Basics of trophoblastic diseases for neet pg
Reading File
Finding Sources
Finding Sources
Reading File
Reading File
Reading File
Reading File
Reading File
Reading File
Reading File
Reading File
Reading File
Finding Sources
Loading Image
Loading Image
Finding Sources
Loading Image
I now have all the content needed for a thorough NEET PG-focused answer. Let me compile it:
Gestational Trophoblastic Disease (GTD) - NEET PG Basics
GTD is a spectrum of tumors and tumor-like conditions arising from abnormal proliferation of placental trophoblasts. All types elaborate hCG to varying degrees and are broadly divided into benign (hydatidiform moles) and malignant (gestational trophoblastic neoplasia - GTN) forms.
- Robbins & Kumar Basic Pathology, p. 702
Classification of GTD
| Category | Condition |
|---|---|
| Benign | Complete Hydatidiform Mole, Partial Hydatidiform Mole |
| Malignant (GTN) | Invasive Mole, Gestational Choriocarcinoma, Placental Site Trophoblastic Tumor (PSTT), Epithelioid Trophoblastic Tumor (ETT) |
1. Hydatidiform Mole
Gross Appearance
The classic "bunch of grapes" uterine mass - swollen, translucent, thin-walled cystic villi:
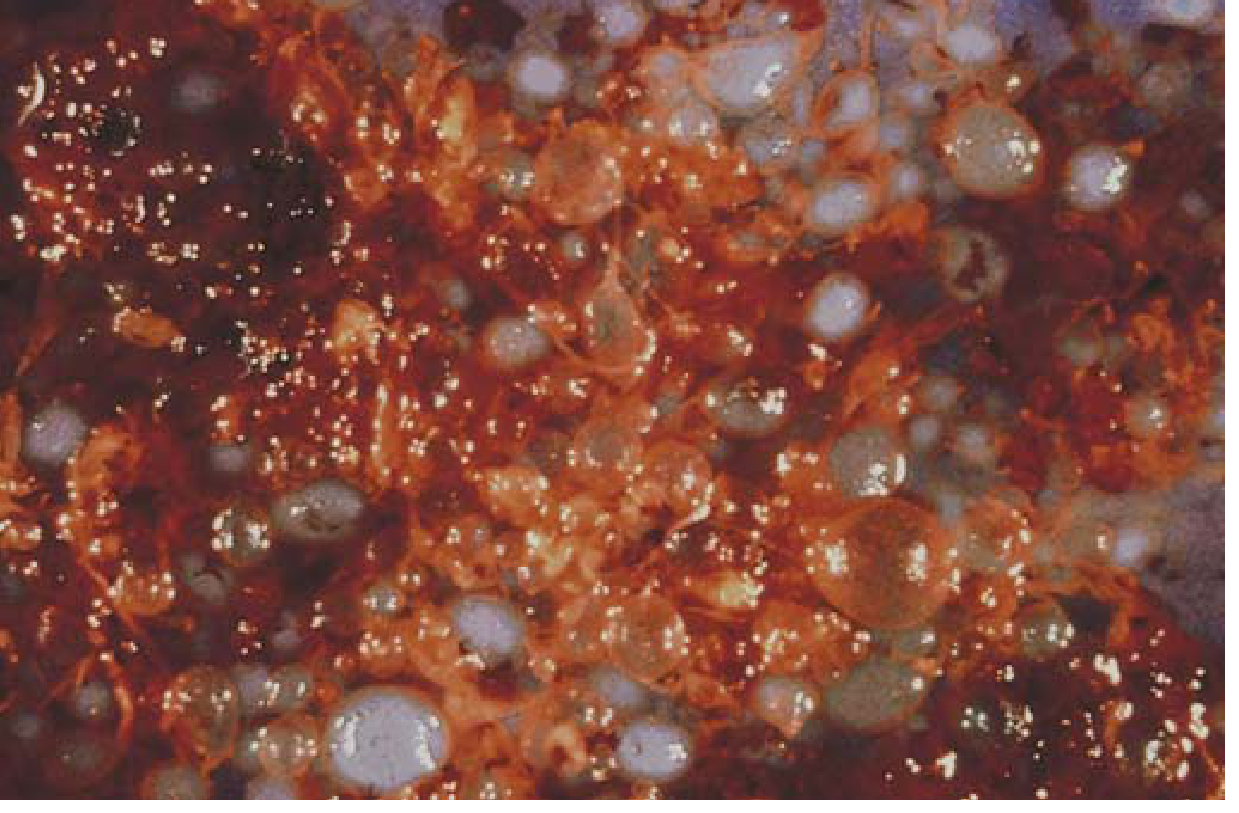
Complete hydatidiform mole - Robbins & Kumar Basic Pathology
Origin of Moles (Cytogenetics)
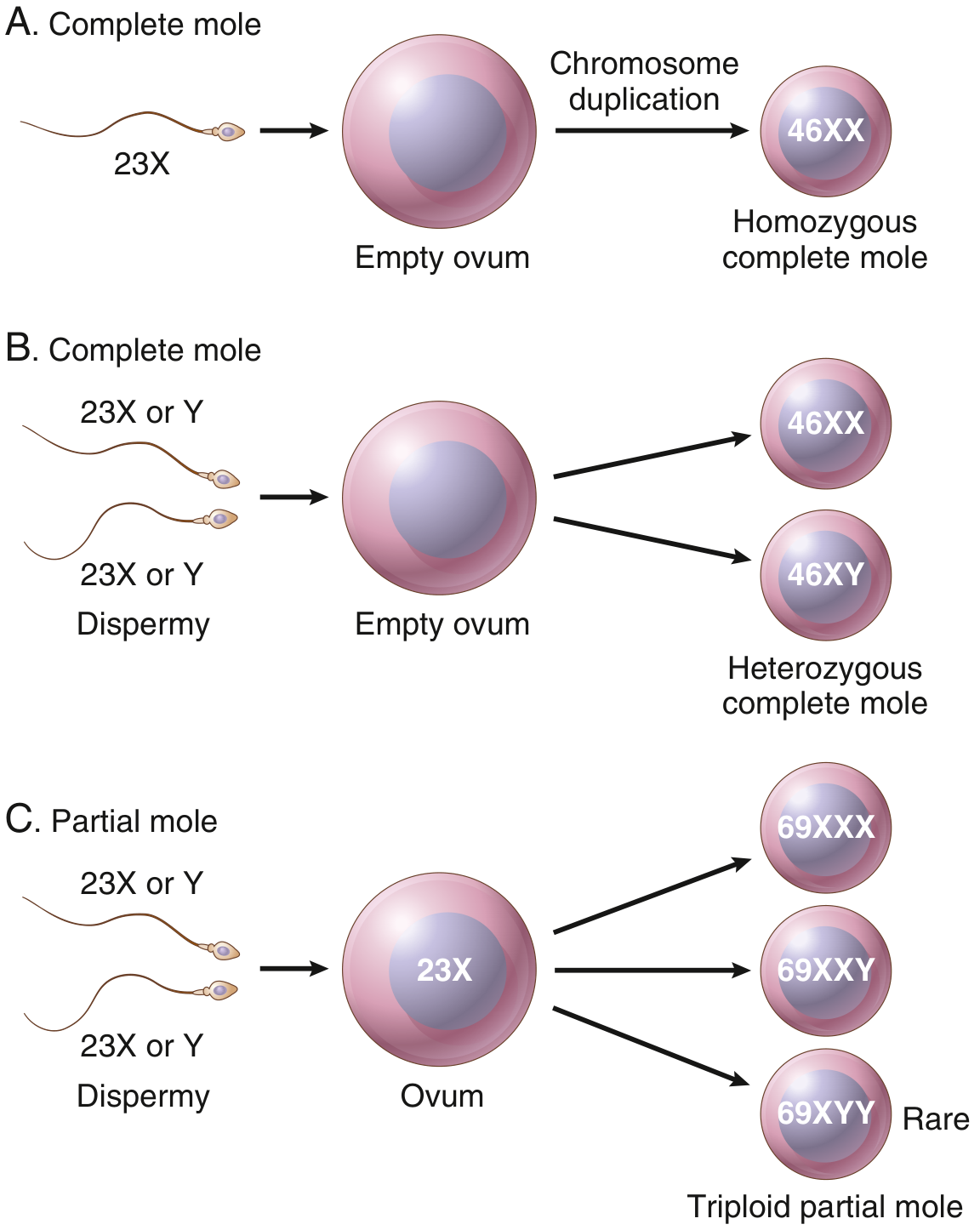
