Snek bite poisoning
Reading File
Finding Sources
Searching PubMed
"snake bite" AND "envenomation" AND management
Finding Sources
Finding Sources
Reading File
Reading File
Reading File
Reading File
Reading File
Reading File
Reading File
Reading File
Reading File
Reading File
Reading File
Reading File
Loading Image
Here is a comprehensive overview of snake bite poisoning (envenomation):
Snake Bite Poisoning (Envenomation)
Epidemiology
The WHO estimates 5.4 million snake bites per year worldwide, with 1.8-2.7 million cases of actual envenomation, and between 81,000-138,000 deaths annually - plus 3x as many amputations and permanent disabilities. In the United States, 7,000-8,000 bites occur per year with only about 5-6 deaths. Up to one-third of venomous snake bites are "dry bites" - no venom is injected.
High-quality antivenoms are classified as essential medicines by the WHO.
- Sabiston Textbook of Surgery, p. 751-753
Classification of Venomous Snakes
There are 4 families of venomous snakes worldwide:
| Family | Examples | Primary Toxicity |
|---|---|---|
| Elapidae (incl. Hydrophiinae - sea snakes) | Cobras, kraits, mambas, coral snakes, adders | Predominantly neurotoxic |
| Viperidae (pit vipers & true vipers) | Rattlesnakes, Russell's viper, saw-scaled viper | Hemotoxic/cytotoxic/local tissue damage |
| Colubridae | Boomslang, bird snake | Mostly Africa |
| Atractaspididae | Stiletto snakes | Africa/Middle East |
- Sabiston Textbook of Surgery, p. 753-754
Venom Delivery Mechanism
Venom glands evolved from salivary glands and sit on each side of the head above the maxillae, behind the eyes. Each gland has its own muscle and nerve supply, allowing the snake to control the dose injected. Pit vipers have large, hollow, rotating anterior fangs. Coral snakes have smaller fixed hollow fangs. In Viperids, jaw closure compresses the gland, ejecting venom through the fang tip.
Notably, fang size does not correlate with venom potency - sea snakes (Hydrophids) have tiny fangs but extremely toxic venom. - P C Dikshit Textbook of Forensic Medicine and Toxicology, p. 494
Venom Composition
Venom is over 90% protein by dry weight, consisting of enzymes and toxins:
Key enzymes and their actions:
- Phospholipase A2 - destroys phospholipids in nervous tissue, alters neuromuscular conduction, causes hemolysis
- Hyaluronidase - spreads venom rapidly from bite site (present in ALL snake venoms)
- Proteolytic enzymes / metalloproteinases - tissue destruction, hemorrhage, vascular damage
- L-amino acid oxidase - splits fibrinogen, contributes to DIC
- Cholinesterase (mainly Elapid) - hydrolyzes acetylcholine, impairs neuromuscular transmission
- Hemolysin (mainly Viper) - widespread hemolysis in presence of lecithinase
- Fibrinolysin / Fibrin ferments - coagulation disorders
- Cytolysin - lysis of blood and tissue cells
- Collagenase, Elastase - structural tissue breakdown
- P C Dikshit Textbook of Forensic Medicine and Toxicology, p. 493-495; Sabiston Textbook of Surgery, p. 834-836
Venom Types: Colubrine vs. Viperine
Colubrine Venom (Elapids - cobras, kraits, mambas, sea snakes)
- Predominantly neurotoxic - respiratory and cardiac center paralysis
- Cobra venom causes progressive muscular paralysis: mouth and throat muscles first, then respiratory muscles (curare-like action)
- Krait venom produces muscular paralysis only (no convulsions)
- Components: neurotoxin, cholinesterase, cardiotoxin, phospholipase A
- Local pain and swelling are not usually severe
Viperine Venom (vipers - Russell's viper, Echis, rattlesnakes)
-
Predominantly hemolytic/hemotoxic
-
Cytolysis of vascular endothelium, hemolysis, severe coagulation disorders
-
Severe local: swelling, oozing of blood, spreading cellulitis, necrosis
-
Blood fails to clot even with thrombin (depleted fibrinogen)
-
Causes DIC, renal tubular necrosis
-
P C Dikshit Textbook of Forensic Medicine and Toxicology, p. 494-495
Amounts Injected & Fatal Doses
| Snake | Venom per bite | Fatal dose |
|---|---|---|
| Cobra | 200-250 mg dried | 12-15 mg |
| Viper | 150-200 mg dried | 15-20 mg |
| Krait | 20 mg dried | 5-6 mg |
| Saw-scaled viper | 4.5-5 mg dried | 8 mg |
A cobra can inject ~40x the fatal dose in a single bite.
