpartum depression and MDD; rapid onset (days)
- These represent a completely new mechanism - no monoamine involvement
Psilocybin (Research Stage)
- Classical psychedelic; 5-HT2A agonist
- Phase 2/3 trials showing rapid, durable antidepressant effects in treatment-resistant depression
- A 2025 systematic review (PMID: 39788410) explored neurobiological blood biomarker mechanisms
Vortioxetine - Cognitive Enhancement
- 2025 systematic review (PMID: 39808348) confirmed vortioxetine's expanding role in neurological conditions beyond depression, consistent with its cognitive effects
PART 10 - TREATMENT-RESISTANT DEPRESSION (TRD)
Defined as failure of 2+ adequate antidepressant trials (adequate dose for adequate duration).
Strategies:
- Optimize current drug (dose increase, duration check, adherence)
- Switch to different class
- Combine two antidepressants (e.g., SSRI + bupropion, SSRI + mirtazapine)
- Augment: Add lithium, atypical antipsychotics (aripiprazole, quetiapine, brexpiprazole, cariprazine), thyroid hormone
- Ketamine/Esketamine (FDA-approved specifically for TRD)
- ECT (Electroconvulsive Therapy): Most effective treatment for severe/refractory depression; 70-90% response rate
- TMS (Transcranial Magnetic Stimulation): Non-invasive, FDA-approved
PART 11 - THE ANTIDEPRESSANT DELAY PARADOX
One of the most important unresolved questions: Why do antidepressants take 2-4 weeks to work if monoamine levels increase within hours?
Leading explanations:
- Receptor downregulation theory: Initial 5-HT increase activates somatodendritic 5-HT1A autoreceptors, which suppress firing. Over weeks, these autoreceptors desensitize, allowing full 5-HT output.
- Neuroplasticity theory: The therapeutic effect depends on downstream gene expression changes (BDNF, synaptic remodeling), which take weeks.
- Glucocorticoid receptor normalization: Chronic stress causes glucocorticoid receptor resistance; antidepressants gradually restore sensitivity.
Quick Reference Summary
DEPRESSION
↓ 5-HT, NE, DA in synapses
ANTIDEPRESSANT STRATEGIES:
Block reuptake: SSRI → ↑5-HT
SNRI → ↑5-HT + ↑NE
TCA → ↑5-HT + ↑NE + many side effects
Bupropion → ↑DA + ↑NE
Block degradation: MAOI → ↑all three
Receptor modulation: Mirtazapine → ↑NE + ↑5-HT release
Vortioxetine → multimodal 5-HT
Novel targets:
Ketamine/Esketamine → NMDA block → hours
Brexanolone/Zuranolone → GABA-A modulation
Psilocybin → 5-HT2A agonism (research)
Sources:
- Katzung's Basic and Clinical Pharmacology 16e, Chapter 30 (Antidepressant Agents)
- Stahl's Essential Psychopharmacology, Chapter 6 (Mood Disorders) and Chapter 7 (Antidepressants)
- Kaplan & Sadock's Comprehensive Textbook of Psychiatry
- The Maudsley Prescribing Guidelines 15e
- Harrison's Principles of Internal Medicine 22e
Teach me antidepressant from basic to research
I just completed a comprehensive, textbook-sourced guide on this exact topic in my previous response. Here is the full structured lesson again for easy reference:
Antidepressants: From Basics to Research
Sources: Katzung's Basic & Clinical Pharmacology 16e, Stahl's Essential Psychopharmacology, Kaplan & Sadock's Comprehensive Textbook of Psychiatry, Harrison's 22e, Maudsley Prescribing Guidelines 15e
PART 1 - UNDERSTANDING DEPRESSION (The Foundation)
Before understanding antidepressants, you need to understand what they treat.