Origin of complete and partial moles - Robbins & Kumar Basic Pathology
Complete vs Partial Mole (HIGH-YIELD COMPARISON)
| Feature | Complete Mole | Partial Mole |
|---|---|---|
| Karyotype | Diploid - 46,XX (90%); rarely 46,XY | Triploid - 69,XXY (most common) |
| Chromosomal origin | All paternal (androgenic) - fertilization of empty ovum by 1 sperm (duplication) or 2 sperm | Maternal + paternal - normal ovum fertilized by 2 sperm |
| Fetal/embryonic tissue | Absent | Present (may have fetal parts, RBCs) |
| Villous edema | All villi (diffuse) | Some villi (focal) |
| Trophoblast proliferation | Diffuse, circumferential | Focal, slight |
| hCG levels | Very high (often >100,000 IU/L) | Less elevated or normal |
| Risk of choriocarcinoma | ~2.5% | Rare |
| Risk of persistent GTN | 15-20% | 1-5% |
| Scalloping of villi | Absent | Present |
| Trophoblastic stromal inclusions | Absent | Present |
- Robbins & Kumar Basic Pathology, p. 702-703; Berek & Novak's Gynecology, Table 41-1
Risk Factors for Molar Pregnancy
- Age extremes: <20 years (7x risk for complete mole) and >40 years (2-10x risk)
- Women >50 years: 1 in 3 pregnancies is molar
- Low dietary carotene (vitamin A precursor) and animal fat
- Previous molar pregnancy
- Partial moles: linked to oral contraceptive use, irregular menstruation
Clinical Features of Complete Mole