- P C Dikshit Textbook of Forensic Medicine and Toxicology, p. 495
Clinical Features
Signs and symptoms depend on snake species, venom amount, bite location, and patient factors.
Pit Vipers / Crotalids
- Immediate burning pain at bite site
- Swelling within minutes, may progress for days
- Ecchymosis, petechiae, blebs, bullae at bite site (see photo below)
- Systemic: weakness, nausea, vomiting, sweating, perioral paresthesias, metallic taste, muscle fasciculations, hypotension
- Hematotoxicity: thrombocytopenia, hypofibrinogenemia, prolonged PT/PTT - risk of DIC
- Compartment syndrome: rare despite edema (most bites are subcutaneous)
- Some species (Mojave rattlesnake type A, Timber rattlesnake) cause neurotoxicity: cranial nerve dysfunction, paralysis, respiratory failure

Coral Snakes (Elapids)
- Often minimal local pain and swelling
- Neurotoxic effects delayed several hours but progress rapidly
- Ptosis, vertigo, paresthesias, fasciculations, slurred speech, dysphagia, drowsiness, proximal muscle weakness
- Death from respiratory failure
Elapids generally (cobras, mambas)
-
Predominantly systemic neurotoxic effects
-
Some (e.g., Indian cobra) may also cause extensive local tissue destruction
-
Rosen's Emergency Medicine, p. 811-812; Sabiston Textbook of Surgery, p. 834-836
Severity Grading
| Grade | Description |
|---|---|
| Grade 0 (Dry bite) | No envenomation; fang marks present but no symptoms |
| Grade 1 (Minimal) | Local swelling and pain only; no systemic effects |
| Grade 2 (Moderate) | Progressive swelling beyond bite site; mild systemic effects |
| Grade 3 (Severe) | Extensive swelling, significant systemic effects, lab abnormalities |
Factors associated with more severe envenomation: time to presentation >6 hours, age ≤12 years, adult snake, ptosis, coagulopathy on initial labs.
- Sabiston Textbook of Surgery, p. 919
Diagnosis
- Relies primarily on clinical history and physical examination
- Lab workup after pit viper bite: CBC, PT, PTT, fibrinogen levels
- Monitor for hematotoxicity (may persist 2 weeks post-treatment)
- In Australia/Papua New Guinea: swab the wound for venom identification kit - do NOT wash first
Management
Immediate First Aid
DO:
- Remove jewelry and tight clothing from the affected limb
- Immobilize and splint in functional position
- Limit exertion (especially walking for lower extremity bites)
- Get promptly to a medical facility with snakebite experience
- For elapid bites (Australia): apply pressure bandage at 55 mmHg between wound and heart to reduce systemic toxicity
DO NOT (avoidable/harmful treatments):
-
Do NOT incise the wound - historical incision-and-suction has been contraindicated since 1980; risks vessel, tendon, nerve damage and removes only a tiny amount of venom
-
Do NOT apply ice or heat
-
Do NOT apply tourniquets (especially for crotalid bites - concentrates venom, increases necrosis)
-
Do NOT massage the wound
-
Do NOT use electric shock (TASER, car battery, outboard motor) - historically attempted, no scientific basis
-
Do NOT try to catch the snake (risk of second bite; dead snakes can still bite reflexively)
-
Sabiston Textbook of Surgery, p. 872-893
Hospital Treatment
- Identify the species if possible - most important step in management
- Document puncture site location, fang mark distance (indicates snake size), local and systemic symptoms
- Cleanse wound gently (unless venom ID kit available)
- Serial vital signs guided by clinical response
- Labs: CBC, coagulation studies, fibrinogen, metabolic panel
- Antivenom is the mainstay of treatment
Antivenom
North American Crotalid antivenoms:
- CroFab (Crotalidae polyvalent immune Fab, ovine): ~$3,198/vial; 4-12 vials typical dose; half-life ~15 hours; requires refrigeration