DSM-5 Criteria for Major Depressive Episode
Requires 5+ symptoms for 2+ weeks, with at least one being depressed mood OR anhedonia (loss of interest/pleasure):
- Depressed mood most of the day
- Anhedonia - loss of interest or pleasure
- Sleep disturbance (insomnia or hypersomnia)
- Weight/appetite change
- Psychomotor agitation or retardation
- Fatigue or loss of energy
- Feelings of guilt or worthlessness
- Poor concentration / executive dysfunction
- Suicidal ideation
About 85% of patients with a single MDD episode will have at least one recurrence. Many progress to chronic, treatment-resistant episodes. - Katzung's, p. 851
PART 2 - NEUROSCIENCE OF DEPRESSION
The Monoamine Hypothesis
The central theory of depression: deficiency or dysregulation of three monoamine neurotransmitters in key brain circuits.
| Monoamine | Precursor | Transporter | Degrading Enzyme | Linked Symptoms When Low |
|---|---|---|---|---|
| Serotonin (5-HT) | Tryptophan | SERT | MAO-A | Mood, anxiety, sleep, appetite, impulsivity |
| Norepinephrine (NE) | Tyrosine | NET | MAO-A | Energy, concentration, alertness, drive |
| Dopamine (DA) | Tyrosine | DAT | MAO-B | Motivation, reward, pleasure, anhedonia |
This diagram shows both serotonin (left) and norepinephrine (right) synapses. Monoamines are synthesized from amino acids, released into the synapse, and recaptured via SERT/NET. MAO-A degrades them intraneuronally. Antidepressants block SERT/NET or MAO-A to increase synaptic availability. Downstream signaling via PKA/PKC converges on CREB - the transcription factor driving neuroplastic gene expression. - Katzung's, p. 836
Key evidence supporting the monoamine hypothesis:
- Reserpine (depletes monoamines) causes depression in a subset of patients
- Tryptophan-free diet causes rapid relapse in patients responding to serotonergic antidepressants
- Catecholamine depletion triggers relapse in patients on noradrenergic agents
- SERT gene promoter polymorphism: The "s" (short) allele → more vulnerable to depression under stress, less likely to respond to SSRIs. The "l" (long) allele → stress-resistant, better SSRI response
- Every antidepressant discovered so far has significant monoamine system effects - Katzung's, p. 837-838
The Delayed Response Paradox
Monoamine levels rise within hours of taking an antidepressant. Clinical benefits take 2-4 weeks. Why?
- Autoreceptor desensitization theory: Initial 5-HT surge activates inhibitory 5-HT1A somatodendritic autoreceptors, dampening firing. Over weeks these desensitize, allowing full output.
- Neurotrophic/BDNF theory: The real therapeutic effect depends on downstream upregulation of BDNF (Brain-Derived Neurotrophic Factor), hippocampal neurogenesis, and synaptic remodeling - these take weeks.
- Glucocorticoid receptor theory: Chronic stress impairs glucocorticoid receptor sensitivity; antidepressants gradually restore this.
Beyond Monoamines
The monoamine hypothesis is incomplete:
- Neuroplasticity hypothesis (Stahl's): Depression involves progressive structural brain changes (hippocampal atrophy, reduced synaptic density). Antidepressants may arrest or reverse neuroprogression if started early.
- Glutamate/NMDA hypothesis: Ketamine's near-instant antidepressant effect via NMDA receptor blockade opened an entirely new understanding - glutamate dysregulation may be a core driver.
- Neuroinflammation hypothesis: Elevated pro-inflammatory cytokines (IL-6, TNF-α, CRP) correlate with depression, especially treatment-resistant forms. Some antidepressants have anti-inflammatory properties.
PART 3 - COMPLETE CLASSIFICATION OF ANTIDEPRESSANTS
CLASS 1: SSRIs (Selective Serotonin Reuptake Inhibitors)
Mechanism: Selectively block SERT → increased synaptic serotonin. Minimal affinity for other receptors = fewer side effects than older agents.