- "Too large for dates" uterus (most classic presentation)
- Bleeding in first trimester (brownish discharge)
- Absent fetal heart sounds
- Markedly elevated hCG (sometimes >100,000 IU/L)
- Preeclampsia before 20 weeks (occurs in ~27%) - important clue
- Hyperemesis gravidarum (~25%) - due to high hCG
- Hyperthyroidism (~7%) - hCG has TSH-like activity; can precipitate thyroid storm during evacuation
- Theca lutein cysts (bilateral, multilocular) - due to high hCG stimulation of ovaries
- Trophoblastic embolization - respiratory distress (rare)
Clinical Features of Partial Mole
- Often missed clinically, diagnosed as missed/incomplete abortion
- Uterus is small or appropriate for dates
- hCG may be normal or slightly elevated
Diagnosis
- Ultrasound: "Snowstorm pattern" in complete mole (classic finding)
- Serum beta-hCG
- Histopathology of evacuated tissue
Treatment
- Suction evacuation and curettage (treatment of choice)
- Hysterectomy - if no desire for fertility
- No prophylactic chemotherapy routinely
- Post-evacuation hCG monitoring: Weekly until undetectable, then monthly for 6-12 months
- Contraception for 6-12 months during hCG surveillance
2. Gestational Trophoblastic Neoplasia (GTN)
GTN includes invasive mole, choriocarcinoma, PSTT, and ETT. It is diagnosed by rising or plateauing hCG after molar evacuation (or new lesion after any pregnancy).