- ANAVIP (Crotalidae immune F[ab']2, equine): ~$1,220/vial; starting dose 10 vials; half-life ~133 hours; room-temperature storage; less expensive
Adverse reactions:
- Immediate reactions (anaphylaxis): 6-14% with CroFab (much lower than older equine antivenom which caused ~50% anaphylaxis)
- Serum sickness (type III hypersensitivity): 13-16% with CroFab; treat with corticosteroids tapered over 7-14 days
- If anaphylaxis: stop infusion, give diphenhydramine + epinephrine + steroids, secure airway, volume resuscitation
Special populations:
-
Can be used in children as young as 14 months
-
Pregnancy: antivenom generally recommended when indicated - fetal loss rate up to 20% reported with snakebites globally, improved with antivenom
-
Sabiston Textbook of Surgery, p. 952-960
Medico-Legal / Forensic Notes
-
Snake venom is toxic only when injected, not when ingested (not absorbed by gastric mucosa)
-
However, blood of a bitten animal is poisonous if injected into a human
-
Venom retains potency for years in dried state
-
Snakes emerging from hibernation in early spring give the most dangerous bites
-
Nocturnal bites are more serious than daytime bites
-
Cobras and other "spitting snakes" can project venom 4-8 feet; if it reaches the eye, causes severe corneal and conjunctival inflammation (snake venom ophthalmia)
-
P C Dikshit Textbook of Forensic Medicine and Toxicology, p. 493-495
Summary: Snake bite envenomation is a medical emergency requiring rapid identification of the snake type, supportive care, and antivenom when indicated. The two main venom types - neurotoxic (Elapids) and hemotoxic/cytotoxic (Vipers) - dictate the clinical picture. Historical "treatments" like incision-and-suction, ice, and electric shock are actively harmful and must be avoided. Modern purified antivenoms (CroFab, ANAVIP) are far safer than older equine products and should be administered for significant envenomations.
Liver abcess
Finding Sources
Searching PubMed
"liver abscess" AND management
Reading File
Reading File
Reading File
Reading File
Reading File
Reading File
Reading File
Reading File
Loading Image
Reading File
Loading Image
I now have comprehensive data from multiple textbooks. Here is the full clinical overview:
Liver Abscess
A liver abscess is a collection of pus within the hepatic parenchyma. There are three main types: pyogenic (bacterial), amebic (parasitic), and fungal. The incidence is approximately 1 in 5,000 hospital admissions. Left untreated, pyogenic liver abscess carries a mortality of virtually 100%.
- Bailey and Love's Short Practice of Surgery 28th Edition, p. 2669
- Yamada's Textbook of Gastroenterology 7e
Types and Etiology
1. Pyogenic Liver Abscess (PLA)
The most common type in developed countries. Causative sources include:
| Route | Details | Frequency |
|---|---|---|
| Biliary obstruction | Cholelithiasis, malignancy, biliary instrumentation, post-transplant cholangiopathy | ~35% (most common) |
| Portal vein pyemia | Ascending infection from diverticulitis, appendicitis, IBD | ~20% |
| Trauma | Blunt or penetrating injury | Less common |
| Hematogenous | Systemic bacteremia via hepatic artery | Less common |
| Cryptogenic | No source identified | ~10% |
Organisms:
- Biliary origin: E. coli, Klebsiella spp., Enterococcus
- Enteric origin: Bacteroides fragilis, other anaerobes
- Cryptogenic: Klebsiella pneumoniae (monomicrobial) - associated with colon cancer; consider colonoscopy to rule out occult malignancy
- In USA: Streptococcus spp. are actually the most common isolated pathogens (population-based studies)
- Most PLAs are polymicrobial
Risk factors: Elderly, diabetes mellitus, biliary malignancy or instrumentation, immunosuppression, liver transplant, proton pump inhibitor use (possible mechanism: reduced gastric acid → bacterial overgrowth → biliary colonization), TACE for hepatocellular carcinoma.