The Six SSRIs:
| Drug | Half-life | Key Pharmacokinetics | Standout Feature |
|---|---|---|---|
| Fluoxetine | 1-4 days (norfluoxetine: ~10 days) | Active metabolite norfluoxetine; strong CYP2D6 inhibitor | Longest half-life; needs 5-week washout before MAOI |
| Sertraline | 26 hours | Modest CYP interactions | Best overall tolerability and drug interaction profile; first choice in cardiac patients, pregnancy |
| Paroxetine | 21 hours | Strong CYP2D6 inhibitor; anticholinergic | Highest sexual dysfunction; worst discontinuation syndrome; most anticholinergic of all SSRIs |
| Citalopram | 35 hours | Modest CYP interactions | Dose-dependent QTc prolongation (max 40 mg/day); avoid in cardiac disease |
| Escitalopram | 27-32 hours | S-enantiomer of citalopram | Most selective SSRI; fewest side effects; slight QTc risk |
| Fluvoxamine | 15 hours | Potent CYP1A2 + CYP3A4 inhibitor | Used mainly for OCD; multiple drug interactions |
Indications: MDD, all anxiety disorders (GAD, PTSD, OCD, social anxiety, panic disorder), PMDD, bulimia nervosa (fluoxetine only, FDA-approved)
Side effects:
- GI: nausea, diarrhea (most common at initiation - usually resolves in 1-2 weeks)
- Sexual dysfunction: reduced libido, delayed orgasm, anorgasmia (30-40% of patients - often persists)
- CNS: insomnia/agitation or sedation (drug-dependent), headache
- Weight gain: minimal short-term; can be significant long-term
- Discontinuation syndrome (especially paroxetine, venlafaxine): flu-like symptoms, "brain zaps," dizziness on abrupt cessation - always taper
Critical danger - Serotonin Syndrome: excess serotonin → triad of hyperthermia + neuromuscular abnormalities (clonus, hyperreflexia) + altered mental status. Triggered by MAOI + SSRI, SSRI + tramadol/meperidine, SSRI + linezolid, SSRI + triptans.
CLASS 2: SNRIs (Serotonin-Norepinephrine Reuptake Inhibitors)
Mechanism: Block both SERT and NET. Unlike TCAs, no significant binding to histaminic, muscarinic, or alpha-1 adrenergic receptors.
| Drug | 5-HT:NE Selectivity | Half-life | Key Notes |
|---|---|---|---|
| Venlafaxine | At low doses: SSRI-like; NE at >150 mg/day | 8-11 hours | Dose-dependent BP elevation; lowest protein binding (27%); XR formulation for once-daily dosing |
| Desvenlafaxine | Balanced | 11 hours | Active metabolite of venlafaxine; 45% excreted unchanged in urine; fewer drug interactions |
| Duloxetine | Balanced | 12-15 hours | Best evidence for pain (diabetic neuropathy, fibromyalgia, musculoskeletal pain); 97% protein bound; hepatotoxicity risk - avoid in liver disease |
| Levomilnacipran | NE > 5-HT | 12 hours | More NE-selective; approved for MDD |
| Milnacipran | NE >> 5-HT | 6-8 hours | Approved for fibromyalgia in USA (not for depression) |
SNRIs bind the serotonin and norepinephrine transporters as do TCAs, but unlike TCAs do not have significant affinity for other receptors. - Katzung's, p. 840
Advantages over SSRIs: Potentially more effective for severe depression (dual mechanism), better for pain comorbidity, venlafaxine approved for all major anxiety disorders.
CLASS 3: TCAs (Tricyclic Antidepressants)
Mechanism: Block SERT + NET (like SNRIs) + histamine H1 + muscarinic receptors + alpha-1 adrenergic + sodium channels (cardiac toxicity).
All share a three-ring (tricyclic) iminodibenzyl core. Subtle chemical differences create large pharmacological differences.
| Drug | Relative 5-HT:NE | Anticholinergic | Sedation | Notes |
|---|---|---|---|---|
| Imipramine | Balanced | High | Moderate | Prototype; also used for enuresis |
| Amitriptyline | 5-HT > NE | Very high | Very high | Migraine prophylaxis; neuropathic pain |
| Clomipramine | 5-HT dominant | High | High | Most serotonergic TCA; first-line for OCD |
| Desipramine | NE dominant | Low | Low | Best tolerated TCA; least anticholinergic |
| Nortriptyline | NE > 5-HT | Moderate | Moderate | Preferred in elderly; least orthostatic hypotension; therapeutic window 50-150 ng/mL |
| Doxepin | Low | Very high | Very high | Low dose approved for insomnia (H1 antagonism) |
Current uses: TCA use has been largely replaced by SSRIs/SNRIs. Used now for:
- Treatment-resistant depression (failed SSRIs/SNRIs)
- Chronic neuropathic pain
- Migraine prevention
- Enuresis (imipramine)
- Insomnia (doxepin low dose)
Contraindications: Recent MI, cardiac arrhythmias, BPH, narrow-angle glaucoma, active suicidality (lethal in overdose - sodium channel blockade → QRS widening, ventricular arrhythmias, death at 10x therapeutic dose)
CLASS 4: MAOIs (Monoamine Oxidase Inhibitors)
Mechanism: Inhibit MAO enzyme → less monoamine degradation → more 5-HT, NE, and DA available in neurons and synapses.