Invasive Mole
- Complete mole that invades the myometrium (retains hydropic villi - KEY feature distinguishing it from choriocarcinoma)
- Can penetrate uterine wall - risk of hemorrhage
- Villi may embolize to lungs/brain but do not metastasize in the true sense
- Responds well to chemotherapy
- Robbins & Kumar Basic Pathology, p. 703
Gestational Choriocarcinoma (HIGH-YIELD)
Origins (memorize these percentages):
- 50% from complete hydatidiform moles
- 25% from prior abortions
- ~22% from normal pregnancies
- Remainder from ectopic pregnancies
Histology (distinctive - NO VILLI):
- Composed of anaplastic cytotrophoblasts + syncytiotrophoblasts
- No chorionic villi formed (vs invasive mole which has villi)
- Hemorrhagic, necrotic uterine mass
- Abundant mitoses
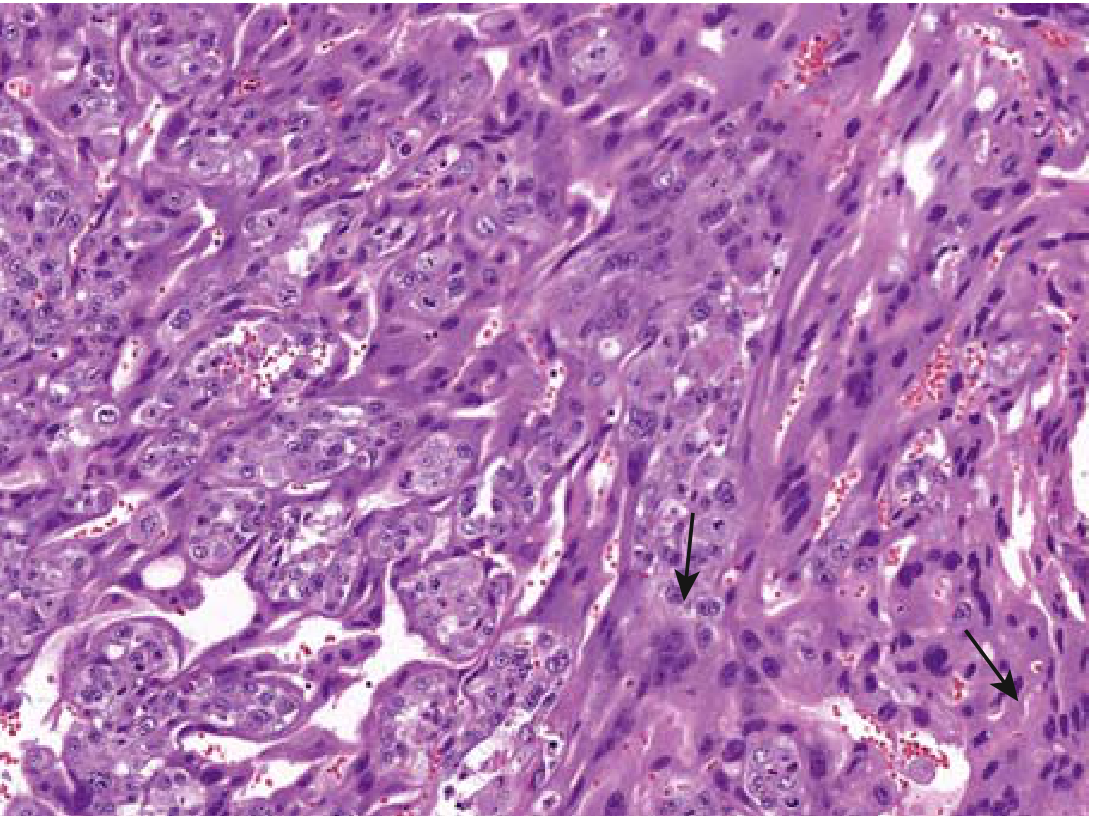
Choriocarcinoma - both cytotrophoblast and multinucleate syncytiotrophoblast (arrows). Robbins & Kumar Basic Pathology
Metastases (spread is hematogenous, NOT lymphatic):
- Lungs: 50% (most common)
- Vagina: 30-40%
- Brain, liver, kidneys
Key fact: Despite widespread metastases, gestational choriocarcinoma is remarkably sensitive to chemotherapy - nearly 100% cure rate even with distant metastases.