- Current Surgical Therapy 14e, p. 103-111; Yamada's Textbook of Gastroenterology 7e
2. Amebic Liver Abscess (ALA)
Caused by Entamoeba histolytica (protozoan). Common worldwide but in the USA seen almost exclusively in male travelers (8:1 male:female) returning from endemic areas.
Pathophysiology:
-
Ingestion of E. histolytica cysts/trophozoites via fecally contaminated food or water
-
Intestinal mucosal invasion → trophozoites seed the liver via the portal venous system
-
Typically occurs 2-4 months after colonic amebiasis
-
Abscess contains necrotic hepatocytes in a characteristic thick brown fluid: "anchovy paste"
-
Current Surgical Therapy 14e, p. 191-196
3. Fungal Hepatic Abscess
Almost exclusively in immunocompromised patients: liver/hematopoietic stem cell transplant recipients, HIV, hepatobiliary malignancy.
Highest mortality of all types - nearly 50% die from disseminated infection; even with treatment, mortality ~20%.
Mostly caused by Candida spp.
Clinical Features
| Feature | Pyogenic | Amebic |
|---|---|---|
| Fever | 90% | 80% |
| RUQ pain | 60% | 60% |
| Jaundice | 50% | Less common |
| Pleuritic pain / right shoulder radiation | When diaphragm involved | When diaphragm involved |