| Isoform | Substrates | Location |
|---|---|---|
| MAO-A | Serotonin, NE, tyramine | Gut, liver, neurons |
| MAO-B | Dopamine, tyramine | Brain, platelets |
| Drug | Selectivity | Reversibility | Notes |
|---|---|---|---|
| Phenelzine | Non-selective | Irreversible | Oral; most sedating; used for atypical depression |
| Tranylcypromine | Non-selective | Irreversible | Oral; stimulant-like (structurally related to amphetamine) |
| Isocarboxazid | Non-selective | Irreversible | Oral; rarely used |
| Selegiline | MAO-B selective (low dose); non-selective (high/antidepressant dose) | Irreversible | Transdermal patch at lowest dose (6 mg/day) avoids first-pass gut MAO-A → no dietary tyramine restriction needed at that dose |
The Tyramine Crisis ("Cheese Reaction"):
Normally, MAO-A in the gut and liver destroys ingested tyramine (found in aged cheese, wine, cured meats, fermented foods). On oral MAOIs, this protective mechanism is gone. Tyramine floods circulation → massive NE release → hypertensive crisis (severe headache, BP >200/120, can cause stroke, MI, death). Patients require strict dietary restriction.
Drug Interactions (life-threatening):
- Cannot combine with any serotonergic drug → serotonin syndrome
- Cannot combine with sympathomimetics (amphetamine, cocaine, ephedrine) → hypertensive crisis
- Cannot combine with meperidine → fatal interaction (serotonin syndrome + respiratory depression)
- Washout: Stop MAOI 14 days before starting SSRI. Stop fluoxetine 5 weeks before starting MAOI.
Use: Atypical depression (hypersomnia, hyperphagia, mood reactivity, rejection sensitivity), treatment-resistant depression, social anxiety. Third or fourth-line due to interactions.
CLASS 5: Atypical Antidepressants
Bupropion (Wellbutrin, Zyban)
- Mechanism: Inhibits DAT and NET (dopamine + norepinephrine reuptake inhibitor). No serotonergic activity.
- Unique advantages: No sexual dysfunction. No weight gain (often weight-neutral or slight loss). No anticholinergic effects.
- Additional uses: Smoking cessation (Zyban), ADHD, seasonal affective disorder
- Side effects: Insomnia, agitation, dry mouth, dose-dependent seizures (contraindicated in eating disorders - electrolyte disturbances lower seizure threshold; avoid in seizure history)
- Note: Resembles amphetamine structurally; activating rather than sedating
Mirtazapine (Remeron)
- Mechanism: Alpha-2 adrenergic antagonist (blocks presynaptic autoreceptors → increases NE and 5-HT release) + blocks 5-HT2 and 5-HT3 receptors + potent H1 antagonist (sedation and appetite)
- NaSSA: noradrenergic and specific serotonergic antidepressant
- Advantages: Good for depression with insomnia, poor appetite, weight loss, nausea, or severe anxiety
- Side effects: Significant sedation and weight gain; low sexual dysfunction
Trazodone
- Mechanism: 5-HT2A antagonist + weak SERT inhibitor
- Primary use now: Off-label hypnotic - very sedating, no tolerance or dependence risk. Rarely used as primary antidepressant.
- Unique risk: Priapism (prolonged erection - up to 1 in 6,000 male patients)
Nefazodone
- Related to trazodone. Black box warning: rare but fatal hepatotoxicity. Rarely prescribed.