Placental Site Trophoblastic Tumor (PSTT)
- <2% of GTN
- Arises from intermediate (extravillous) trophoblasts (not cytotrophoblasts/syncytiotrophoblasts)
- Low hCG but high human placental lactogen (hPL) - key marker
- Usually diploid (XX karyotype)
- Arises months after normal pregnancy (not usually after moles)
- Not sensitive to chemotherapy (unlike other GTN)
- Treatment: Hysterectomy (surgery is preferred)
- Poor prognosis once extrauterine spread occurs
3. FIGO Staging of GTN
| Stage | Description |
|---|---|
| I | Confined to uterus |
| II | GTN involving pelvis and vagina |
| III | GTN extending to lungs |
| IV | All other metastatic sites (brain, liver, kidney) |
4. WHO Prognostic Scoring System (FIGO/WHO Risk Score)
Used to categorize GTN into low-risk (score ≤6) and high-risk (score ≥7):
| Prognostic Factor | Score 0 | Score 1 | Score 2 | Score 4 |
|---|---|---|---|---|
| Age | <40 | ≥40 | - | - |
| Antecedent pregnancy | Mole | Abortion | Term | - |
| Interval from index pregnancy (months) | <4 | 4-6 | 7-12 | >12 |
| Pre-treatment hCG (IU/L) | <10³ | 10³-10⁴ | 10⁴-10⁵ | >10⁵ |
| Largest tumor size (including uterus) | - | 3-4 cm | ≥5 cm | - |
| Site of metastases | Lung, vagina | Spleen, kidney | GI tract | Brain, liver |
| Number of metastases | - | 1-4 | 5-8 | >8 |
| Previous failed chemotherapy | - | - | Single drug | ≥2 drugs |
- Berek & Novak's Gynecology
5. Management of GTN
Low-Risk GTN (FIGO score ≤6)
- Single-agent chemotherapy: Methotrexate (MTX) or Actinomycin D
- Remission rate ~100% for non-metastatic disease
- Methotrexate is first-line; Actinomycin D used if MTX fails or in liver disease
High-Risk GTN (FIGO score ≥7)
- Combination chemotherapy: EMA-CO regimen (Etoposide, Methotrexate, Actinomycin D + Cyclophosphamide, Oncovin/Vincristine)
- Surgery for complications or drug-resistant disease
- Radiation occasionally for brain/liver metastases
PSTT and ETT
- Surgery (hysterectomy) is primary treatment
- Less responsive to chemotherapy compared to other GTN
Quick NEET PG Memory Points
| Point | Fact |
|---|---|
| Tumor marker for GTD | beta-hCG (all types) |
| PSTT marker | hPL (human placental lactogen) |
| Classic presentation | "Too large for dates" + high hCG + snowstorm USG |
| Mole with no fetus | Complete mole |
| Mole that can have a fetus | Partial mole |
| No chorionic villi | Choriocarcinoma |
| Most common site of met in choriocarcinoma | Lung |
| Choriocarcinoma spread | Hematogenous (not lymphatic) |
| Treatment of invasive mole | Chemotherapy (MTX) |
| Treatment of PSTT | Hysterectomy |
| Low-risk GTN chemo | Methotrexate (single agent) |
| High-risk GTN chemo | EMA-CO |
| Preeclampsia before 20 weeks | Think mole! |
| Hyperthyroidism in mole | hCG has TSH-like activity |
| Contraception after mole | 6-12 months (to monitor hCG) |
| Risk of choriocarcinoma - complete mole | ~2.5% |
| Risk of choriocarcinoma - partial mole | Rare |
Sources: Robbins & Kumar Basic Pathology (9th ed.), pp. 702-704 | Berek & Novak's Gynecology, Chapter 41
This is a shared conversation. Sign in to Orris to start your own chat.