| Anorexia, malaise, weight loss | Common | Common |
| Eosinophilia | Absent | Absent (despite being parasitic) |
Physical exam: RUQ tenderness, hepatomegaly, occasional jaundice.
Complications if untreated:
-
Rupture into peritoneum → purulent peritonitis (high mortality without surgery)
-
Rupture into right pleural space
-
Rare rupture into pericardium
-
Portal vein / hepatic vein thrombosis from local inflammation
-
Ipsilateral pleural effusion (>50% if abscess >10 cm)
-
Yamada's Textbook of Gastroenterology 7e; Current Surgical Therapy 14e
Laboratory Findings
| Test | Finding |
|---|---|
| WBC | Leukocytosis (90%) |
| Alkaline phosphatase | Elevated (80%) |
| Bilirubin | Elevated (50%) |
| Transaminases | Elevated (50%) |
| Blood cultures | Positive in >50% of PLAs |
| Amebic serology (IgG) | >90% sensitivity for ALA |
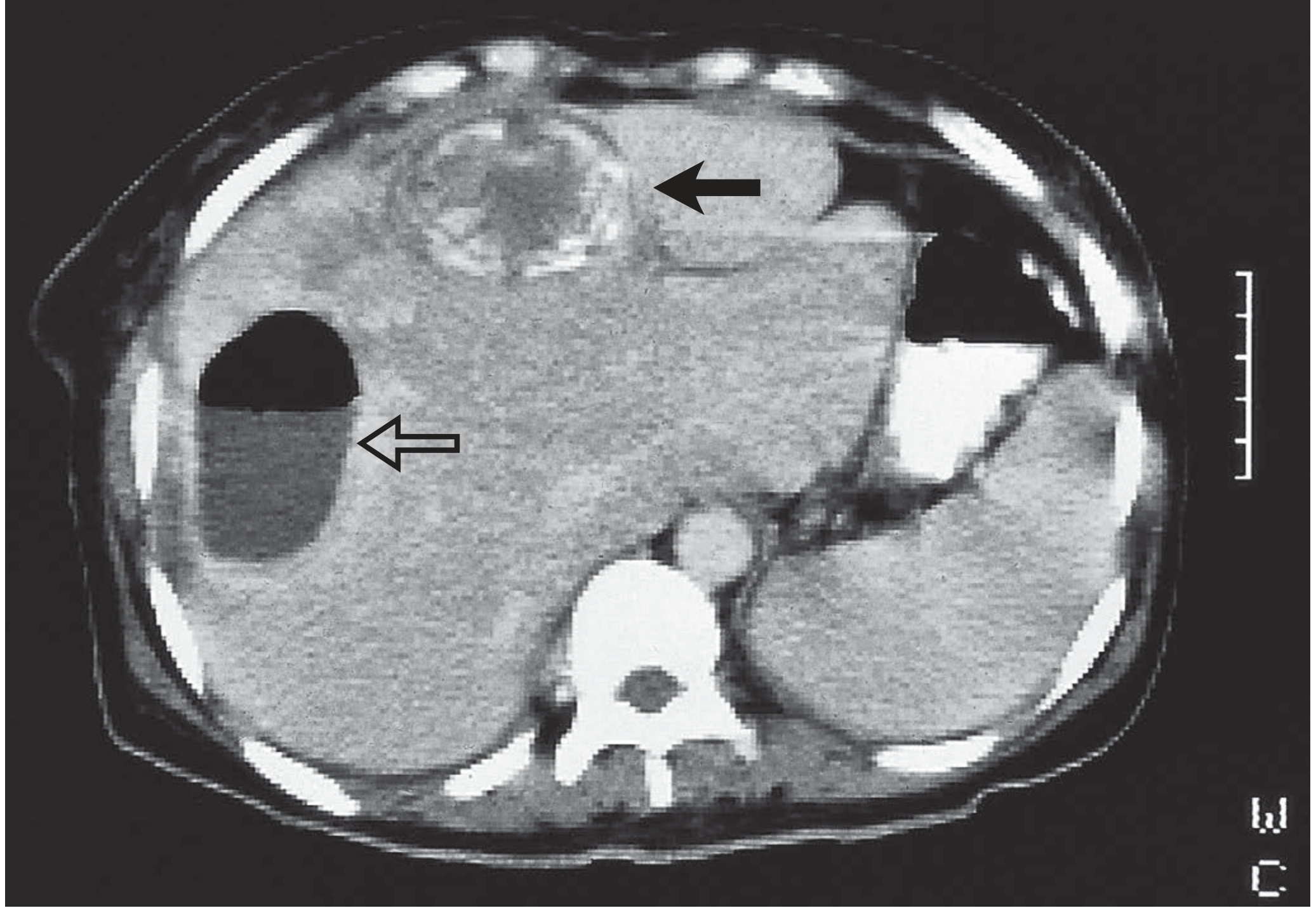
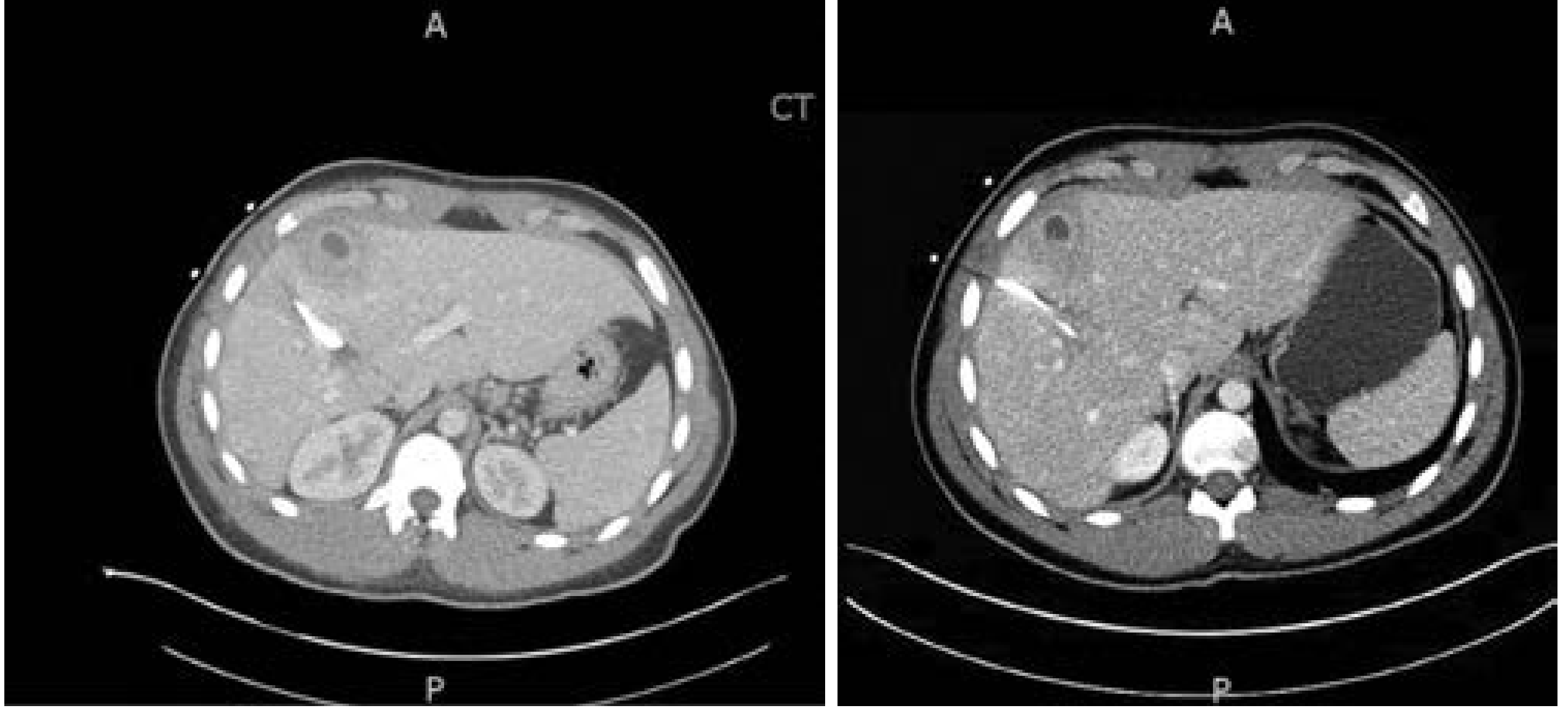
Imaging
Ultrasound
- First-line imaging in pediatrics and initial assessment
- Abscesses appear hypoechoic, often with internal echoes
- Can identify multiloculated cystic mass
- Less sensitive than CT overall