Vilazodone (Viibryd)
- SSRI + 5-HT1A partial agonist
- Minimal weight gain and sexual dysfunction
- Requires food for adequate absorption
Vortioxetine (Trintellix)
- Multimodal: SERT inhibitor + 5-HT3/5-HT7/5-HT1D antagonist + 5-HT1B partial agonist + 5-HT1A agonist
- Not simply an SSRI - actions not primarily from SERT inhibition
- Key advantage: Improves cognitive dysfunction associated with depression (approved for this in Europe and USA)
- FDA-approved for MDD; favorable sexual dysfunction profile
- Katzung's, p. 842
PART 4 - PHARMACODYNAMICS AT A GLANCE
| Mechanism | Classes Using It |
|---|---|
| SERT blockade | SSRIs, SNRIs, TCAs, trazodone (weak), vilazodone, vortioxetine |
| NET blockade | SNRIs, TCAs, bupropion |
| DAT blockade | Bupropion |
| MAO inhibition | MAOIs |
| Alpha-2 antagonism (↑NE/5-HT release) | Mirtazapine |
| 5-HT2 antagonism | Mirtazapine, trazodone, nefazodone |
| NMDA antagonism | Ketamine, esketamine, dextromethorphan |
| GABA-A positive modulation | Brexanolone, zuranolone |
| 5-HT1A partial agonism | Buspirone (adjunct), vilazodone, vortioxetine |
The increased synaptic monoamine availability triggers a cascade: downstream gene transcription via CREB → production of BDNF, glucocorticoid receptors, beta-adrenoreceptors → this protein-level change is what actually determines the therapeutic benefit and the 2-4 week delay. - Katzung's, p. 848
PART 5 - KEY PHARMACOKINETICS
| Drug | Half-life | Protein Binding | CYP Metabolism | Special Note |
|---|---|---|---|---|
| Fluoxetine | 1-4 days (norfluoxetine 7-15 days) | 94% | CYP2D6 inhibitor | Longest half-life; 5-week MAOI washout |
| Sertraline | 26 hours | 99% | Modest | Fewest drug interactions |
| Paroxetine | 21 hours | 94% | Strong CYP2D6 inhibitor | Worst discontinuation syndrome |
| Citalopram | 35 hours | 80% | Modest | QTc prolongation dose-dependent |
| Venlafaxine | 8-11 hours | 27% | CYP2D6 | Lowest protein binding of all antidepressants |
| Duloxetine | 12-15 hours | 97% | CYP2D6, CYP1A2 | Hepatic impairment significantly alters levels |
| Desvenlafaxine | 11 hours | 30% | Conjugation (not CYP) | 45% excreted unchanged in urine |
| Fluoxetine vs Paroxetine | - | - | Both potent CYP2D6 inhibitors | Many drug interactions; avoid polypharmacy |
PART 6 - SIDE EFFECT COMPARISON TABLE
From Kaplan & Sadock's Comprehensive Textbook of Psychiatry:
| Drug | Anticholinergic | Sedation | Orthostatic Hypotension | QTc Prolongation | GI Toxicity | Weight Gain | Sexual Dysfunction |
|---|---|---|---|---|---|---|---|
| Citalopram | None | None | Slight | Moderate | Moderate | Slight | Slight |
| Escitalopram | None | None | Slight | Slight | Slight | Slight | Moderate |
| Fluoxetine | None | None | Low | Slight | Low | None | Moderate |
| Paroxetine | Slight | Slight | Slight | Slight | Slight | Slight | High |
| Sertraline | None | None | Low | Low | None-slow | Low | Moderate |
| Bupropion | None | None | Moderate (IR) | None | Slight | Slight | None |
| Venlafaxine | None | None | None | None | Moderate | Low | Moderate |
| Duloxetine | None | None | Slight | None | Low | Unknown | Slight |
| Mirtazapine | Low | High | Slight | None | Low | High | Low |
PART 7 - CLINICAL DECISION-MAKING
Choosing an Antidepressant
| Clinical Scenario | Best Choice(s) |
|---|---|
| First episode MDD, no special features | Sertraline or escitalopram (best tolerability + evidence) |
| MDD + comorbid anxiety | Any SSRI or SNRI |
| MDD + neuropathic pain / fibromyalgia | Duloxetine, or TCA (amitriptyline) |
| MDD + insomnia, weight loss | Mirtazapine |
| MDD + smoking cessation needed | Bupropion |
| MDD + sexual dysfunction is unacceptable | Bupropion, mirtazapine, vortioxetine |
| MDD + obesity / weight gain concern | Bupropion |
| MDD + cardiac disease | Sertraline (most evidence), avoid TCAs |
| MDD in pregnancy | Sertraline (most safety data) |
| MDD + postpartum (acute) | Brexanolone (IV, rapid) or zuranolone |
| OCD | High-dose SSRI or clomipramine (longest duration - 8-12 weeks before judging) |
| PTSD | Sertraline, paroxetine (only FDA-approved for PTSD) |
| Atypical depression | MAOIs > SSRIs > TCAs |
| Elderly patient | Nortriptyline (if TCA needed), sertraline, escitalopram |
| Bipolar depression | Avoid antidepressants monotherapy; quetiapine, lurasidone, or lamotrigine preferred |
Duration Rules
- Acute phase: 6-12 weeks to assess response (at least 4 weeks at adequate dose before declaring failure)
- Continuation: 4-9 months after achieving remission (prevents relapse)
- Maintenance: Long-term if 2+ serious episodes in 5 years, OR 3+ lifetime episodes - Katzung's, p. 851
Antidepressant Failure / Treatment-Resistant Depression
Defined as failure of 2+ adequate antidepressant trials (adequate dose, adequate duration, confirmed adherence).