CT (with IV contrast) - Most sensitive
- Abscesses appear as hypoattenuating (low-density) lesions
- Peripheral rim enhancement - uncommon but specific
- May show loculations, air-fluid levels
- Identifies extrahepatic causes (appendicitis, diverticulitis)
- Multiple abscesses on imaging favor pyogenic over amebic etiology
Differential Diagnosis
- Hepatic malignancy with necrotic center
- Cholangitis / cholecystitis
- Right lower lobe pneumonia
- Hydatid (echinococcal) cyst
- Non-infected hematoma
- Perforated peptic ulcer
Distinguishing PLA vs. ALA
| Feature | Pyogenic (PLA) | Amebic (ALA) |
|---|---|---|
| Geography | Worldwide | Travel to endemic area |
| Demographics | Any age | Males 8:1, travelers |
| Organisms | Bacteria (polymicrobial) | E. histolytica |
| Number | Often multiple | Usually single (right lobe) |
| Aspirate | Purulent (bacterial) | "Anchovy paste" (brown) |
| Serology | Negative | Anti-amebic antibodies >90% sensitivity |
| Eosinophilia | Absent | Absent |
| Imaging differentiation | Not reliable | Not reliable |
Note: ALA and PLA cannot be reliably differentiated on imaging alone. Travel history and serology are key.
Treatment
Pyogenic Liver Abscess
Antibiotics
- Blood cultures and abscess cultures are essential (positive >50%)
- Empiric coverage must cover: streptococci, gram-negative enteric organisms, anaerobes
- Typical regimens: beta-lactam/beta-lactamase inhibitor combination, or 3rd-generation cephalosporin + metronidazole
- If liver transplant or risk of ESBL: consider carbapenems
- Metronidazole and clindamycin: excellent anaerobic coverage and abscess penetration
- 3rd-gen cephalosporins and aminoglycosides: effective against gram-negatives
- Duration: guided by clinical response and imaging resolution at 4-6 weeks
Percutaneous Drainage (standard of care)
- Recommended for all PLAs without evidence of rupture or concurrent intra-abdominal abscess
- Abscess >5 cm: percutaneous catheter drainage (superior to needle aspiration alone)
- Abscess >10 cm: may require multiple catheters
- Abscess <3 cm: aspiration alone (if technically feasible) to guide antibiotics
- Catheters remain until output is low and clear for several days
- Watch for bile in drains - indicates biliary communication → investigate with HIDA or MRCP/ERCP → may need sphincterotomy or percutaneous biliary drain
Surgical Drainage or Resection
-
Required in 10-20% of cases (failure of percutaneous approach)
-
Indications: large multiloculated abscesses, biliary tree communication, concurrent intra-abdominal abscess
-
Laparoscopy preferred; laparotomy for complex cases (e.g., simultaneous diverticulitis)
-
No evidence that partial hepatectomy is superior to simple surgical drainage + irrigation
-
Current Surgical Therapy 14e, p. 124-176
Amebic Liver Abscess
Antibiotics
- Oral metronidazole 500-750 mg TDS x 7-10 days - highly effective; >90% clinical improvement
- Must also treat intestinal reservoir to prevent recurrence:
- Oral paromomycin 10 mg/kg TDS x 7 days, OR
- Oral diiodohydroxyquin 650 mg TDS x 20 days
- Treatment duration is standardized (unlike PLA); imaging resolution may take months but is not needed to stop antibiotics
Drainage
- NOT routinely recommended for ALA - prospective studies show no benefit from early drainage
- Indicated only if no clinical response to antibiotics
- If failing standard ALA therapy: broaden antibiotics (cover for PLA), pursue percutaneous catheter drainage (consider bacterial superinfection)
Fungal Liver Abscess
- Same paradigm: antifungals + percutaneous drainage
- Empiric: Amphotericin B or an echinocandin (caspofungin or micafungin)
- Guided by culture data; duration determined by resolution on imaging
- Antifungal prophylaxis in transplant patients reduces risk
Recurrent / Refractory Abscess
- Recurrence rates: 12-38% depending on organism identification and whether diabetes is controlled
- More common when initial lesion was large, multiple, or with biliary communication
- Management: repeat aspiration → catheter drain → surgical drainage (laparoscopy preferred over laparotomy)
Outcomes / Prognosis
-
Mortality has improved dramatically with early diagnosis, antibiotics, and percutaneous drainage
-
Current mortality: 4-10%
-
Poor prognostic factors: diabetes mellitus, underlying malignancy, cirrhosis, abscess size >10 cm
-
Fungal abscess: highest mortality (~20-50%)
-
Current Surgical Therapy 14e, p. 179-181
Recent evidence note (PubMed 2025-2026): A 2025 review on Klebsiella pneumoniae liver abscesses (PMID 40607938) highlights evolving challenges with hypervirulent K. pneumoniae strains, which are increasingly associated with cryptogenic PLA and metastatic spread (endophthalmitis, meningitis) - particularly in diabetic patients from Asia. This is an emerging concern to keep in mind in clinical practice.
This is a shared conversation. Sign in to Orris to start your own chat.