Sequential strategies:
- Optimize current drug (dose, duration, adherence check)
- Switch within class (different SSRI) or across class (SSRI → SNRI or bupropion)
- Combine: SSRI + bupropion, SSRI + mirtazapine ("California rocket fuel")
- Augment: Add lithium, atypical antipsychotics (aripiprazole, quetiapine, brexpiprazole), T3 thyroid hormone
- Esketamine (Spravato) - FDA-approved specifically for TRD
- ECT (70-90% response rate - most effective treatment for severe/refractory depression)
- TMS (transcranial magnetic stimulation) - non-invasive, FDA-approved
- Psilocybin-assisted therapy (clinical trials/research)
PART 8 - DANGEROUS DRUG INTERACTIONS
Serotonin Syndrome
| Combination | Risk |
|---|---|
| MAOI + any SSRI/SNRI/TCA | Life-threatening |
| SSRI + tramadol or meperidine | High |
| SSRI + linezolid or methylene blue | High |
| SSRI + triptans (sumatriptan) | Moderate - controversial but FDA warning exists |
| SSRI + high-dose dextromethorphan | Moderate |
Clinical triad: Hyperthermia + Neuromuscular abnormalities (clonus, tremor, hyperreflexia) + Altered consciousness. Treatment: Stop offending agents, cyproheptadine (5-HT2 antagonist), benzodiazepines, supportive care.
MAOI-Specific Interactions
- Tyramine-containing foods → hypertensive crisis
- Sympathomimetics (amphetamine, pseudoephedrine) → hypertensive crisis
- Meperidine → serotonin syndrome + respiratory depression (particularly dangerous)
TCA Overdose
Sodium channel blockade → widened QRS → ventricular arrhythmias, hypotension, seizures, coma. Treatment: IV sodium bicarbonate (alkalinization narrows QRS), supportive care.
CYP2D6 Interactions
Fluoxetine and paroxetine are potent CYP2D6 inhibitors. They can dramatically increase levels of:
- Tricyclic antidepressants
- Antipsychotics (haloperidol, risperidone)
- Opioids (codeine → cannot convert to morphine; tramadol → reduced analgesia)
- Beta-blockers (metoprolol)
- Antiarrhythmics (flecainide, propafenone)
PART 9 - NOVEL TREATMENTS (The Research Frontier)
Ketamine and Esketamine - The Paradigm Shift
The biggest advance in antidepressant pharmacology in 60 years.
Racemic IV Ketamine (off-label):
- NMDA receptor antagonist → rapid glutamate-mediated synaptogenesis
- Antidepressant effects within hours (vs. weeks for SSRIs)
- Single dose can relieve depression for 1-2 weeks
- Used for treatment-resistant depression and acute suicidality
- t1/2 ~3 hours; given as subanesthetic infusion (0.5 mg/kg over 40 min)
Esketamine (Spravato) - FDA-approved 2019:
- S-enantiomer of ketamine; intranasal spray
- 48% bioavailable intranasally; Tmax 20-40 minutes; t1/2 7-12 hours
- Must be administered in a certified clinic under supervision (dissociation, dizziness)
- FDA-approved for: (1) Treatment-Resistant Depression + oral antidepressant, (2) MDD with acute suicidal ideation
- Katzung's, p. 847; The Maudsley Prescribing Guidelines 15e
Dextromethorphan/Bupropion (Auvelity) - FDA-approved 2022:
- Bupropion inhibits CYP2D6 → raises dextromethorphan levels → NMDA antagonist effect
- Oral tablet; faster onset than SSRIs (1-2 weeks)
- t1/2 22 hours; peak in 3 hours
Brexanolone and Zuranolone (Neuroactive Steroids)
Completely new mechanism - no monoamine involvement:
Brexanolone (Zulresso) - FDA-approved 2019:
- IV neuroactive steroid; positive allosteric modulator of GABA-A receptors
- 60-hour continuous IV infusion; must be administered in hospital
- 99% protein bound; t1/2 ~9 hours
- FDA-approved for postpartum depression (PPD)
- Response within 24-48 hours (unprecedented for depression)
Zuranolone (Zurzuvae) - FDA-approved 2023:
- Oral neuroactive steroid (GABA-A modulator)
- 14-day course treatment
- FDA-approved for PPD and MDD
- Rapid onset: significant improvement by Day 3 in some trials
Psilocybin - Active Clinical Research
- 5-HT2A agonist (classical psychedelic)
- Mechanism likely involves rapid synaptogenesis, default mode network reset
- Phase 2/3 trials in treatment-resistant depression, MDD, PTSD, addiction
- FDA granted "Breakthrough Therapy" designation for TRD
- A 2025 systematic review on psilocybin blood biomarker mechanisms (PMID 39788410) is mapping the neurobiological underpinnings
- Not yet FDA-approved for depression (regulatory uncertainty as of 2026)
Vortioxetine - Cognitive Frontier
- 2025 systematic review (PMID 39808348) confirmed expanding neurological applications for vortioxetine, consistent with its well-documented pro-cognitive effects in depression
Other Emerging Targets
| Target | Agent | Stage |
|---|---|---|
| Kappa opioid receptor antagonism | Aticaprant | Phase 3 |
| GLP-1 receptor agonism | Semaglutide (incidental) | Observational evidence |
| Neuroinflammation (IL-6, TNF-α) | Celecoxib augmentation | Phase 2 evidence |
| AMPA potentiation | Multiple compounds | Preclinical-Phase 2 |
| Muscarinic M1/M4 agonism | Xanomeline-trospium (for TRD) | Phase 2 |
PART 10 - THE "BIG PICTURE" SUMMARY
ROOT CAUSE OF DEPRESSION (current understanding):
↓ Synaptic 5-HT, NE, DA + Neuroplasticity failure + HPA axis dysregulation
+ Glutamate dysfunction + Neuroinflammation
↓
HOW ANTIDEPRESSANTS WORK:
BLOCK REUPTAKE:
SSRIs → ↑5-HT (selective)
SNRIs → ↑5-HT + ↑NE
TCAs → ↑5-HT + ↑NE + many side effects
Bupropion → ↑DA + ↑NE
BLOCK DEGRADATION:
MAOIs → ↑5-HT + ↑NE + ↑DA
RECEPTOR MODULATION:
Mirtazapine → ↑NE + ↑5-HT release via alpha-2 blockade
Vortioxetine → multimodal 5-HT (most complex)
Trazodone → 5-HT2 blockade (primarily sedation/hypnotic)
NOVEL MECHANISMS:
Ketamine/Esketamine → NMDA blockade → synaptogenesis → hours
Brexanolone/Zuranolone → GABA-A modulation (postpartum)
Psilocybin → 5-HT2A → circuit reset (research)
↓
DOWNSTREAM (common final pathway):
↑BDNF → Neuroplasticity → Restored hippocampal circuits → Remission
Textbook Sources Used:
- Katzung's Basic and Clinical Pharmacology, 16th Edition - Chapter 30 (Antidepressant Agents)
- Stahl's Essential Psychopharmacology - Chapters 6 & 7
- Kaplan & Sadock's Comprehensive Textbook of Psychiatry
- The Maudsley Prescribing Guidelines in Psychiatry, 15th Edition
- Harrison's Principles of Internal Medicine, 22nd Edition (2025)
This is a shared conversation. Sign in to Orris to start your own chat.